
Abstract
To promote the informatization management of hospital human resources and advance the application of hospital information technology. The application of deep learning (DL) technologies in health care, particularly in hospital settings, has shown significant promise in enhancing decision-making processes for nurse staff. Utilizing a hospital management decision support system based on data warehouse theory and business intelligence technology to achieve multidimensional analysis and display of data. This research explores the development and implementation of a DL-Based Clinical Decision Support System (DL-CDSS) tailored for nurses in hospitals. DL-CDSS utilizes advanced neural network architectures to analyze complex clinical data, including patient records, vital signs, and diagnostic reports, aiming to assist nurses in making informed decisions regarding patient care. By leveraging large-scale datasets from Hospital Information Systems, DL-CDSS provides real-time recommendations for treatment plans, medication administration, and patient monitoring. The system’s effectiveness is demonstrated through improved accuracy in clinical decision-making, reduction in medication errors, and optimized workflow efficiency. The system analyzes and displays nurses data from hospitals in terms of quantity, distribution, structure, forecasting, analysis reports, and peer comparisons, providing head nurses with multilevel, multiperspective data mining analysis results. Challenges such as data integration, model interpretability, and user interface design are addressed to ensure seamless integration into nursing practice, also concludes with insights into the potential benefits of DL-CDSS in promoting patient safety, enhancing health care quality, and supporting nursing professionals in delivering optimal care.
Introduction
Clinical Decision Support Systems (CDSSs) are designed to enhance health care delivery by augmenting medical decisions with targeted clinical knowledge, 1 patient-specific information, and other health data. 2 A traditional CDSS involves software that aids clinical decision-making by matching individual patient characteristics to a computerized clinical knowledge base, providing patient-specific assessments or recommendations to the clinician for informed decision-making. 3 The inception of computer-based CDSS dates back to the 1970s, when integration issues, time-intensive operations, and academic limitations were prevalent. Ethical and legal concerns regarding the use of computers in medicine, physician autonomy, and accountability for system recommendations with imperfect “explainability” were also raised. 4 Today, CDSS have evolved to integrate seamlessly with electronic health records (EHRs) and computerized provider order entry systems, utilizing web applications, and various devices such as desktops, tablets, smartphones, and wearable health technology. Clinical decision support (CDS) systems are pivotal in modern health care, leveraging evidence-based guidelines to enhance clinical practice. 5 These systems empower clinicians with timely, personalized information, thereby improving decision-making quality, reducing errors, and fostering shared decision-making (Kwan et al., 2020). By integrating population-level evidence with individual patient characteristics, CDS systems offer tailored recommendations across diverse care settings, integrating tools like BMJ Best Practice and seamlessly embedding them within EHRs and digital workflows. 6
With the exponential growth of health care data and advancements in computing power, CDS systems capitalize on statistical methods to analyze vast datasets, predicting, and optimizing clinical decisions. 7 EHRs facilitate the capture of comprehensive clinical data, enabling CDS systems to apply evidence-based insights directly to patient records, thereby guiding personalized care decisions. Recognized as a hallmark of digitally mature health services (Orenstein et al., 2019), CDS systems are already integral to clinical workflows, functioning as calculators, alerts, and educational resources within EHRs. 8 Despite their proven efficacy, widespread adoption of CDS systems faces barriers, including variability in implementation and the risk of disrupting established clinical workflows, potentially leading to alert fatigue. 9 Successful integration demands alignment of technological capabilities with clinical workflows and stakeholder needs, necessitating collaborative efforts, and codesign strategies. 10 Digital leaders play a crucial role in driving the adoption of CDS systems across health care organizations, facilitating their integration into daily practice. This implementation guide serves to unify understanding and promote best practices in deploying CDS systems, supporting both digital and clinical leaders in navigating their digital transformation journey. 11 It highlights potential benefits, addresses implementation challenges, and underscores the importance of evidence-based approaches in optimizing health care delivery. 12
Historically, the governance of health care delivery and organization has predominantly resided within the purview of physicians. Despite the enduring resilience of medical dominance, “decision-rich” domains such as pharmacotherapy, initiation of critical care outreach in acute settings, nutritional management, and rehabilitation planning provide opportunities for nonmedical professionals to formally influence health care delivery, patient experience, and clinical outcomes. 13
In addition to formalized medical decisions like diagnosing, prescribing, or prognosticating, the realpolitik of health care relies heavily on an array of informal judgments, decisions, and negotiated positions among diverse health care professionals with fluid and overlapping roles. Technological advancements have increasingly infiltrated health care decision-making, offering support, information, and recommendations to augment professional judgment. 14
This discourse centers on the contributions of nurses, midwives, and allied health professionals (NMAHPs). Their roles, demographic profiles, educational backgrounds, and socio-economic standings often diverge from those of physicians, yet they are integral to a complex, dynamic, and critically negotiated division of labor in health care. Authority within this framework partially derives from the capacity to exercise clinical judgment, engage in clinical reasoning, and shape or make decisions. 15 Assuming that health care work is rooted in and reflective of reasoned judgments and decisions, it is evident that different professionals in multidisciplinary teams encounter distinct uncertainties, judgments, and decisions. Consequently, the support required to navigate these uncertainties may also vary.
