
Abstract
Introduction:
Over the last few years, a growth in research and interest in medical cannabis (most often referred to as medical marijuana) use have occurred nationally. Medical cannabis has become a treatment option for disease conditions, such as epilepsy, wasting syndrome associated with AIDs, and post-traumatic stress disorder, when traditional medication is ineffective.
Objectives:
The objectives were to identify knowledge deficits of the medical cannabis program (MCP) in Connecticut among Connecticut pharmacists and the impact of MCP on Connecticut pharmacy practice and concerns Connecticut pharmacists have regarding medical cannabis use.
Methods:
A cross-sectional survey through an online platform, Google forms, was administered for 2 months (October 15, 2017–December 15, 2017). An e-mail containing the link to the survey was e-mailed to all pharmacists whose e-mail addresses were available from the State of Connecticut's Commission of Pharmacy database (n = 6182). Of those with available e-mail addresses, only 5653 pharmacists received the e-mail; the others were rejected upon receipt of our e-mail. Our survey consists of 16 items related to pharmacist demo- graphic information, knowledge assessment, impact on pharmacists' practice, and concerns stemming from medical cannabis.
Results:
Only 51 (15.2%) respondents believed that Connecticut MCP would impact their practice. Only 39 (11.6%) respondents selected the two correct requirements for patient registration and correctly identified the wrong choices. Only 81 (24.2%) respondents identified the correct approved dose (maximum allowable monthly amount of 2.5 ounces) of medical cannabis. Sixty-eight (20.2%) respondents correctly identified all three approved conditions and all other incorrect conditions. Sixty-five (19.40%) respondents correctly identified all roles of dispensary pharmacists. Majority of respondents, 243 (72.5%), expressed their concern about federal laws regarding cannabis. A total of 98 (29.3%) respondents thought that they were knowledgeable enough about the side effects of medical cannabis to provide appropriate counseling to patients.
Conclusion:
Overall, the results of our survey found that Connecticut licensed pharmacists had lack of complete and accurate knowledge regarding the state's MCP. As more states legalize medical cannabis, it will be imperative that education of pharmacists and other health care professionals about the MCP and the clinical use of cannabis occur.
Introduction
Over the last few years, a growth in research and interest in medical cannabis (most often referred to as medical marijuana) use have occurred nationally. Medical cannabis has become a treatment option for disease conditions, such as epilepsy, wasting syndrome associated with AIDs, and post-traumatic stress disorder, when traditional medication is ineffective. Thirty-three states, the District of Columbia, Guam, and Puerto Rico have laws decriminalizing medical cannabis, which range from broad decriminalization to strict/limited medical use, while 10 states have decriminalized recreational cannabis use in adults.1,2 Five states, Arkansas, Minnesota, New York, Oklahoma, and Pennsylvania, in addition to Connecticut mandate role of the pharmacist in provision of medical cannabis.1,2
In June 2012, Connecticut Governor Malloy signed into law a state medical cannabis program (MCP). 3 Several amendments to the regulations have occurred that have expanded the program (call-out box). 3 Despite these state laws, cannabis remains a Schedule I controlled substance federally under the Controlled Substances Act (21 U.S.C. § 811). 4 Therefore, health care professionals working within the medical cannabis arena are not protected against federal prosecution even in states with laws decriminalizing medical cannabis.
Limited research within the last 5 years in states with medical cannabis has evaluated the knowledge and attitudes of physicians and pharmacists regarding state MCPs. In a survey of New York physicians' perspective and knowledge of the state MCP, a total of 167 respondents participated in the survey with the majority (87%) of physicians responding to the survey as not registered providers with the New York's MCP. 5 Sixty percent of respondents were somewhat or not well informed about the endocannabinoid system. In terms of knowledge of the state MCP, 45% of respondents had no familiarity of patient requirements for the state MCP, while 47% had no familiarity of physicians' requirements to participate.
In Minnesota, a similar survey was administered to pharmacists before the launch of the state MCP. The survey assessed pharmacists' preparedness for the state program in terms of competency in program policies and procedures, as well as the pharmacotherapy. 6 In addition, the survey assessed pharmacists' comfort with patient counseling on medical cannabis products. In this study, 738 responses were collected. Seventy-five percent of respondents had little to no self-perceived knowledge of cannabis pharmacology. With regards to the state program, respondents had mixed results in knowledge of dosage forms eligible for distribution (87% identified oral pill as eligible, and 46% identified inhaled cannabis from cannabis extract as eligible) and qualifying medical conditions (90% for cancer related pain and 24% for Crohn's disease).
