
Abstract
Introduction:
Osteoarthritis (OA) is disabling and degenerative disease of the joints that is clinically characterized by pain and loss of function. With no disease-modifying treatment available, current therapies aim at pain management but are of limited efficacy. Cannabis products, specifically cannabinoids, are widely used to control pain and inflammation in many diseases with no scientific evidence demonstrating their efficacy in OA.
Objective:
We investigated the effects of non-euphorigenic cannabis extracts, CBD oil and cannabigerol oil (CBG oil), on pain and disease progression in OA mice.
Methods and Results:
Twelve-week-old male C57BL/6J mice received either sham or destabilization of the medial meniscus (DMM) surgery. DMM mice were treated with vehicle, CBD oil, or CBG oil. The gait of DMM mice was impaired as early as 2 weeks following surgery and continued deteriorating until week 8, which was restored by CBD oil and CBG oil treatments throughout the disease course. Mechanical allodynia developed in DMM mice, however, was not ameliorated by any of the treatments. On the other hand, both CBD oil and CBG oil ameliorated cold allodynia. In open field test, both oil treatments normalized changes in the locomotor activity of DMM mice. CBD oil and CBG oil treatments significantly reduced synovitis in DMM mice. Only CBG oil reduced cartilage degeneration, chondrocyte loss, and matrix metalloproteinase 13 expression, with a significant increase in the number of anabolic chondrocytes. Subchondral bone remodeling found in vehicle-treated DMM mice was not ameliorated by either CBD or CBG oil.
Conclusions:
Our results show evidence for the therapeutic efficacy of CBD oil and CBG oil, where both oils ameliorate pain and inflammation, and improve gait and locomotor activity in OA mice, representing clinical pain and function. Importantly, only CBG oil is chondroprotective, which may provide superior efficacy in future studies in OA patients.
Introduction
Osteoarthritis (OA) is one of the most common musculoskeletal disease and affects over 30 million adults in the United States and over 300 million people worldwide.1,2 This condition is clinically characterized by joint pain, tenderness, crepitus, and stiffness with limitation of movement, which affects daily activities, including personal care, ability to work, and maintaining the household. 1 Chronic pain is a major complication of OA that negatively impacts physical function and quality of life for patients.3,4 Additionally, OA places a significant financial strain on the health care system with an estimated 300 billion dollars in medical costs and lost earning annually. 2
There is currently no disease-modifying OA drugs (DMOAD) to prevent cartilage degeneration, 5 and the only end-point treatment option is joint replacement surgery. 6 Thus, existing treatments mainly focus on pain management to reduce disability and improve physical function. 7 Nonsteroidal anti-inflammatory drugs and steroids are the most commonly used medications; however, their effects are inadequate as they wear off over time,7,8 and they may even worsen OA progression 8 as well as cause serious health risks when used long term. 9 Opioids are another line of treatment utilized to control OA pain, but their low efficacy and abuse potential represent serious concerns.8,9 Nearly 60% of OA patients are not satisfied with their current pain management, 10 thus, there is a need to discover nonaddictive therapies that can control OA pain with fewer side effects.
Cannabis use to control pain in OA patients is continuously increasing, with numerous preclinical studies supporting its efficacy.10–12 Cannabinoids exert their effects by targeting the endocannabinoid system (ECS), a homeostatic regulator of neurotransmitter activity that functions in the brain, skin, digestive tract, liver, cardiovascular system, genitourinary function, bone, 13 and most relevantly cartilage.14–16 The ECS consists predominantly of anandamide (AEA) and 2-arachidonoylglycerol (2-AG), which regulate pain through cannabinoid receptors. The ECS is activated in several different diseases where it is involved in inflammation and cell differentiation. It is expressed in all joint compartments where evidence demonstrates its involvement in (1) modulating chronic pain and (2) ameliorating joint inflammation and degeneration in OA.7,10,14,17,18
Anecdotal evidence suggests the efficacy of cannabinoids in regulating chronic pain with the ECS being the key target.10,19 Studies in animal models have identified possible ECS pathways in arthritis, 20 with growing evidence for the analgesic and anti-inflammatory effects of cannabinoids in OA.7,21 This suggests that targeting the ECS with cannabinoids is a promising therapeutic strategy in OA.7,10,17
CBD is the main nonpsychoactive cannabinoid derived from cannabis that has been used in OA.10,22,23 While cannabigerol (CBG) is another recently emerging nonpsychoactive cannabinoid, and is the precursor molecule to both CBD and Δ 9 -THC in the plant,24,25 its effects in OA have not been investigated. 26 CBD specifically has been demonstrated to have analgesic effects, diminishing hyperalgesia and mechanical/thermal allodynia.7,20 Additionally, CBD has potential anti-inflammatory effects in OA, but with insufficient evidence 7 ; while some studies report anti-inflammatory effects of CBD, others have reported opposing results.7,21
Importantly, OA is a disease of the whole joint; it not only affects the joint cartilage, but also the underlying bone, and the synovial membrane encapsulating the joint.17,27 Thus, a pain management strategy that does not compromise joint tissues or, better yet, which simultaneously ameliorates pathological joint remodeling, would be a promising therapeutic intervention. So far, there are no comprehensive studies that investigate the effect of phytocannabinoids on chronic pain as well as OA progression.4,7
We hypothesized that the non-euphorigenic cannabinoids, CBD and CBG, in the cannabis extracts (CBD and CBG oils) can reduce OA chronic pain and possibly disease progression. Thus, we investigated the therapeutic efficacy of CBD oil and CBG oil in a clinically relevant surgical OA model of destabilization of the medial meniscus (DMM), where we focused on determining their effects on pain, gait, locomotor activity, and joint remodeling.
Materials and Methods
Study design
Sample size was determined using the G*Power 3.1 software. Based on our previous experience and studies, the area of uncalcified tibial cartilage and the total number of chondrocytes are the two main parameters affected by DMM. Based on the difference between these two groups we calculated the sample size required for each group to reach 5% significance and 0.80 power. Power analysis showed that at least four mice in each group are required. Thus, we increased the number of mice from seven to nine to account for any unexpected side effects due to surgery or treatments. The end-point of 8 weeks post-DMM was chosen based on our and others experience with the DMM model where mid-stage OA develops.23,28–30 The surgeon and laboratory personnel performing daily drug injections, pain and behavioral assessment were blinded to the animal identity and treatment.