Research on the decision-making processes of NMAHPs remains relatively sparse compared with the extensive studies on physicians and medical reasoning. However, since the 1960s, prominent decision scientists have examined nursing decisions, and researchers have categorized and analyzed various types of “nursing” decisions. 16 Some scholars argue that there is no intrinsic reason to regard nurses—and by extension, other health professionals—as having a unique decision-making cognition, even though their decisions may appear distinct when contextualized. Others have extended established descriptive and prescriptive theories of professional decision-making to encompass forms of knowledge and cognition, such as “reflection-in-action,” associated with specific professional groups, particularly nurses.
Classification and types of CDSS
CDSSs are categorized based on intervention timing and delivery method (active or passive). They are frequently classified as knowledge-based or nonknowledge-based. Knowledge-based systems use rules (IF-THEN statements) derived from literature-based, practice-based, or patient-directed evidence, while nonknowledge-based systems leverage artificial intelligence (AI), machine learning (ML), or statistical pattern recognition, often facing challenges such as “black box” logic and data availability. 17
Government endorsement and global adoption
The U.S. Government’s Health and Medicare acts have endorsed CDSS, incentivizing their integration into EHRs. As of 2013, 41% of U.S. hospitals with an EHR also had a CDSS, increasing to 40.2% with advanced CDS capability by 2017. Internationally, Canada, England, Denmark, Estonia, and Australia have shown promising adoption rates and significant health care IT investments.
Functions and benefits of CDSS
CDSS functionalities are vast, encompassing diagnostics, alarm systems, disease management, prescription and drug control, and more. They manifest as computerized alerts, reminders, guidelines, order sets, patient data reports, documentation templates, and clinical workflow tools. Each function offers potential benefits and challenges, which will be explored in detail throughout this review.
Enhancing nursing practice with CDSS
Nursing in High-Demand Environments
Nurses are crucial to patient safety and clinical duties, often managing numerous patients per shift. In Taiwan, for example, nurses face significant workload stress, leading to high resignation rates among junior staff. 18 Major reasons include lack of clinical experience, poor coordination with colleagues, and work overload affecting daily life. These stressors highlight the importance of developing efficient nursing information systems to support nurses in high-demand environments.
The Nursing Process and Decision-Making
The nursing process involves multiple stages: assessment, diagnosis, care target setting, treatment application, and evaluation. Nurses must integrate physiological, psychological, spiritual, and social views with their knowledge and experience to make informed decisions. However, time constraints, stress, and workload can impact the accuracy and completeness of nursing diagnoses and records. 19
CDSS in Nursing Practice
A decision support system (DSS) assists in making relevant decisions by leveraging databases and AI to facilitate decision-making. DSS can provide quick and appropriate suggestions for various clinical symptoms and test results, supporting health care providers with valuable information for better decision-making. 20 The main function of DSS is to support users with relevant information, based on the users’ professional knowledge and experience.
Artificial intelligence in nursing informatics
Deep Learning Technology and Nursing Informatics
Nursing informatics aims to create a patient-centered recording model supported by AI technology, facilitating nursing care and establishing clinical nursing guidance for various patients. AI technology explores and designs machines that simulate human behaviors, demonstrating human-like intelligence in thinking and operations. Artificial neural networks, such as back-propagation neural networks (BPN), are popular AI models used to enhance decision-making accuracy and consistency in medical contexts. 21
DL Applications in Medical Decision-Making
AI techniques, including BPNs and adaptive-network-based fuzzy inference systems, have been applied to various medical decision-making processes. These techniques enhance accuracy in triage and acuity scale determination, forecast discharge planning services, and classify diseases such as diabetes and metabolic syndromes. 22 AI systems provide valuable support for medical staff, assisting in clinical decisions and preemptive disease treatment.
CDS Systems and AI technology represent significant advancements in health care delivery and nursing practice. By integrating targeted clinical knowledge, patient information, and AI capabilities, CDSS enhance decision-making processes, improve patient outcomes, and support nursing staff in high-demand environments. 23 Continued research and development in CDSS and AI will further optimize health care delivery and address the challenges faced by clinicians and nurses worldwide.
The Evolution of Hospital Informatization in China
Over the past two decades, hospital informatization in China has undergone rapid development. Information technology has seamlessly integrated into various aspects of hospital management, including medical care, nursing, laboratory testing, finance, and administration. This integration has become a pivotal strategy for enhancing hospital management. Human resources management, once characterized by simple functional roles and traditional methods, has evolved into a sophisticated department utilizing electronic information systems. 24 Hospitals, being hubs of knowledge and technology, are increasingly competing in areas of technology, equipment, and service. Consequently, human resources management has become a central focus for hospital administrators. 25
Health care system reforms and informatization
China’s health care system reform has brought about significant changes, emphasizing hospital management and the adoption of electronic medical records (EMRs). 26 These reforms promote hospital informatization and necessitate advancements in human resources management. Modern challenges in hospital human resources management include outdated management models, low efficiency, lack of performance management, insufficient strategic planning, and inadequate competitive awareness. 27 Furthermore, issues such as fragmented data sources, lack of uniform standards, and low data utilization efficiency pose significant obstacles to hospital informatization.
The imperative for intelligent tools
In this new era, leveraging intelligent tools to modernize, standardize, and scientifically manage hospital operations is crucial. The integration and mining of vast data resources to provide decision support for hospital human resources management is a critical area of exploration. 28 Enhancing the informatization of human resources management and hospital information application is paramount.