Pharmacists are positioned perfectly to play a vital role in selection, education, and delivery of medical cannabis. In Arkansas, Connecticut, Minnesota, New York, Oklahoma, and Pennsylvania, a pharmacist is mandated to be involved in their state specific MCP. 1 Pharmacists in these six states provide consultations at state-approved cannabis dispensaries. 1 In Connecticut, each dispensary must have a pharmacist on site during business hours. Once the patient is certified by a physician or nurse practitioner and having a qualifying condition, the patient can apply to receive a medical cannabis card. The patient then goes to a state-approved dispensary for a consultation with a pharmacist to obtain medical cannabis. To date, no published research has assessed pharmacists' knowledge of Connecticut MCP, its impact on the practice of pharmacy, and concerns following implementation of the state's MCP. This study provides insight into self-identified areas of knowledge deficits by Connecticut pharmacists that allow targeted development of future professional development activities related to medical cannabis use and regulations in the state of Connecticut and within other states implementing medical cannabis laws.
The objectives of this study are to identify: (1) knowledge deficits of the MCP in Connecticut among Connecticut pharmacists; (2) the impact of MCP on Connecticut pharmacy practice; and (3) concerns of Connecticut pharmacists regarding medical cannabis use.
Materials and Methods
The Institutional Review Board of the Philadelphia College of Osteopathic Medicine approved this study. A cross-sectional survey through an online platform, Google forms, was administered for 2 months (October 15, 2017–December 15, 2017). An e-mail containing the link to the survey was e-mailed to all pharmacists whose e-mail addresses were available from the State of Connecticut's Commission of Pharmacy database (n=6182). Of those with available e-mail addresses, only 5653 pharmacists received the e-mail; the others were rejected upon receipt of e-mail. A follow-up e-mail was sent midway through the survey period reminding those who had not already completed the survey to take the survey.
The survey consists of 16 items related to pharmacist demographic information, knowledge assessment, impact on pharmacists' practice, and concerns stemming from medical cannabis. Three items focused on pharmacist demographic (current practice setting, years in practice, and age of pharmacist). Four items assessed pharmacist knowledge of Connecticut medical cannabis laws, including drug schedule class, patient registration, approved dosage forms, and dosing. With regards to assessing pharmacist's knowledge of the Connecticuts' MCP, four items addressed assessment of approved medical conditions, quality control, role of dispensary pharmacist, and dispensing process. Impact on practice of the pharmacist was assessed by questions about the pharmacists' awareness of patients in their pharmacy enrolled in MCP and percentage of patients enrolled in MCP. One item addressed specifically what concerns pharmacists had about medical cannabis. Finally, pharmacists rated their knowledge of medical cannabis side effects, drug–drug interactions, and efficacy using a 5-point Likert scale where 1 represented “strongly disagree” and 5 represented “strongly agree.” Our survey was not pretested for validity or reliability. Descriptive statistics was used to report frequency for each item. Chi-square test was used to measure any association between categorical variables. All analyses were conducted using SAS version 9.4 (Cary, NC).
Of the 5653 pharmacists who received an e-mail about the survey participation, 335 (5.9%) responded to our survey (Table 1). Most (47.2%) respondents worked in a community setting, and 72 (21.5%) worked in hospital setting. Almost one-third, 111 (33.1%), pharmacists had work experience less than 10 years, and 107 (31.9%) had more than 30 years of work experience (Fig. 1).