All animals were randomized for treatment. All mice treatments were initiated after DMM and their collected samples were coded and analyzed in a blinded manner until data were obtained and quantification was completed. Data were then decoded and matched to the corresponding groups, results were charted, and statistical analysis was performed. Outlier data determined by Grubb's test were excluded.
Animals
Twelve-week-old male C57BL/6J mice were purchased from The Jackson Laboratories. All mice were housed in groups of three to five mice per microisolator cage in a room with a 12-h light/12-h dark schedule. All animal procedures were performed according to the National Institute of Health (NIH) Guide for the Care and Use of Laboratory Animals and approved by the Animal Care and Use Committee of the Pennsylvania State University.
Drugs
To determine whether cannabis extracts can prevent or decelerate OA progression in the DMM model, we used two commercial cannabis extracts: CBD oil (Nuleaf Naturals, Denver, CO) and CBG oil (Extract Labs, Boulder, CO). CBD oil (50 mg/mL CBD content), is a low THC product (Table 1) derived from Cannabis sativa with growing potential as an alternative method for treating chronic pain. 31 The CBG oil is a cannabis extract that is high in both CBG (25 mg/mL) and CBD (25 mg/mL) (Table 1). CBG is the precursor molecule for the most abundant phytocannabinoids, including CBD and Δ 9 -THC. Although CBG demonstrates activity characteristics similar to those of CBD at some receptors,24,25,32 there is little research regarding the potential of CBG oil in treating OA pain. 32 The cannabinoid (Table 1) and terpene composition (Table 2) of each oil was independently verified (Keystone State Testing Labs, Harrisburg, PA), and dosing levels were based upon these findings. Extracts were diluted in fractionated coconut oil to the concentrations listed above.
Cannabinoid Composition of the Diluted Oils as Used in the Experiments as Measured by Independent Laboratory Analysis (Keystone State Testing Labs, Harrisburg, PA)
CBC, cannabichromene; CBDA, cannabidiolic acid; CBDV, cannabidivarin; CBG, cannabigerol; CBN, cannabinol.
Terpene Composition of the Diluted Oils as Used in the Experiments as Measured by Independent Laboratory Analysis (Keystone State Testing Labs, Harrisburg, PA)
Experimental groups
In 12-week-old male wild-type C57BL/6 mice that received DMM surgeries, vehicle (coconut oil, n=7), CBD oil (20 mg/kg/day CBD, n=7), or CBG oil (10 mg/kg/day CBG, and 10 mg/kg/day CBD, n=7) were administered every other day by subcutaneous injection in the OA knee region. Drug treatment was initiated 3 days following DMM. Sham-operated mice (n=9) with only skin incision performed, to avoid inflammatory reaction in the joint, were used as the non-OA controls. Mice were euthanized 8 weeks following DMM, at 20 weeks of age, to determine the effect of treatments on the development and progression of OA. Blood was collected to quantify blood levels of CBD and CBG. Knees were collected, microcomputed tomography (micro-CT) scanned, formalin fixed, and paraffin embedded for further analyses.
DMM surgery
Twelve-week-old male mice were administered DMM surgery to the right knee and sham surgery to the left knee as described.23,28,30 Mice were sacrificed at the indicated time point by anesthesia, followed by whole animal perfusion using 10% NBF (normal buffered formalin). Knees were harvested and fixed for 7 days in 10% NBF, decalcified for 7 days in 10% w/v EDTA, embedded in paraffin, and 5 μm sections were cut and mounted for Safranin-O/Fast Green or immunofluorescence (IF) staining.
Gait analysis
The gait of mice was analyzed using the paw-print method. 33 The hind legs were stamped on an ink pad and mice were placed at the end of a 3-feet dark tunnel, which was lined with blank paper. The mice walked across to the other side of the tunnel and the ink marked the gait of the mice. The paper was collected, and three different gait parameters (stride, stance, and sway) were recorded and quantified by investigators blind to the treatment. 33
Acetone test
The acetone test was used to measure sensitivity to cold. In this assay, a drop (50 μL) of acetone is gently applied to the plantar surface of the hind paw and the total time spent in acetone-evoked behaviors (paw elevation, flinching, licking, and scratching) over a 1-min observation period is determined.
von Frey test
Mechanical hypersensitivity was assessed using an electronic von Frey apparatus (IITC Life Sciences). Mice were acclimated for 30 min to individual plexiglass chambers located on top of a wire mesh table. The electronic von Frey anesthesiometer equipped with a semi-flex tip was touched onto the plantar surface of the right hind paw. The amount of force (grams) required to evoke a paw withdraw response was measured in triplicate and the highest value was recorded.
Open field test
In a subset of randomly selected mice, locomotor activity was tracked during spontaneous exploratory movement through automated software (Activity Monitor; Med Associates, St. Albans VT) controlling horizontal and vertical infrared light sensors (at 1.5 cm intervals) within the open field arena (30×30×20 cm; Med Associates). Total distance traveled was recorded over the 30-min testing period and locomotor traces were plotted as 1 sec bins. Assessments were performed 2–5 h into the light cycle of a well-lit room and all groups were exposed to the same lighting conditions.
CBD and CBG blood level measurement
The doses of CBD oil and CBG oil in this study were chosen based on reports in the literature, where animal studies used doses ranging between 1 and 50 mg/kg/day. In clinical settings, these oils are used by topical application on the OA joint. To determine the systemic distribution of CBD and CBG following local subcutaneous injections in mice, we measured their plasma levels. Blood was collected from mice that were treated with vehicle, CBD oil, or CBG oil, and plasma was separated and used to measure the blood levels of both phytocannabinoids by high performance liquid chromatography with tandem mass spectrometry (HPLC-MS-MS). Sciex QTRAP 6500+ mass spectrometry coupled with a Sciex EXion HPLC separation system were used with a HPLC column—Acquity UPLC BEH C18 analytical column (2.1×100 mm), 1.7 μm—with a linear detection range of 0.5–1000 ng/mL for CBD and 0.25–1000 ng/mL for CBG.