Deep Learning-Based decision support for nurse staff
Transforming Nursing with Decision Support Systems
DSSs are intelligent computer application systems designed to assist decision-makers by leveraging data, models, and knowledge in a human-machine interactive manner. In this study, we establish a deep learning (DL)-based DSS specifically tailored for nursing staff. 29 This system aims to enhance the efficiency and effectiveness of nurse staff by providing real-time, data-driven insights, and recommendations.
System Architecture and Data Processing
The system architecture, as illustrated in Figure 1, involves the Extract-Transform-Load (ETL) process. Here, data undergoes extraction, transformation, and loading into predefined data warehouse (DW) models. Subsequently, online transaction processing (OLTP) and online analytical processing (OLAP) technologies associated with data warehousing are employed. OLTP facilitates immediate data transmission to the processing center for real-time handling, enabling users to respond promptly to data. 30 OLAP acts as the system’s front-end display tool, utilizing advanced analysis
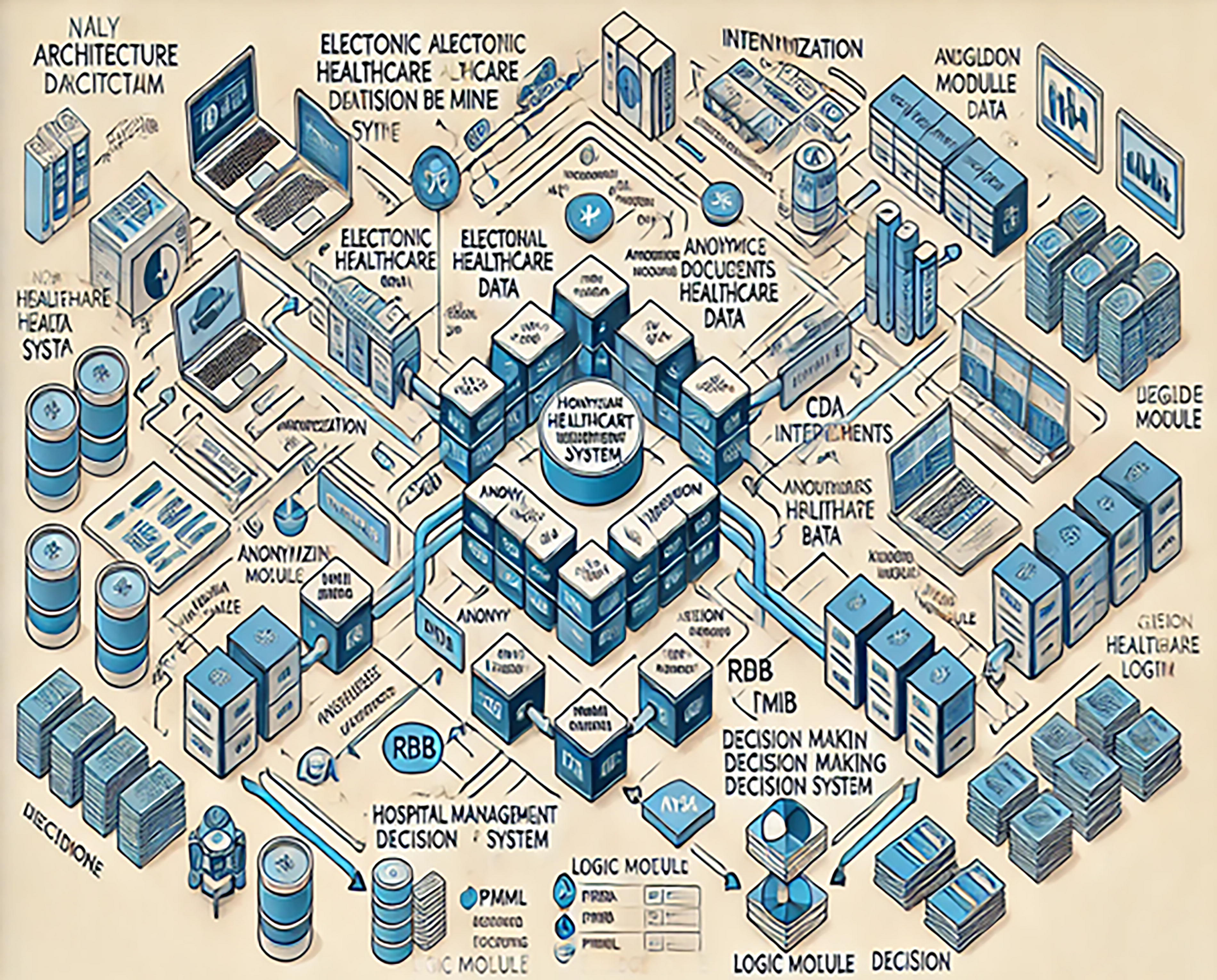
Analysis architecture of hospital management DSS. This figure illustrates the overall structure of the DSS for hospital management, highlighting key components such as data input sources, analysis modules, and output decision-making processes. DSS, decision support system.
Implementation
Robust integration platform for nurse staff HR data using DW technology
DW technology serves as the cornerstone for DSSs, offering a subject-oriented, integrated, time-variant, and nonvolatile collection of data. 31 Creating a subject-oriented DW involves consolidating nurse staff human resources data scattered across various business systems into centralized storage units. 32 This setup allows for comprehensive analysis and multidimensional observation of data, with the human resources subject area structured around dimensions such as data periods (year, quarter, month), departments, education levels, genders, professional qualifications, personnel counts, and various personnel compositions.