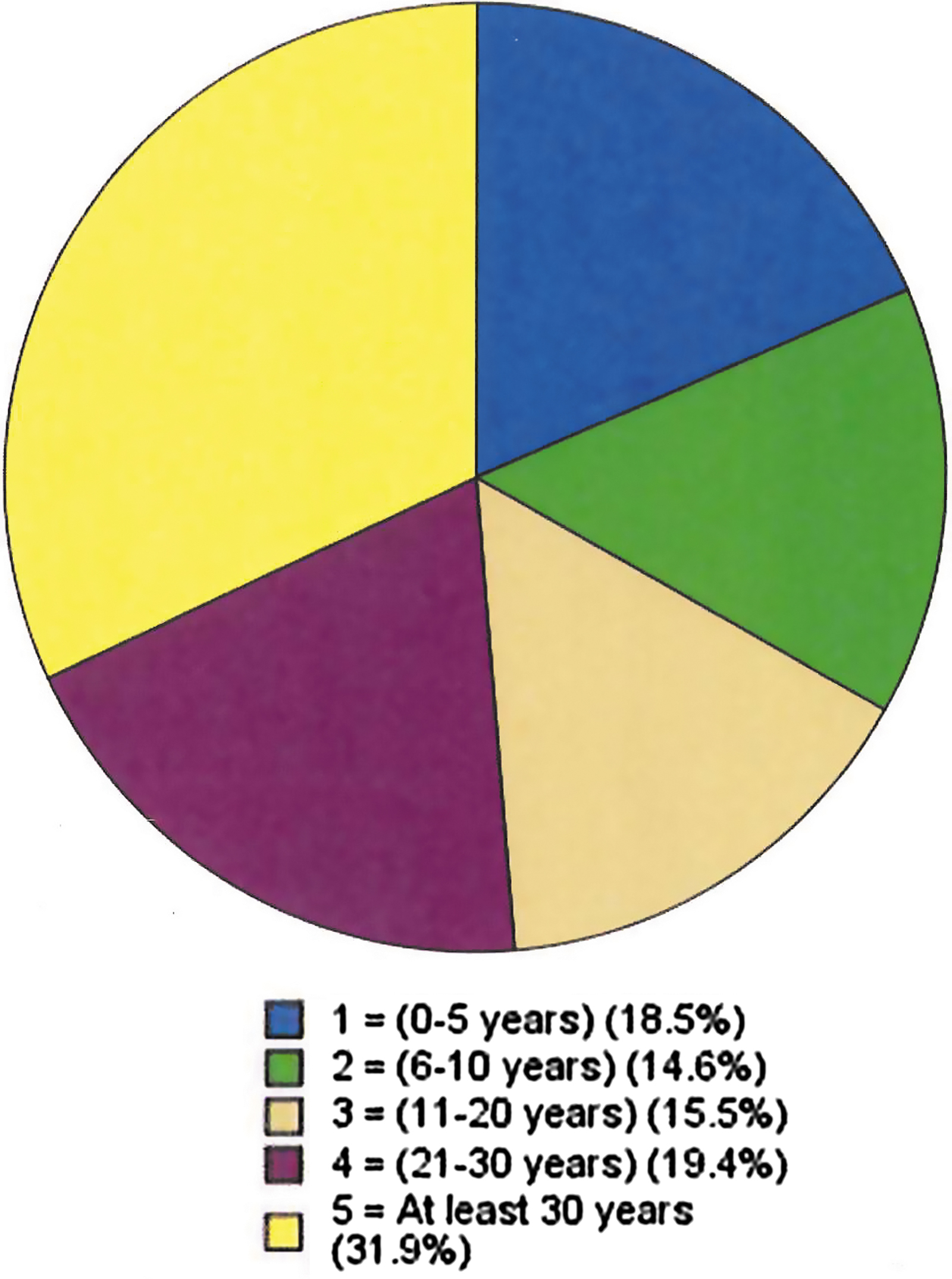
Number of years of practice.
Pharmacists' Knowledge of Connecticut's Medical Cannabis Program
Full knowledge: Survey respondent selected all correct answer choices. Partial knowledge: Survey respondent selected at least one but not all correct answer choices. No knowledge: Survey respondent did not select any correct answer choices.
Pharmacists' knowledge of the Connecticut MCP is detailed in Table 1 and Figure 2. Pharmacists' concerns regarding MCP are highlighted in Figure 3. Table 2 details pharmacist self-assessment of medical cannabis.