Histomorphometry: (Safranin-O/Fast Green) coupled with histomorphometry using the Osteomeasure® system
Using Safranin-O/Fast Green-stained sections, the OsteoMetrics system was used to quantify the above parameters on three sections from representative levels (50 mm apart) of the medial compartment of the joint for each sample, as we previously described.23,28 A blinded observer quantified uncalcified articular cartilage area, total chondrocyte number, matrix-producing chondrocyte number, and the synovial membrane thickness using the built-in area calculation algorithms and quantification functions of the OsteoMeasure system.
IF staining
Paraffin sections were deparaffinized, antigen retrieval was performed, followed by permeabilization, as we previously described. 28 Sections were then blocked for 1 h at room temperature in 10% normal goat serum in 1×TBS; then incubated overnight at 4°C with the rabbit anti-mouse primary antibodies specific for matrix metalloproteinase 13 (MMP13; ab39012; Abcam, Waltham, MA) and cannabinoid receptor type 2 (CB2 receptor; ab3561; Abcam). This was followed by washing, incubation with biotinylated goat anti-rabbit secondary antibody (Life Technologies, Waltham, MA), washing again, and incubation with Alexa Fluor 647 Streptavidin. Finally, slides were washed, mounting and nuclear staining was performed using ProLong™ Gold Antifade Reagent with 4′,6-diamidino-2-phenylindole (DAPI; Invitrogen, Waltham, MA).
We have described the detailed protocol elsewhere. 28 After staining, imaging was performed using Zeiss Axio Observer 7 upright wide-field microscope (Carl Zeiss Microscopy GmbH). Image analysis to quantify the percentage of fluorescence area was performed using Zen Blue Advanced Image Analysis Software. The percentage of fluorescence positive cells was measured as the number of positively stained cells (fluorescence higher than the background threshold set by the software) divided by the total number of cells.
Micro-CT assessment
Before histological processing, harvested knee joints were evaluated through micro-CT using a Scanco vivaCT40 scanner with a 55 kVp source as we have previously described. 34 Joints were scanned at a resolution of 10.5 μm. General three-dimensional (3D) images were obtained with simple segmentation at a Scanco threshold of 260, which was determined on inspection of the first specimen. This translates to a linear attenuation coefficient of 2.080 cm−1.
Analysis of the medial subchondral bone was started by locating the inferior end of the medial subchondral bone plate plus 5 slices. From this start and moving inferiorly, the next 15 slices of the medial trabecular bone were analyzed. A threshold of 260 (2.080 cm−1) was used to analyze bone volume (BV) and microarchitecture. Only trabecular bone was included in the analysis. Osteophytes were identified as protrusions and counted using cross-sectional images of the 3D stacks. Subchondral plate thickness was calculated by determining the number of cross-sections forming the subchondral plate and multiplying it by section thickness. 35
Statistical analyses
Two-way analysis of variance (ANOVA) was used to test the significance of treatment and time effects in gait analysis and von Frey test, whereas one-way ANOVA was used to test the significance of treatment effect in the remaining studies. Tukey's post hoc analysis was performed and data were considered statistically significant if (p≤0.05) was achieved. Homogeneity of data was tested by running the Brown–Forsythe test and if standard deviations were different (p≤0.05), Brown–Forsythe ANOVA was performed with Tukey's post hoc analysis. All calculations were performed using the GraphPad Prism 9.0 program.
Results
CBD oil and CBG oil treatments normalize gait changes in OA mice
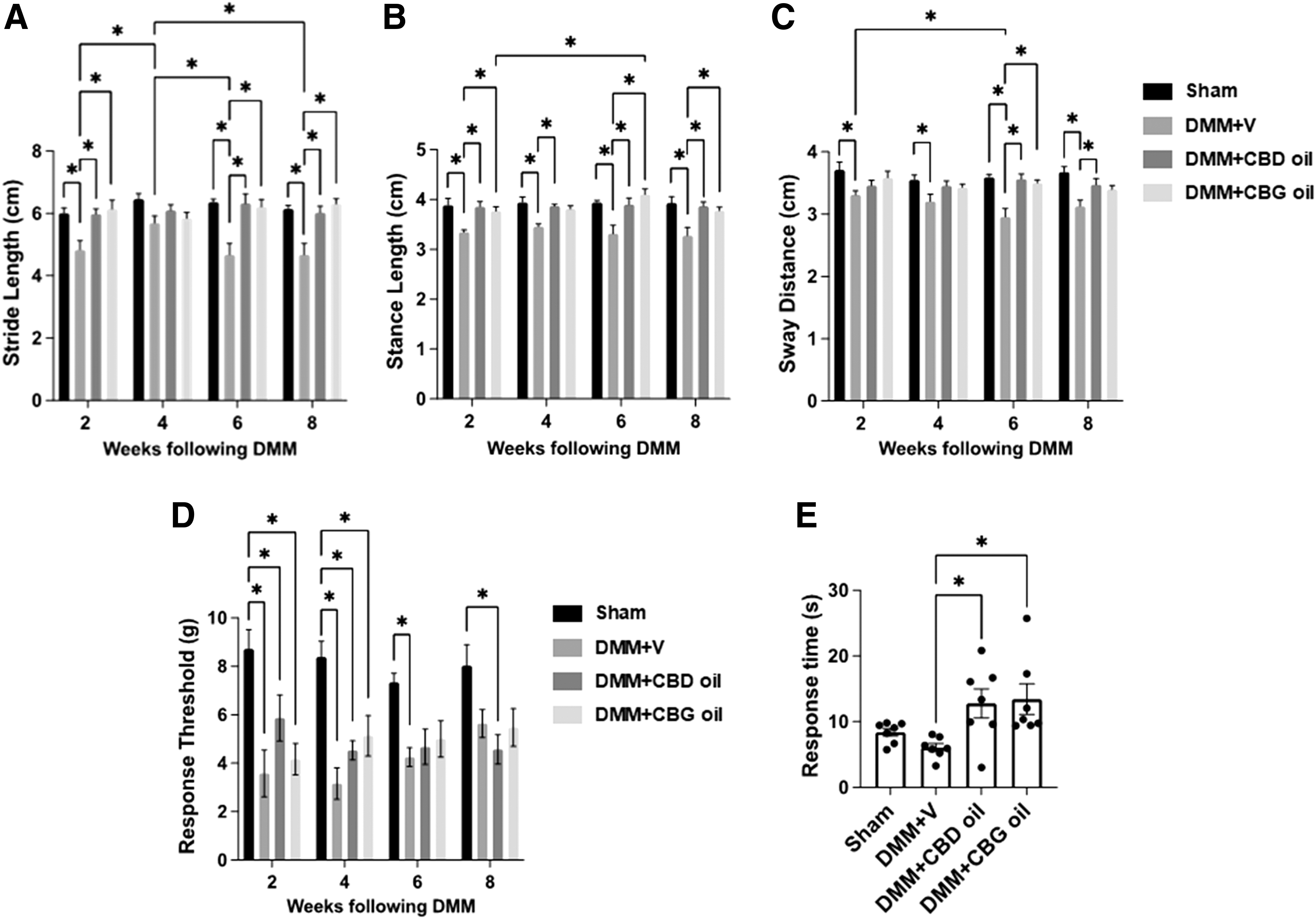