The DW provides a stable integration platform for nurse staff human resources management, characterized by:
Subject Orientation: Excluding data irrelevant to decision-making. Integration and Sharing: Aggregating nurse staff human resources data from diverse sources. Data Persistence: Ensuring data continuity over time. Interoperability: Facilitating cross-subject data linkage.
Presently, hospital human resources information management is lagging, with many hospitals managing nurse staff records through isolated departmental archives. 33 The current level of human resources informatization is confined to standalone management software, impeding information sharing, timely updates, and interdepartmental coordination. 34 Under the human resources subject area in the DW, data are cohesively organized, eliminating dispersion. 34 Additionally, subject interoperability allows the linkage of nurse staff human resources data with themes such as medical services and financial income, enabling thorough analyses of departmental performance and medical service efficiency. 35
Ensuring data quality control
Data quality is pivotal for generating reliable analytical outcomes. To maintain accuracy, all data analyzed by the hospital management DSS emanate from a centralized data center within the DW. By decoupling data resources from business systems and integrating them within the data center, the DW remains unaffected by changes in operational systems. 36 All data from hospital-wide business systems must be channeled into the data center for analysis, thereby overcoming the challenges of dispersed data sources and information silos.
To integrate data from various business systems, this study establishes standardized specifications for data exchange interfaces in provincial hospital business systems, based on statutory reporting forms. 36 For instance, data from Hospital Information Systems (HIS) undergoes an ETL process for data cleansing before entering the data center, ensuring data quality at the entry point. Additionally, advanced Business Intelligence (BI) data collection tools enforce strict audit criteria, strengthen data correlations, and automate indicator generation, thereby rigorously controlling data quality from its source and enhancing the overall quality of hospital medical data. 37
This rigorous approach ensures that nurse staff data are accurately captured and maintained, providing a reliable foundation for decision-making processes that affect nurse staffing, training, and overall hospital operations. 38
Analysis and visualization of hospital workforce data
In this research, we utilized data from a specific hospital, collected through the mandated “Basic Information Survey Form for Health Human Resources.” These data formed the basis for our DL-based DSS, tailored specifically for nurse staff and broader hospital workforce management. As depicted in Figure 2, the system provides a comprehensive analysis and visualization of human resources data across five key aspects: workforce quantity, distribution, structure, forecasting, analysis reports, and peer comparisons. Notable features of the system include:
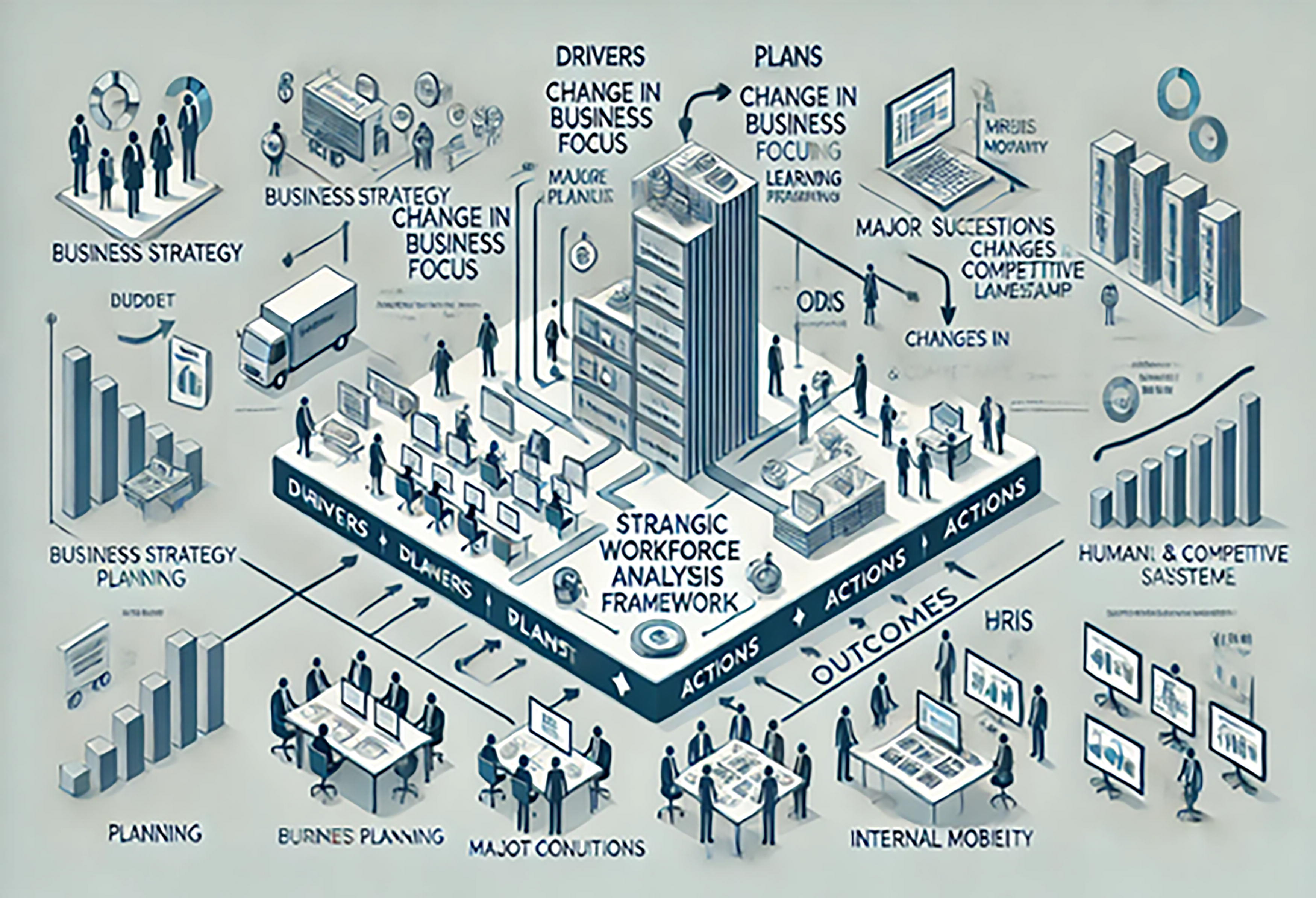
Hospital workforce analysis framework. This framework outlines the methodologies used to analyze the hospital workforce, including factors such as staffing levels, department roles, and performance metrics.