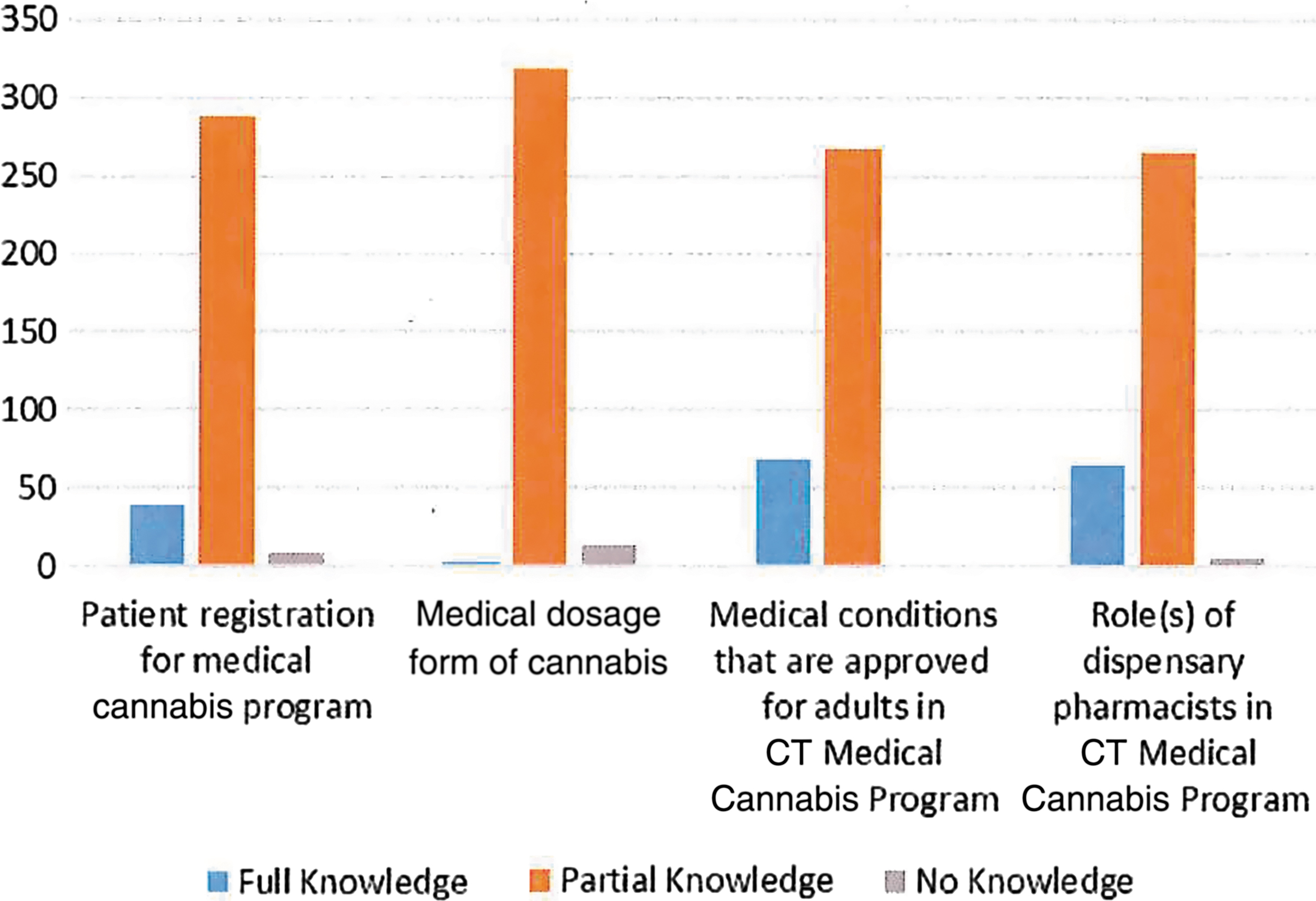
Pharmacist knowledge of Connecticut (CT) Medical Cannabis Program.

Pharmacist concerns regarding medical cannabis.
Pharmacist Self-Assessment of Medical Cannabis
Identification of the correct Drug Enforcement Administration Scheduling of cannabis was significantly (p=0.01) associated with number of years in practice, but not with the practice setting (p=0.22). The number of years of practice was also significantly (p=0.01) associated with correct identification of the role of dispensing pharmacists in the Connecticut MCP. A significant association (p=0.0335) existed between practice setting of the respondents and correct identification of dispensing rule in the state of Connecticut. Neither practice setting nor number of years of practice had any significant association with the respondents' thought about the impact of Connecticut MCP on their practice or different types of concerns regarding use of medical cannabis. Respondents' perception about their knowledge level to counsel patients related to side effects, drug–drug interactions, and efficacy of medical cannabis had no significant association with practice setting or the number of years in practice.
