
Abstract

Several studies since the early 2010s have demonstrated that there can be an inverse relationship between the occurrence of dementia and cancer incidence and that this is two-way. This has been highlighted again in a recent publication. 1
In an early study, Driver et al. showed that there is a negative association between the development of cancers and Alzheimer’s disease (AD) in USA. 2 Over a mean follow-up period of 10 years, compared with control healthy participants, 221 cases of probable AD had a significantly lower risk of subsequently developing cancer (hazard ratio [HR] = 0.39). The same was true for participants with any dementia (HR = 0.44). The cancers involved several types of carcinomas (oesophagus/stomach, colon/rectum, pancreas, lung, melanoma, breast, uterus/endometrium, cervix, ovary, prostate, bladder, and kidney). An independent study by Musicco et al. also found an inverse relationship between cancer incidence and cases of AD in Italy during 2004–2009. Thus, analyses of over 1 million patients revealed that Alzheimer’s patients had a 50% lower risk of developing cancer, including numerous carcinomas. 3 In 161 cases, cancer and AD dementia were diagnosed in the same individuals; in 68 (42%) of these, AD dementia preceded the diagnosis of cancer. Finally, using data collected over 2002–2019, a study on a cohort of 24,664 Korean patients and 98,656 control cases also found that patients with AD had a significantly lower risk of developing various cancers, compared with those without AD (HR = 0.63). The cancers included pancreatic, hepatic, and gastric cancers. This inverse relationship persisted over a follow-up period of 16 years. 4
As regards the underlying mechanism(s), the authors generally considered various common genetic factors and biochemical pathways. 5 The latter could involve risk factors such as inflammation, oxidative stress, and changes in the immune system. On the contrary, independent studies have shown increasingly (i) that tumors are innervated (Fig. 1) and (ii) that the nerve input contributes directly to the cancer process.6–8 Both peripheral and central nervous systems may be involved. Overall, the nerve input accelerates cancer progression both directly and via immune evasion within the tumor microenvironment. 9 The neural input itself can be physical or mediated by chemical messengers released into circulation. In the case of prostate cancer, for example, the sympathetic nervous system (noradrenaline) was shown to promote the early (proliferative) stages of the cancer, while the parasympathetic (cholinergic) input promoted later stages of invasiveness and metastasis. 10 Interestingly, pancreatic cancer, which appeared in all three studies cited above,2–4 is well known to be particularly aggressive and to have one of the strongest nerve inputs. 11
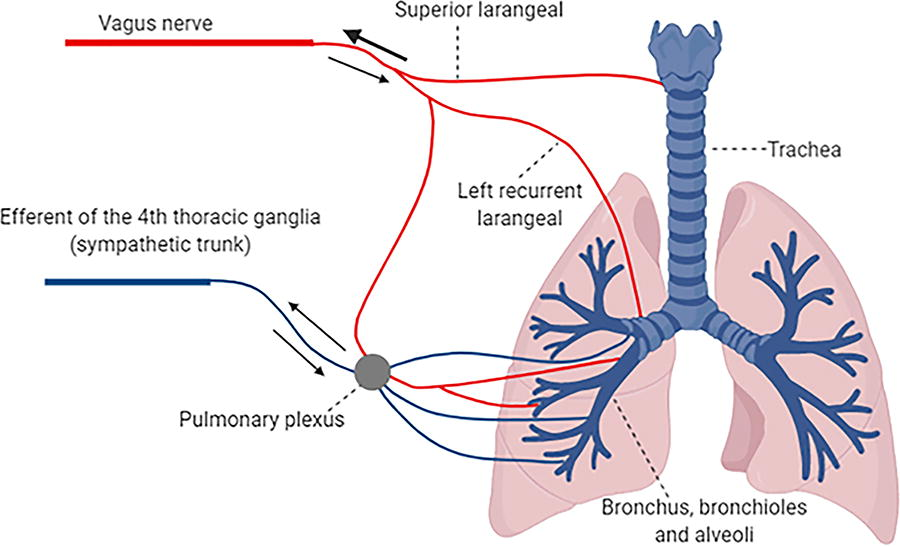
Schematic representation of autonomic nerve inputs to lungs as an example of the substrate for nerve-tumor connectivity. Lung cancer is one of the disease states affected in Alzheimer’s disease. 2 The arrangement also emphasizes the reciprocity of the association. The efferent of the 4th thoracic ganglia of the sympathetic trunk provides “sympathetic” input (blue) via the pulmonary plexus. “Parasympathetic” input (red) is via efferents of the vagus nerve. Arrows indicate the presence of both afferent and efferent fibers, where thickness represents sensory versus motor balance. Reproduced from Hutchings et al. with permission. 6
One can imagine, therefore, that dysfunction of the nervous system in a degenerative state could well lead to a tendency for cancer suppression as a result of impairment in the positive regulatory impact. Indeed, in a particularly radical example, men with spinal cord injuries resulting in functional denervation of the prostate were found to have a significantly lower incidence of prostate cancer (HR = 0.73). 12 The vagus nerve also can affect/promote the cancer process. 13
Interestingly, the cancer-dementia association is reciprocal. Thus, a recent study analyzed data from 3,021,508 individuals aged 60 and over in the UK Clinical Practice Research Datalink over a period up to 30 years (1988–2018). 1 The results showed that survivors of common cancers had a 25% lower risk of developing dementia (HR = 0.75, after adjustment for potential confounders). These authors did identify a common profile (vertical pleiotropy) between genetically predicted cancer and reduced risk of AD. Nevertheless, an additional underlying mechanism could, again, be neuronal and bioelectric since the tumor-neuron association is (also) reciprocal and both nerves and cancer cells are capable of generating electrical signals, including classical Hodgkin-Huxley-type action potentials. 14
This pattern of the apparent inverse relationship between AD and cancer may extend to some other neurogenerative states. Huntington’s disease (HD), a condition in which neuronal death occurs in parts of the brain, has been linked to a significantly (ca. 40%) reduced risk of cancer in several studies, beginning with the original report of Sørensen et al. based on 694 HD patients in Denmark. 15 Evidence for a link between Parkinson’s disease and cancer is somewhat mixed, but a negative association has been reported for most cancers.16,17 Finally, evidence for multiple sclerosis, where nerve conduction is compromised, is also mixed with factors such as immune modulation and disease-modifying medication likely to complicate the picture. 18 Nevertheless, future analyses promise to clarify the situation. 19
In conclusion, first, there is substantial evidence for a parallel between the occurrence of degenerative brain diseases (especially AD and HD) and the development of cancer, and, overall, this association is negative. Second, the neuronal connection, hitherto not considered in ongoing publications, could have a significant involvement in this process. If so, this would indeed be another facet of the burgeoning field of cancer neuroscience, with bioelectricity/ionic activity likely to be a major signaling bridge between the two fields. 20 Much worthwhile work remains to be done to elucidate the underlying mechanism(s) of the dementia–cancer association. This may differ qualitatively and quantitatively amongst individuals, and the balance of the direct/neurogenic versus indirect effects may also vary, so the application of principles of precision medicine will be necessary.
Footnotes
Acknowledgment
The author thanks Julia Ridgway for facilitating this commentary.