Integration of statistical tables and various graphical results.
Support for ad-hoc queries with customizable analysis tables.
Capability for drill-down data exploration.
Users can select different dimensions such as time periods (year, quarter, month), departments, and personnel categories to create multidimensional displays tailored to their needs. Detailed summaries allow for deep data exploration from department-level views down to individual nurse staff, enhancing the depth of queries. 39
Yale New Haven Hospital (YNHH) nursing was an early adopter of the Rothman Index, a sophisticated tool designed to reflect patient acuity and risk. 40 Director of Nursing Professional Practice Dr. Judith Hahn, Strategic Analytics Innovation Scientist Dr. Joan Rimar Sr., and Clinical Informatics Manager Leslie Hutchins have illuminated the complexities involved in integrating new algorithms into nursing and interprofessional practice. 41 Hutchins emphasized that the goal of YNHH’s technological implementations is “providing the right advisory, at the right time, to utilize meaningful information for achieving desired patient outcomes. 42 ”
The Rothman Index calculates scores using EMR data from 26 variables, including 11 nursing assessment metrics, and displays these scores graphically. Initially, the introduction of the Rothman Index faced skepticism regarding its validity and reliability in producing actionable results. At first, there was a lack of peer-reviewed literature to persuade nurses and other clinicians that the index would significantly improve patient care. However, recent research indicates that the performance of the Rothman Index is positively influenced by nursing assessment data, underscoring the substantial potential for nurses to impact patient outcomes.
At YNHH, specialized nurse SWAT teams utilize the Rothman Index to identify patients at risk. These teams, composed of experienced nurses trained in critical care, advanced cardiovascular life support, and trauma care, now receive immediate warning notifications on their mobile phones when the index signals patient deterioration. 43 Upon receiving an alert, the SWAT team reviews the EMR, assesses the patient if necessary, and collaborates with clinical nurses and medical staff to address pertinent aspects of care. SWAT nurses describe their role as serving as “a second set of eyes. 44 ”
The data used to generate the Rothman Index scores are derived from routine nursing documentation, and timely input of nursing assessment data is crucial for the real-time updating and accuracy of the index. For clinicians to embrace and consistently use the index, they often need an “a-ha” moment where they realize the tangible impact of the data on patient care.
Workforce Quantity and Distribution
Effective human resources management requires ongoing adjustment of the workload-to-personnel ratio. Our DL-based DSS analyzes total health personnel, departmental distributions, and year-over-year changes in personnel numbers. 45 This approach provides an overarching view of hospital staffing trends, along with detailed insights into departmental and category-specific staffing configurations. For example, Table 1 and Figure 3 demonstrate the 2013 distribution of health technical personnel, managerial staff, technical support staff, and other technical personnel according to health personnel standards. Users can flexibly query and display information on personnel quantity and distribution across various dimensions such as time periods, departments, and personnel categories, facilitating efficient staffing decisions through enriched graphical displays, multidimensional queries, and data drill-down features.
Hospital health personnel composition (%). A pie chart depicting the distribution of various health personnel types (doctors, nurses, administrative staff, etc.) in the hospital, expressed as percentages.
Composition of health personnel in 2013
Note: Data sourced from annual reports.
Workforce Structure
Hospitals employ a diverse range of technical professionals engaged in complex tasks, requiring precise management of job classifications, organizational structure, and position design to ensure operational efficiency and cost-effectiveness. The DL-based DSS not only allocates personnel across departments but also ensures the rationality of various personnel structures, such as age, education, professional titles, and gender ratios, to support the hospital’s ongoing human resources needs. As illustrated in Figure 2, this study analyzes and displays the hospital workforce structure based on the rationality of educational backgrounds, ages, genders, and professional titles to facilitate effective personnel management.