We performed gait analysis in OA mice by evaluating changes in three parameters: stride, sway, and stance, to study limb movement (Fig. 1A–C). Two weeks following injury, vehicle-treated DMM mice showed significantly impaired stride length (4.82±0.304) (Fig. 1A), which was significantly restored by CBD oil (5.98±0.16) or CBG oil (6.14±0.28), administered subcutaneously over the joint (Fig. 1A). This continued through the later phase of OA disease progression at 6 and 8 weeks following DMM (Fig. 1A). Four weeks following DMM, the stride length of vehicle-treated DMM mice was not different from sham mice, but was significantly different from vehicle-treated DMM mice at weeks 2, 6, and 8. CBD oil and CBG oil had no effect on stride length at week 4 post-DMM. Vehicle-treated DMM mice showed significantly impaired stance length (3.34±0.045) 2 weeks following DMM (Fig. 1B), which was significantly restored by CBD oil (3.85±0.10) or CBG oil (3.76±0.08) (Fig. 1B). This continued at 4, 6, and 8 weeks following DMM (Fig. 1B).
CBD oil and CBG oil normalize gait and ameliorate cold allodynia in PTOA mice.
Sway distance was impaired as early as 2 weeks following DMM in the vehicle-treated mice (3.311±0.06537), and continued to worsen as OA progressed, but was restored by CBD and CBG oil treatment at week 6 (3.50±0.046 [V], 3.56±0.08 [CBD], 3.50±0.04 [CBG]) and week 8 (3.12±0.09 [V], 3.47±0.10 [CBD], 3.39±0.063 [CBG]) following DMM (Fig. 1C). These results show a significant effect of both CBD oil and CBG oil treatments in normalizing gait changes in OA mice.
CBD oil and CBG oil treatments ameliorate cold allodynia with no significant changes in mechanical allodynia in OA mice
To determine changes in stimulus-evoked nociception, we performed the von Frey test. The von Frey test determines changes in mechanical allodynia by manually applying a microfilament to the paw and measuring the threshold needed to evoke a withdrawal response. 36 Two weeks following DMM, von Frey test showed a significant reduction in the response threshold in vehicle-treated DMM mice (3.58±0.96) relative to sham-operated mice (8.71±0.79), indicating the development of mechanical allodynia (Fig. 1D). Four weeks following DMM, mechanical allodynia was maintained at a similar level (3.16±0.64) to week 2 (3.58±0.96) in vehicle-treated DMM mice. At 6 and 8 weeks post-DMM, the withdrawal thresholds were not statistically different from the earlier time points (Fig. 1D) (4.25±0.39 and 5.64±0.58, respectively). Neither CBD oil, nor CBG oil had an effect on mechanical allodynia throughout the disease course in DMM mice (Fig. 1D).
As we did not find an effect of CBD oil or CBG oil on mechanical allodynia in DMM mice, we performed the acetone evaporation test to determine the effects of treatments on cold allodynia. The acetone evaporation test determines changes in cold allodynia in response to acetone application by measuring the time to elicit a nocifensive behavior. 36 CBD oil and CBG oil-treated DMM mice showed significantly reduced cold allodynia as reflected in their increased response times (12.79±2.20 and 13.42±2.30, respectively) (Fig. 1E).
CBD oil and CBG oil treatments have no effect on locomotor activity in OA mice
Next, we performed open-field experiments to evaluate the general locomotor activity of DMM mice under different treatments. 37 No significant changes in locomotor activity parameters were detected in the DMM mice receiving vehicle treatment versus sham-operated mice (Fig. 2). Neither CBD oil nor CBG oil treatment exerted an effect on locomotor activity of DMM mice (Fig. 2). Altogether, these results show that the locomotor activity of mice did not change 8 weeks following DMM with no effect of CBD oil or CBG oil treatment.

CBD oil and CBG oil do not affect the locomotor activity of PTOA mice.
Both CBG oil and CBD oil ameliorate synovitis in OA mice
A common characteristic of OA is synovitis, inflammation of the synovium that is characterized by thickening of the synovial membrane. 38 Eight weeks following DMM, vehicle-treated mice had significantly increased synovial thickness (0.0211±0.0020) in comparison to sham-operated mice (0.0115±0.0012). DMM mice treated with CBD oil or CBG oil had significantly reduced synovial membrane thickness (0.0116±0.0016 and 0.0137±0.0020, respectively) in comparison to vehicle-treated DMM mice (Fig. 3A, C and yellow arrows in Fig. 3B). These results suggest that both CBD oil and CBG oil exert significant anti-inflammatory effects in DMM OA models.

Treatment with CBD oil or CBG oil ameliorates synovitis in PTOA mice.