Discussion
Despite Connecticut having a MCP since 2012, this is the first study to identify whether MCP knowledge deficits by licensed pharmacists in the state of Connecticut exist. Overall, the results of the survey found that Connecticut licensed pharmacists lack complete and accurate knowledge regarding the state's MCP, including medical dosage form of cannabis, correct and approved dosage, approved medical conditions among adults, possible roles of dispensary pharmacists, and patient registration requirements. Furthermore, the study identified the concerns of Connecticut pharmacists regarding medical cannabis use and the impact of MCP on Connecticut pharmacy practice. Similar findings were also observed in a survey of pharmacists in the state of Minnesota, where pharmacists demonstrated a partial understanding of the patient registry program and had a lack of knowledge about their role in MCP. 6 It is important to mention that although most of the pharmacists identified some of the correct dosage forms of medical cannabis, only three of them could accurately identify all of the correct dosage forms. 6 More than three-fourth of the respondents could not correctly identify the dose of medical cannabis as approved in the state of Connecticut. Deficits of accurate knowledge of approved medical conditions for medical cannabis and the role of dispensing pharmacists are potential deterrents to providing adequate and appropriate patient counseling. In the California Pharmacy Student Leadership (CAPSLEAD) program, a survey of medical cannabis users measured user interest of having a pharmacist or health care professional counsel them on proper usage of the medical cannabis. 7 Findings revealed that 36% (n=28) strongly agreed that they would like contact with a health care professional, 29% (n=22) slightly agreed, 19% (n=15) were neutral, 4% (n=3) slightly disagreed, and 12% (n=9) strongly disagreed that they would like contact with a health care professional. 7 No correlation was found between an increased interest in engagement with pharmacist or health care professional and users with side effect experiences, complex drug regimens, or recently started using medical cannabis. 7 Rather, the majority of patients expressed an interest in pharmacist engagement, revealing a need for pharmacists to have competency in counseling on medical cannabis in a diversity of patients. 7
The present study found that number of years in practice had a significant association with identification of the right schedule of cannabis in Connecticut and the role of dispensing pharmacists. Those with less than 10 years of practice experience performed significantly better in identifying the correct schedule and the accurate role of dispensing pharmacists. However, this is not surprising given that medical cannabis was legalized in the state of Connecticut in mid 2012. One of the possible reasons may be that pharmacists who were licensed in recent years received more training on medical cannabis compared to those who have been in practice for a long time. These results call for more education and training on medical cannabis among pharmacists with particular focus on those who have been in practice longer than 10 years. Training would enable practicing pharmacists to become more knowledgeable and competent in providing patient counseling on the use of medical cannabis. Almost three-fourth of the respondents expressed significant concern about federal laws related to cannabis. Because cannabis is a schedule I drug according to federal law, more guidance and training on handling medical cannabis would be helpful for pharmacists. Continuing education is a vital resource for training of pharmacists on medical cannabis. In a survey of Minnesota pharmacists, an overwhelming majority felt incompetent regarding clinical knowledge of medical cannabis. 7 In the CAPSLEAD study, 57% of pharmacists who received medical cannabis continuing education stated that the general knowledge directly impacted their comfort level compared to 94% of pharmacists who did not receive the continuing education. 7 In the current Connecticut study, a majority of pharmacists also expressed concerns about the interaction between medical cannabis and other medications and potential adverse effects. The survey also identified that the pharmacists were concerned about the quantity and quality of current scientific evidence of medical cannabis and Connecticut state regulations. Interestingly in the CAPSLEAD study, the primary reason for discomfort in pharmacist counseling on medical cannabis was a general lack of knowledge about medical cannabis. This again suggests education as the largest barrier to counseling. 7
The present study also found that many pharmacists had very low self-rated knowledge level about side effects, drug–drug interaction, and efficacy of medical cannabis. Similar findings were found by Hwang et al. who evaluated Minnesota pharmacists before the initiation of Minnesota's MCP. 6 A survey of medical schools revealed that 75% of respondents felt graduates were not prepared or only slightly prepared to discuss medical cannabis with patients. 8 Similarly, in a recent national survey of 400 oncologists regarding their attitude and knowledge of medicinal cannabis, most oncologists reported having discussed cannabis use with patients or their families, yet only 30% of oncologists reported feeling adequately knowledgeable to do so. 9 These studies demonstrated that health care professionals tend to feel inadequate in their knowledge about medical cannabis despite often having to make clinical recommendations.
In a survey of Minnesota pharmacists, an interest in further education regarding medical cannabis and state regulations was expressed by pharmacists. 8 The majority of pharmacists felt incompetent in clinical knowledge of medical cannabis, which suggested that they were not sufficiently prepared to work with patients enrolled in the state's MCP. In addition, these pharmacists lacked understanding of the patient certification requirements and process for the state program. 8 In another study, the lack of general knowledge and education on medical cannabis created the greatest barrier to counseling by the pharmacist. 7 A positive association was found between pharmacist's education on medical cannabis and comfort level in counseling on this medication. Clearly, there is a demand for additional continuing education on medical cannabis in order for pharmacists to feel comfortable and be proficient in counseling on medical cannabis. Great opportunity exists within the curriculum of schools of pharmacy to integrate more didactic material on medical cannabis. 7 Clearly, both development of continuing education courses and curriculum within schools of pharmacy are ideal for equipping pharmacists to become competent in counseling patients on medical cannabis.