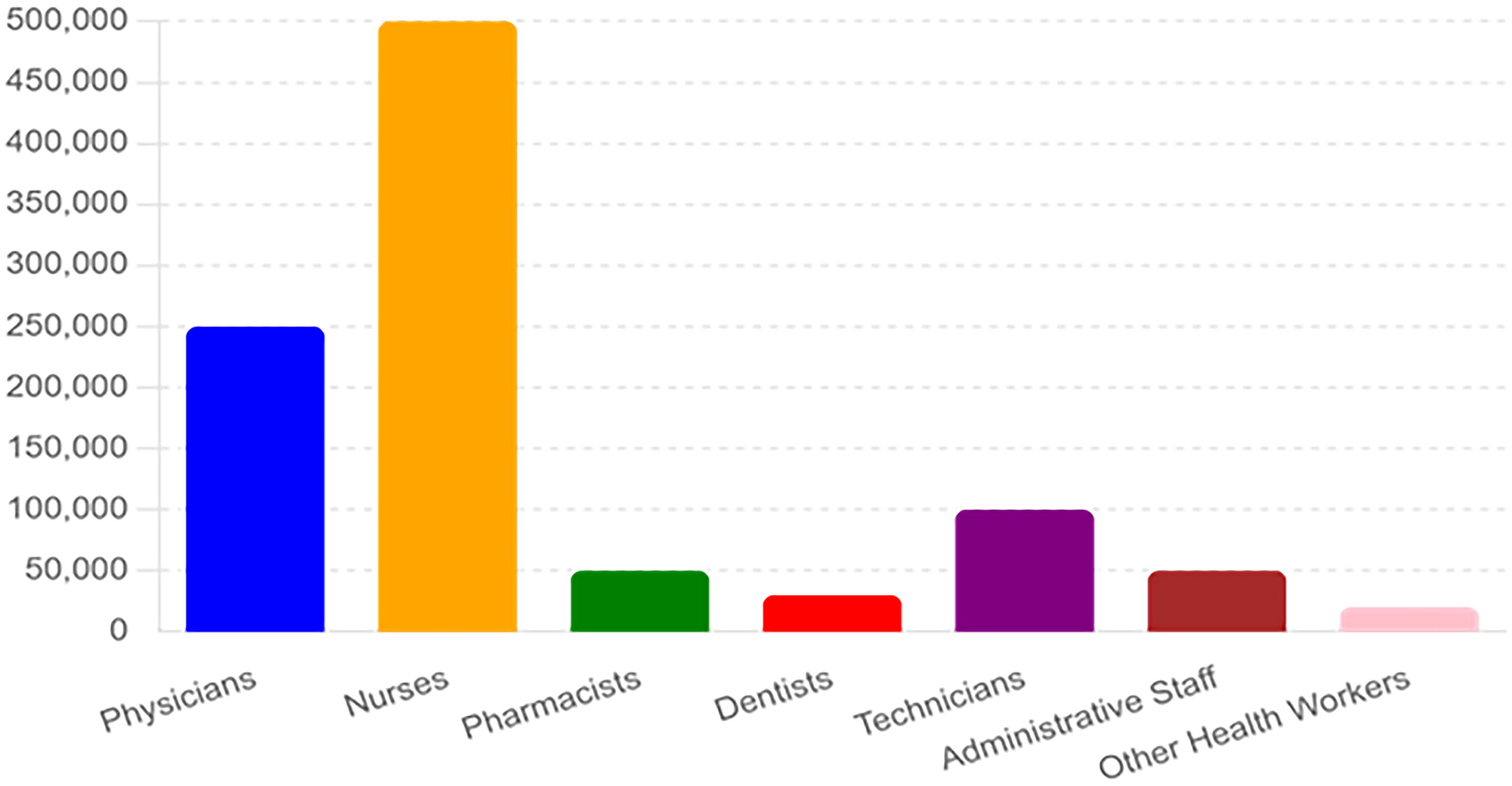
Figure 4 shows the employment status of hospital health personnel professional titles in 2013. Users can access information on personnel structures from different perspectives through multidimensional queries, 46 assisting decision-makers in improving organizational structures in line with industry standards. This approach ensures balanced labor allocation, prevents issues like personnel imbalances and organizational inefficiencies, and effectively enhances labor productivity. 47

Employment status of hospital health personnel professional titles in 2013. This bar chart shows the employment status (e.g., full-time, part-time, contractual) of hospital health personnel across different professional titles in the year 2013.
Our system is designed to assist in making informed decisions regarding nurse staff and other hospital personnel, ensuring that the workforce is effectively managed and optimized for better patient care and operational efficiency. 48
Hospital Human Resource Forecasting
Expanding Demand and Complexity in Human Resources
As societal demand for medical services surges, particularly within public hospitals, the scale of these institutions continues to grow. 49 The dynamics of personnel management become increasingly complex due to the significant number and mobility of staff across various domains such as medical care, technology, administration, and logistics. 50 Furthermore, the constant influx of personnel for further education and internships adds to the complexity, rendering traditional methods inadequate for long-term human resource management.
Leveraging BI Tools with DL
BI tools, augmented by DL-based DSSs, offer a suite of data mining analysis methods, including clustering analysis, predictive analysis, regression analysis, and correlation analysis. 51 These tools empower users to select appropriate models based on data types, thereby enhancing predictive outcomes. 52 In the realm of human resource data mining, our study has made preliminary strides in forecasting the number of health care personnel required, with a particular focus on nurse staff.
Influencing Factors on Human Resource Demand
Human resource demand is shaped by both internal and external organizational factors. Internal factors encompass technology and equipment, hospital size, and operational direction. 53 External factors include economic conditions, the political environment, technological advancements, and competitive pressures.