Treatment with CBG oil, but not CBD oil, is chondroprotective in OA mice
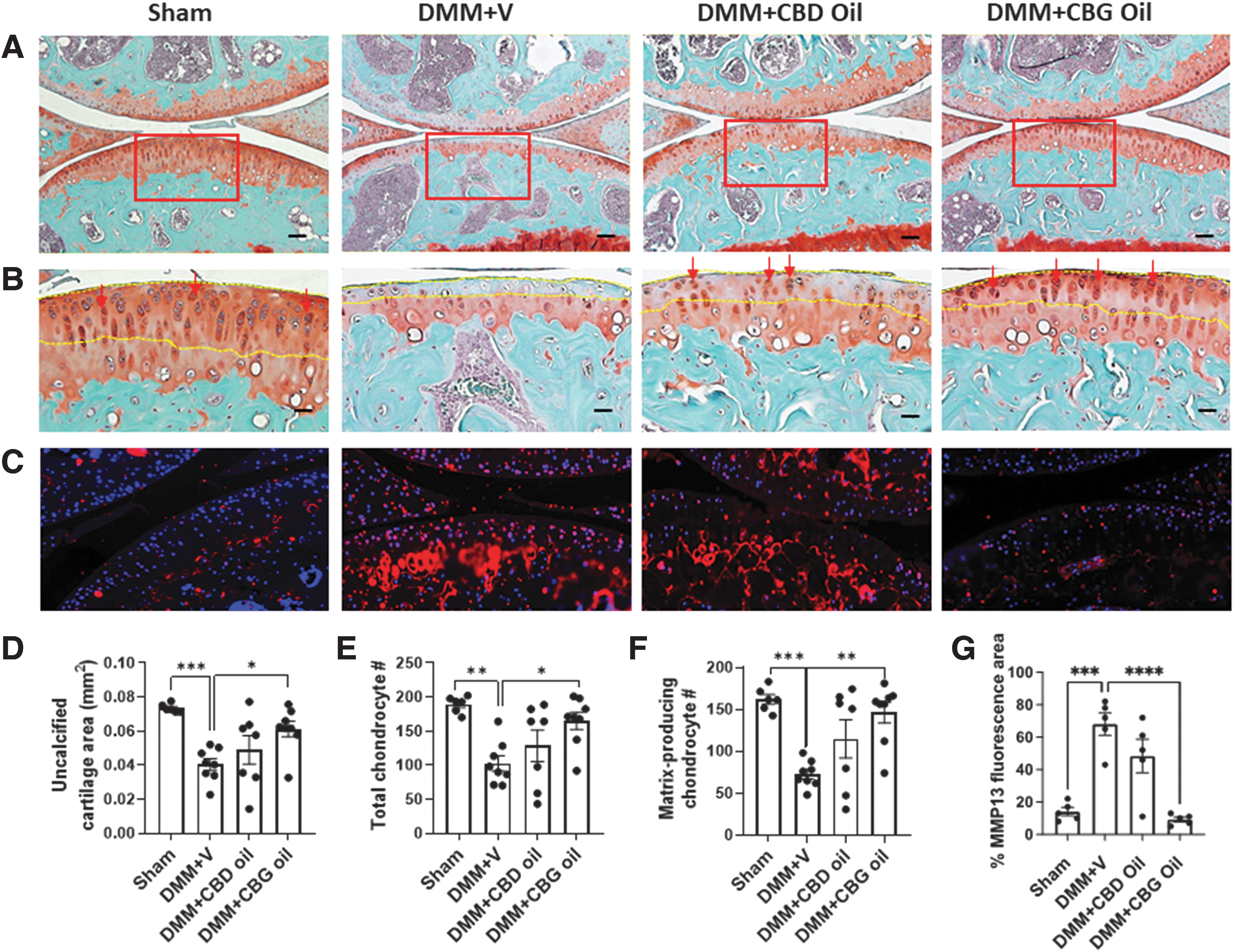
Safranin-O Fast/Green staining showed significant cartilage degeneration in vehicle-treated DMM mice (0.0402±0.0034) in comparison to sham-operated mice (0.0734±0.0010), 8 weeks following DMM (Fig. 4A, D). This cartilage degeneration was significantly ameliorated in DMM mice treated with CBG oil (0.0611±0.0045), but not CBD oil (0.0489±0.0082) (Fig. 4A, and yellow dotted line in Fig. 4B) as shown in the histomorphometric analysis of the uncalcified tibial cartilage area (Fig. 4D). Furthermore, the number of total chondrocytes was significantly reduced in vehicle-treated DMM mice (102.5±11.22) and was significantly preserved with CBG oil treatment (165±12.61) (Fig. 4E). Altogether, these data indicate a chondroprotective effect of CBG oil; importantly, CBD oil did not exert this effect.
Treatment with CBG oil, but not CBD oil, is chondroprotective and chondroregenerative in PTOA mice.
The number of the matrix-producing chondrocytes was also significantly reduced in vehicle-treated DMM mice (72.67±5.6), and was significantly preserved by CBG oil treatment (red arrows in Fig. 4B and Fig. 4F), indicating preserved anabolic signaling in chondrocytes of CBG oil-treated DMM mice (146±12.43).
Finally, we determined changes in the expression of the catabolic enzyme MMP13 by IF staining (Fig. 4C). MMP13 expression was significantly elevated in vehicle-treated DMM mice (68±6.877) in comparison to the sham group (14±2.51), which was significantly reduced by CBG oil (9.2±1.428) and not CBD oil treatment (48.4±10.33) (Fig. 4C, G). Altogether, this indicates that CBG oil, but not CBD oil, exerts a chondroprotective effect and a potential matrix-regenerative effect in OA mice by preserving the anabolic phenotype of chondrocytes.
Neither CBD oil nor CBG oil affect cannabinoid receptor type 2 expression in the synovium or cartilage of OA mice
CB2 receptor is reported to play an anti-inflammatory effect in the synovium and a protective role in chondrocytes in OA.39,40 Therefore, we investigated changes in the expression of CB2 receptor using IF staining. We found that CB2 receptor expression trended toward a reduction in the synovium of vehicle-treated DMM mice, and trended toward an increase with CBD oil and CBG oil treatment (Supplementary Fig. S1A, B). In articular chondrocytes, CB2 receptor expression did not change following DMM or by different treatments (Supplementary Fig. S1C, D).