In another study, a lack of medical or clinical training on cannabis health information was clearly pointing to the need for medical training programs to incorporate cannabis health and risk information. 10 In a survey of curriculum deans representing 82 allopathic and 19 osteopathic medical schools from 37 states, 24% rated their graduates as moderately, very, or extremely prepared to answer questions about medical cannabis. Almost half (48.4%) of curriculum deans agreed or strongly agreed that medical school education should incorporate medical cannabis education. 11 According to Association of American Medical Colleges Curriculum Inventory, only less than 10% of medical schools teach medical cannabis in their curriculum. 11 In Kondrad and Reid study, 80% of respondents agreed that medical cannabis training should be incorporated into the medical school curriculum, and 92% agreed that medical cannabis continuing medical education should be available to primary care providers. 12 Overall respondents showed a strong desire for medical cannabis educational opportunities at all levels of medical education. 12 Pharmacists are similar to physicians in expressing interest in educational training on medical cannabis. In Isaac et al. study, majority of respondents demonstrated a need for development of training courses to ensure greater understanding of effects of medical cannabis. 13 Most importantly, majority of patients expressed interest in pharmacist involvement, which demonstrated the need for pharmacist to have competence in counseling patients on medical cannabis. 7
In addition, in our study, most pharmacist respondents indicated that they had patients enrolled in the MCP, but less than one-fourth of respondents were unaware if they had patients enrolled in the MCP. Lack of awareness about enrollment of individual patients could pose a significant challenge to pharmacists in providing appropriate counseling to patients. Pharmacists should be aware of patients who are enrolled in MCP, so that careful monitoring can be done to reduce chance of any misuse and adverse effects.
A very small proportion of respondents mentioned that the Connecticut MCP affected their practice. It could be that pharmacists do not participate in education of patients, clinical monitoring, or recommendations for use because they are not working in medical cannabis dispensaries. In addition, it could be that because of the reported inadequate knowledge, pharmacists feel uncomfortable discussing medical cannabis with patients. Increasing pharmacists' knowledge by providing adequate training about MCP in the state of Connecticut could assist pharmacists to take a more active role in managing patients registered with MCP and thus potentially improve patient care. The study population included registered pharmacists within the state of Connecticut at the time in which the MCP had been in place for 5 years. Although information and professional development have been offered throughout the existence of the program, practicing pharmacists are not required to participate. The results indicated a perceived need of pharmacists despite the previous offerings and likely indicate that other health care professionals may have similar needs. Because the study only included pharmacists licensed in Connecticut and had a very low overall response rate, the generalizability of study findings is low. The current study found similar results as a previous study of Minnesota pharmacists. Inherent to a survey of this nature is response bias, and this must be considered when assessing survey findings. Furthermore, self-selected participation by pharmacists possibly influenced the findings of the study. If the majority of pharmacists with adequate knowledge about MCP did not participate in the survey, findings undermine the level of knowledge about MCP among the pharmacist community in the state. Nevertheless, availability of further training would help the whole pharmacist community to be better prepared to serve the patients who were registered with the Connecticut MCP.
Conclusion
The survey found that even 5 years after medical cannabis was approved in the state of Connecticut, a significant portion of practicing pharmacists still require adequate training to actively participate in patient care related to MCP. As more and more states decriminalize medical cannabis, it is imperative that education of pharmacists and other health care professionals about the clinical use of medical cannabis occurs and the program itself occurs before implementation of the MCP. It is also necessary to continue to provide continuing professional development that focuses on new regulations, laws, and emerging evidence about medical cannabis use, benefits, and risks. Health care professional organizations should take the lead in providing this education to pharmacists and other health care professionals, such that they can engage more effectively in patient care and influence the legislative process related to medical cannabis.
Footnotes
Acknowledgment
The authors thank Marghie Giuliano of the Connecticut Pharmacists Association for assisting them during the study design.
Authors' Contributions
Drs. Reece and Mukherjee designed the methodology and developed the survey tool. Drs. Reece, Holle, and Mukerjee wrote the original draft of the article.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.