Predictive Modeling for Future Planning
For instance, Table 2 employs a time series model to analyze historical changes in the number of hospital health personnel from 2005 to 2023, assuming constant influencing factors. This model forecasts the potential range of changes in various health personnel categories, including nurse staff, over the next five years, providing valuable insights for organizational units to plan their future personnel needs. 54
Analysis of time series interval forecast of health personnel from 2005 to 2023
The integration of DL and BI tools into hospital human resource management offers a sophisticated approach to forecasting, benchmarking, and reporting. 55 This not only addresses the complexities of modern hospital environments but also equips decision-makers with actionable insights for strategic planning and improved operational efficiency, 56 with a particular emphasis on the management of nurse staff. 57
As new algorithms become integrated into patient care processes, it is crucial for nurses to develop proficiency in interpreting diverse data results and incorporating novel information into their practice.
58
Drawing from their experience with the Rothman Index implementation,
59
the YNHH team has provided several best practices for integrating new data into patient care:
Cultivate a Growth Mindset: Fostering an organizational culture that embraces learning and innovation is vital. Teams should be prepared to adopt new methods for collecting and utilizing patient data and information. Localize Tool Experience: The effectiveness of new tools is contingent on their integration into existing practices, informed by frontline provider experiences. The dissemination of tool utility through narratives and word-of-mouth complements formal education and is crucial for widespread adoption. Ensure Ease of Use and Intuitive Interpretation: Tools must be user-friendly, and their output should be easy to interpret, allowing health care professionals to quickly, and effectively utilize the data. Enhance Patient Care: The ultimate goal of any new tool should be to improve patient care. Ideally, these tools should enable nurses to spend more time at the bedside and gain a deeper understanding of the patient’s condition and needs.
60
Discussion
Transformative impact of human resource information management in hospitals
The recent wave of medical reform emphasizes the necessity for efficient hospital management and electronic medical records, 61 thereby driving forward hospital information infrastructure and imposing greater demands on human resource management. 62 Effective human resource information management leverages modern information technology’s networked, intelligent, and digitized capabilities to fully exploit available data resources. 3 By scientifically analyzing material flow, capital flow, talent flow, and information flow, hospitals can significantly enhance their human resource management, expanding its scope and impact across various domains. 63 The integration of DL-based DSSs marks a departure from traditional management limitations, allowing for deep analysis of extensive data accrued from various business systems, ultimately yielding valuable insights for strategic decision-making, particularly in optimizing nurse staff deployment. 64
Addressing data utilization challenges
Presently, the application of HISs is hampered by issues such as fragmented data sources, lack of standardization, and inefficient data utilization. Despite the vast amounts of data generated by hospital business systems, integration remains suboptimal, and data utilization is inefficient. 65 Many institutions still rely on a combination of manual and automated systems for data management. 66 This includes statistical personnel manually compiling data from various departments or business systems, and the subsequent manual analysis required before presenting insights to management. This prolonged decision-support cycle often results in outdated information, underscoring the need for more intelligent, 67 modern tools, such as DL-based DSSs, 68 to effectively manage large data sets and enhance HIS applications. 69 These tools are especially beneficial in optimizing the scheduling and allocation of nurse staff, ensuring better patient care. 70
Enhancing hospital human resource management through advanced analytics
OLAP technology, which revolves around the concept of “dimensions,” encompasses a suite of sophisticated analytical techniques designed for DSSs. 71 By facilitating data aggregation and multidimensional organization, OLAP aids in the precise management of hospital human resources. For instance, the monthly headcount of hospital staff can be aggregated into quarterly or yearly figures. Dimensions such as age, gender, education level, and professional title can be cross-referenced to analyze the quantity and structure of personnel, 72 such as the educational background of health care staff across departments or the composition of medical and nursing personnel in various sections. 73 The integration of DL-based DSSs further enhances these capabilities by providing predictive analytics and insights, particularly useful for nurse staff management. 74 These versatile data exploration methods empower managers to break free from rigid query modes, enabling them to analyze issues from multiple perspectives and objectives, and derive results in varied formats. This analytical capability forms the basis for optimizing organizational structures, effectively arranging labor combinations, ensuring efficient human resource allocation, and enhancing labor productivity to better support frontline clinical services. 75
Driving the evolution of human resource management models
The synergy between information technology and management system reform is pivotal in transforming traditional hospital management models. As hospitals transition from manual and semimanual information collection to fully digital management processes, there is a shift from basic personnel management to comprehensive human resource management. This evolution sees the role of personnel departments expand from routine functions to sophisticated information processing units. 76 The integration of DL-based DSSs into these processes provides real-time analytics and decision-making support, particularly in managing nurse staff schedules and assignments. Standardization and modernization of daily management processes, coupled with improved timeliness and efficiency of decision-support services, will continually drive the reform of human resource management models. This, in turn, maximizes the efficacy of human resource management departments and fosters the deeper and broader enhancement of human resource management practices.