Neither CBD oil nor CBG oil treatment affect the subchondral bone of OA mice
Finally, we investigated the effect of CBD oil and CBG oil treatment on subchondral bone change in OA. Micro-CT 3D reconstructions of the knee joints of sham and vehicle-treated DMM mice showed that vehicle-treated DMM mice exhibited increased joint mineralization particularly at the medial side (black arrow in Fig. 5A), and irregular bone surface of both the tibia and femur (red arrows in Fig. 5A). These changes were reflected in increased total volume (TV) (0.0697±0.0053) (Fig. 5B) that was significantly reduced only in the CBG oil-treated mice (0.0496±0.0045) (Fig. 5B). There was no change in BV (Fig. 5C) in between experimental groups. BV/TV ratio (BV/TV; Fig. 5D) was significantly reduced in the vehicle-treated DMM mice (0.0496±0.0045), suggesting increased bone porosity in OA mice. This was in parallel with a significant increase in trabecular spacing (Tb.Sp; 0.0519±0.0027) (Fig. 5E) and a trend toward reduced bone mineral density (BMD; 597.5±41.68) (Fig. 5F) of the subchondral bone in these mice.
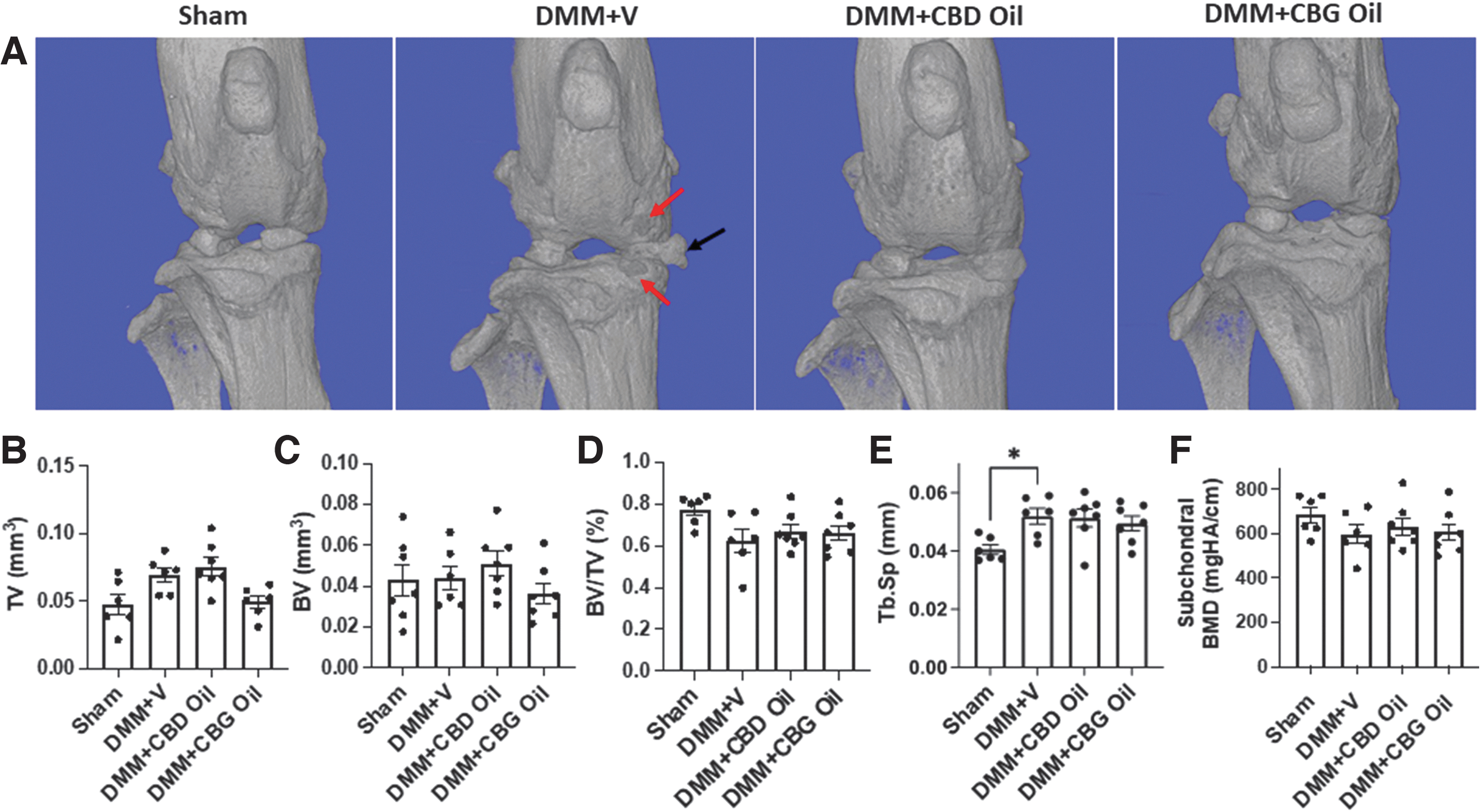
Treatment with CBG oil or CBD oil exerts no effect on changes in the subchondral bone of PTOA mice. Microstructural assessment of subchondral bone changes, using micro-CT, in sham (n=6) and DMM mice receiving treatment with vehicle (V; n=6), CBD oil (n=7), or CBG oil (n=7).
These pathological changes were not altered by CBD oil and CBG oil treatments (Fig. 5D–F). Finally, trabecular number (TB.N) (Supplementary Fig. S2A), trabecular thickness (Tb.Th) (Supplementary Fig. S2B), and subchondral plate thickness (Supplementary Fig. S2C) were not different in between the experimental groups.