Conclusion
In the dynamic landscape of health care, technological advancements continuously revolutionize patient care approaches. One of the most transformative innovations is DL, 77 a specialized subset of AI that has garnered substantial attention. While already prevalent in radiology, pathology, and other medical fields, the integration of DL into nursing care represents an exciting new frontier. 78
In this discourse, we will delve into the evolving role of DL in nursing practice, 79 exploring its challenges and the myriad opportunities it presents. DL, a sophisticated form of ML, utilizes neural networks with multiple layers to learn from vast datasets. 80 This enables the identification of complex patterns and features, facilitating sophisticated decision-making processes. In health care, DL algorithms have demonstrated remarkable capabilities in image analysis, natural language processing, and predictive modeling. 81
Efforts to standardize data collection and enhance interoperability are critical to fully harness the potential of DL models, as nursing data often presents as heterogeneous, fragmented, and occasionally incomplete. Incorporating DL can significantly enhance clinical decision-making by providing real-time insights. 82 AI-driven tools can assist nurses in patient assessments, risk predictions, and personalized care planning. Continuous monitoring of vital signs, patient movements, and behaviors can preempt adverse events, with DL algorithms analyzing this data to detect changes and promptly alerting nurses 83
For instance, a study by Tunca et al. demonstrated that DL models could analyze gait patterns, sensor data, and patient movements to predict fall risks, enabling nurses to receive alerts and tailor interventions accordingly. Similarly, research by Cicceri et al. showed that by analyzing skin images and patient positioning, DL algorithms could identify early signs of pressure ulcers, allowing nurses to implement preventive measures.
Additionally, DL can aid in medication reconciliation, dosage calculations, and adverse event predictions, thus enabling nurses to focus on patient education and adherence. Despite its potential benefits, DL in nursing also raises several ethical issues that must be addressed. 84 It is crucial for nurses to understand how DL algorithms reach decisions to build trust and foster collaboration between nurses and these algorithms. 85
Moreover, it is essential to ensure that DL models do not perpetuate biases based on race, gender, or socioeconomic status. AI should be viewed as a tool that enhances the expertise of nurses rather than replacing it. 86 To achieve optimal outcomes, effective collaboration between humans and algorithms is paramount.
In summary, as DL technology continues to evolve, nurses can harness its potential benefits to improve patient care, boost operational efficiency, and contribute to a more data-driven health care system. 81 Achieving these goals, however, requires interdisciplinary collaboration, consistent education, and a steadfast commitment to ethical AI practices.
Implementing new workflows is always challenging, and the deployment of AI technologies is no exception. McCarthy suggests the following strategies for successful AI implementation:
Identify a Proof of Concept: Engage frontline users (physicians, nurses, and interprofessional team members) who have a significant pain point to resolve. The issue must be important enough to warrant their time and effort. Cultivate a Growth Mindset: Embrace new practices and accept failures as part of the process. Success relies on the right culture and leadership. Respect Clinicians’ Time: Acknowledge that clinicians have limited availability. Be prepared with essential information, answers to common questions, and feedback mechanisms. Identify Measurable Outcomes: Ensure the outcomes are meaningful and align with organizational goals. Learn from Other Industries: Look beyond health care to see how AI has advanced other sectors and apply those lessons.
By following these steps, AI teams can effectively integrate new technologies, enhancing the efficiency and effectiveness of health care delivery.
Molly McCarthy, Microsoft’s CNO and National Director of the US Provider Industry, envisions AI as a powerful ally for nurses, enabling them to operate at the pinnacle of their professional capabilities. McCarthy has observed that many tasks performed by nurses today could be more efficiently handled by other professionals, allowing nurses to focus on their specialized skills. AI tools promise to relieve nurses of these ancillary duties, redirecting their efforts toward activities that leverage their full education, training, and experience. 87
Microsoft is pioneering the application of AI technologies in three critical areas of health care: clinical, financial, and operational. They work closely with nursing teams to identify how AI can add value to health care delivery. A spokesperson from Microsoft noted, “Nurses are integral to the design, development, and deployment of health information technology. Their expertise is crucial for empowering nurses throughout the health care industry’s digital transformation.”
A recent study on DL-based DSSs for nurse staff in hospitals expands our understanding of DL’s application in nursing care, highlighting its transformative potential. 88 Future research should explore the impact of DL on health care operations management through both quantitative and qualitative lenses. By investigating how DL can optimize health care delivery aspects like resource allocation and patient monitoring, researchers can offer valuable insights (Fig. 5).

DL-based DSS for nurses. This figure illustrates a DL-based DSS specifically designed for nurses, detailing how the system assists in clinical decision-making by analyzing patient data and providing recommendations. DL, Deep Learning.
To integrate DL effectively into nursing practice, a comprehensive framework is essential. This framework should address technical considerations and encompass ethical, legal, and regulatory aspects to ensure AI’s responsible and ethical use in health care settings. 89 Future research should also recognize and mitigate the limitations of current studies, such as potential biases in article selection or analysis methodologies, fostering a more robust understanding of DL in nursing care.
Nurses can enhance their decision-making capabilities by embracing DL technologies, improving patient care outcomes, and streamlining clinical workflows. Continued exploration and utilization of AI in health care necessitate collaboration among researchers, clinicians, policymakers, and industry stakeholders. 90 This collaboration is vital for driving innovation and facilitating the widespread adoption of DL in nursing practice.
As AI and DL continue to evolve, their integration into nursing practice holds immense potential for transforming health care delivery. By addressing the technical, ethical, and regulatory challenges, and fostering interdisciplinary collaboration, we can unlock new levels of efficiency and effectiveness in patient care, ultimately leading to better health outcomes and a more sustainable health care system.
Footnotes
Authors’ Contributions
All authors contributed equally to this manuscript.
Author Disclosure Statement
The authors declare that they have no financial or personal relationships that could inappropriately influence or bias the content of this research. No interests to disclose.
Funding Information
No funding was received for this article.