Discussion
In the current study, we determined the effects of chronic treatment with cannabis extracts, CBD oil and CBG oil, on OA pain and joint structural changes during OA development and progression. There is limited scientific evidence supporting the efficacy of cannabis extracts in OA pain management, where some studies report the efficacy of pure CBD and synthetic cannabinoids in attenuating pain in inflammatory pre-clinical OA models that are of limited clinical relevance.7,10,23,40 Our study, using the clinically relevant DMM mouse model, showed that both CBD oil and CBG oil ameliorate sensitivity to cold pain and synovitis, and normalize OA-induced changes in gait and locomotor activity. Importantly, only CBG oil displayed chondroprotective and potential chondroregenerative effects in OA mice.
DMM is a surgical OA model that replicates aspects of clinical post-traumatic OA (PTOA): allodynia, 41 synovial inflammation, 42 cartilage degeneration, 42 and bone remodeling. 42 It is widely used as a reproducible, slowly progressing PTOA mouse model, where chondrocyte differentiation, hypertrophy, and loss—the main mechanisms for cartilage degeneration and disease progression in human OA—are reproduced in DMM joints.43,44 DMM leads to phenotypic changes within the joint characterized by an early phase of acute inflammation, followed by chondrocyte loss, cartilage degeneration, and some fibrillation evident by 8 weeks following surgery.29,45
To gain better insights into the effects of treatments on OA development and progression, we analyzed the gait changes in sham and DMM mice with different treatments. Movement-evoked pain is an early characteristic of OA and gait pattern may be altered to protect injured limbs from loading and motion. 33 Gait analysis is a method of studying nonstimulus-evoked nociception and it has been used to study changes in limb movement and positioning in many disease models in mice, such as Parkinson's disease, spinal cord injury, and stroke. 36
In our study, both CBD oil and CBG oil ameliorated the deterioration in the gait of DMM mice starting from early stages of the disease and until 8 weeks. Changes in gait in early OA are attributed to pain, whereas gait changes in later stages of this disease are attributed to both pain and dysfunction due to cartilage degeneration and joint remodeling. 33 However, CBD oil did not exert chondroprotective effects, which supports its antinociceptive and anti-inflammatory effects as the main players in the observed improvement in the gait of OA mice.
Allodynia, increased sensitization to pain, characterizes clinical OA and is replicated in DMM mice, 41 where synthetic CBG derivatives, but not pure CBG 46 or pure CBD, 47 inhibit mechanical pain sensitivity in inflammatory arthritis. In our study, CBD oil or CBG oil treatments did not exert analgesic effects on mechanical allodynia throughout the course of DMM. Conflicting evidence for the development of mechanical allodynia in OA mice is reported in the literature, where researchers could 48 or could not 49 detect the development of mechanical allodynia in DMM mice 8 weeks following surgery. We detected mechanical allodynia starting from the early stage (week 2) of OA in DMM mice, which continued until week 8; although mechanical allodynia appeared to be less pronounced at the later time points, it was not significantly different from early onset OA.
Considering the effect of cannabis extracts in improving gait, and the lack of effect on mechanical allodynia, we performed the acetone test to detect changes in cold allodynia, finding that both CBD oil and CBG oil ameliorate cold allodynia in DMM mice. The discrepancy in the effect of cannabis extracts on mechanical versus cold allodynia can be attributed to their antagonist effect on transient receptor potential melastatin-8 (TRPM8). TRPM8 is a nonselective cation channel and a neuronal sensor that is stimulated by cold temperature and plays a significant role in pain perception, 50 where TRPM8 activity is increased in OA.47,51 Importantly, both CBD and CBG act as TRPM8 antagonists at nanomolar concentrations. 52 Altogether, this suggests reduced TRPM8 activity by CBD oil and CBG oil as a potential mechanism for their effect in ameliorating cold allodynia in DMM mice.
Impaired locomotor activity and altered gait pattern can be the result of both pain and joint remodeling in OA, with different literature reports of changes in the locomotor activity of DMM mice. Eight weeks following DMM, Miller et al. found decreased locomotor activity in DMM mice, which was lost at week 16. 53 On the other hand, Sambamurthy et al. found altered locomotor activity in comparison to the nonoperated controls, but not in comparison to the sham-operated animals 54 ; which supports our findings with no changes in locomotor activity of vehicle-treated DMM mice 8 weeks following surgery, relative to sham-operated mice. Finally, Alves et al. found no changes in locomotor activity of mice 12 weeks following DMM, 49 also in agreement with our findings.
In spite of the lack of change in locomotor activity, we found significant impairment of the gait in vehicle-treated DMM mice, which was improved by both CBD oil and CBG oil treatment. Impaired gait in DMM mice was reported by others with a trend in early/mid stages of OA that reached significance at week 12. 55 Others found no change in the gait of mice 5 weeks following DMM with significant impairment at week 10. Our results suggest that increased cold allodynia from week 2 to 8 following DMM correlated with impaired gait, with no detectable changes in locomotor activity; both cold allodynia and gait were improved by CBD oil and CBG oil treatment. It is noteworthy that reduced cartilage degeneration by CBG oil and not CBD oil treatment was not a contributing factor to changes in pain and gait of DMM mice, as both treatments were equally effective in ameliorating cold allodynia and gait impairment.
It is now understood that OA is a disease of the whole joint, with no disease-modifying therapy available. Recently, the correlation between pain, synovitis, and cartilage degeneration in OA is gaining more appreciation. 9 Synovitis is caused by the increased inflammatory cell infiltration to the synovium, which leads to increased production of inflammatory mediators that trigger chondrocyte inflammatory and hypertrophic signaling and inhibit anabolic signaling. 38 Therefore, in OA, synovitis directly promotes cartilage degeneration and vice versa through cartilage/synovium crosstalk. The ECS has been documented in the cartilage and synovium of human14,19 and pre-clinical arthritis models,7,10,18,39 suggesting a role in OA development and progression. Synovitis peaks in early stages post DMM surgery before declining, where it persists, at levels that remain higher than those of sham mice, throughout mid and late stages of PTOA. 38
We found that both CBD oil and CBG oil attenuated synovial inflammation in mice 8 weeks following DMM. These findings are corroborated by other studies showing that pure CBD is effective in attenuating inflammation in rat inflammatory arthritis, 30 and that both pure CBD10,22,56,57 and pure CBG24,25,58,59 are effective in attenuating inflammation in other inflammatory diseases. Of relevance, we found a downward trend of CB2 receptor expression in the synovium of DMM mice, which trended upward with CBD oil and CBG oil treatment. This corroborates the reported anti-inflammatory effect of CB2 receptor in the synovium of rheumatoid arthritis. 60
Increased joint innervation and neurogenic inflammation play a major role in exacerbating synovitis and in increased pain sensitivity in OA. The normally aneural articular cartilage becomes innervated by sensory and sympathetic nerve fibers in mild and severe stages of human OA. 61 This increased joint innervation leads to high levels of neuropeptides in the joint that correlate with increased pain sensitivity, angiogenesis, and inflammatory cell infiltration, therefore increasing inflammation 62 and OA severity. 63 On the contrary, some studies have shown reduced sensory innervation in the synovium during acute inflammation in human samples, 64 and in inflammatory OA mouse model. However, this sensory innervation increased in mid/late stage OA and correlated with pathological joint remodeling. 65 Of relevance to our model, DMM mice had increased expression of calcitonin gene-related peptide (CGRP) in the sensory nervous system correlating with increased allodynia 12 weeks after DMM. 49
Importantly, cannabinoids can dose dependently decrease neurogenic inflammation by preventing neuropeptide release from primary afferent nerve endings through their effect on cannabinoid receptors CB1, CB2, and TRPV1. 15 Finally, both CBD15,22 and CBG 24 were shown to directly reduce neurogenic inflammation. Altogether, this supports a role for CBD oil and CBG oil in ameliorating neurogenic inflammation, thus reducing both synovitis and pain in DMM mice.
Reports support the protective effects of synthetic cannabinoids in attenuating chondrocytes' hypertrophic differentiation in vitro,39,40,66 with CB2 receptor playing a major role.39,40 In addition, a synthetic CB2 agonist ameliorates OA development in DMM mice. 39 We found that CBG oil prevents cartilage degeneration and chondrocyte loss in DMM mice, with impressive preservation of cartilage matrix. Mechanistically, we found attenuated chondrocyte hypertrophy by CBG oil, as reflected in reduced protein expression of the chondrocyte hypertrophy marker, MMP13. Furthermore, CBG oil exerted an anabolic effect as reflected by an increase in the number of matrix-producing chondrocytes. This supports previous reports of the protective effects of CB2 receptor in chondrocytes in vitro, where it prevents the secretion of cartilage-degrading enzymes and promotes the production of aggrecan, a major cartilage matrix component.39,40 Of note, there was no change in chondrocyte CB2 receptor expression among all groups in our study.
The lack of chondroprotective effects with CBD oil treatment suggests that CBG is responsible for the chondroprotective effect of CBG oil. While CBG was shown to act as an agonist at the CB2 receptor,28,32 CBD has been demonstrated to act as an antagonist67,68 and as a partial agonist of the CB2 receptor. 69 This supports CB2 receptor agonism by CBG as an underlying mechanism for the observed chondroprotective effect of CBG oil in OA mice. As we recently reviewed, 32 CBG is a potent agonist at serotonin type 1a, alpha-2 adrenergic receptors, and PPAR receptors, in addition to traditional cannabinoid receptors. Therefore, further studies with pure CBG and specific agonists and inhibitors of these receptors are necessary to elucidate the mechanisms behind these chondroprotective effects of CBG oil.
In OA, the subchondral bone undergoes remodeling with increased porosity in early/mid stages of the disease, followed by sclerosis in later stages. 70 Subchondral bone changes may also contribute to pain chronification in OA.17,41,71 Several reports showed that cannabinoids influence bone structure by regulating bone cell differentiation, survival, and function mainly through CB2 receptor, with the most important outcome being increased bone mass. 7 Our data show that although CBG oil-treated mice had less mineralization at the medial side of the joint, it exerted no effect on the subchondral bone structure of OA mice. This may be due to the dose and route of administration we used, where there is less systemic drug distribution. We chose to inject the oils subcutaneously in the knee region, which is the closest simulation of topically and locally applied oils by OA patients.
This treatment regimen maintained plasma levels at 735.87±291.74 ng/mL CBD in CBD oil-treated mice, and 473.58±141.46 ng/mL CBD and 452.35±222.22 ng/mL CBG in CBG oil-treated mice (Supplementary Table S1). The dose we used had no effect on behavior, as recently reported with CBD. 72 Furthermore, there was no change in the body weight of mice receiving CBD oil or CBG oil treatment in comparison to vehicle-treated or sham-operated mice (data not shown), as it was also previously reported with CBD. 72 These results support a promising clinical application of cannabis extracts in OA with no side effects, considering the significant pain-reducing and disease-modifying effects we found in OA mice.
There is an incredible demand to develop a treatment that reduces pain and stops or reverses the pathological joint changes in OA. 7 Thus, recent research has been focusing on targeting the ECS for cartilage, bone, and synovium homeostasis to discover novel therapies in efforts to prevent further progression of OA. 7 At the same time, the use of cannabis oils to control pain in OA is increasing among the public. Our study provides scientific evidence for the efficacy of CBD and CBG oils in pain control in OA, with a chondroprotective and a potential chondroregenerative effect of CBG oil, suggesting it as a DMOAD. Future clinical studies will determine the extent of this therapeutic efficacy in OA patients.
Authors' Confirmation Statement
All authors met the ICMJE authorship criteria.
Footnotes
Acknowledgments
The authors would like to acknowledge the members of the Pennsylvania-approved Medical Marijuana Academic Clinical Research Center at Penn State for discussions and support.
Author Disclosure Statement
The authors have nothing to disclose.
Funding Information
F.K. is the recipient of research support from the NIH NIAMS R01 AR071968; R.A.E. is the recipient of research support from the NIH NIDDK R01 DK121327; K.E.V. and the Penn State College of Medicine are the recipients of research support from PA Options for Wellness, a Pennsylvania-approved Medical Marijuana Clinical Registrant. The Penn State College of Medicine is a Pennsylvania-approved Medical Marijuana Academic Clinical Research Center.
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.