
Abstract
Introduction:
Cannabidiol (CBD) is primarily consumed through ingestion and inhalation. Little is known about how CBD pharmacokinetics differ between routes of administration, and duration of pulmonary exposure.
Methods:
Pharmacokinetics, brain distribution, and urinary elimination of CBD and its major metabolites (6-hydroxy-cannabidiol [6-OH-CBD], 7-hydroxy-cannabidiol [7-OH-CBD], 7-carboxy-cannabidiol [7-COOH-CBD], and CBD-glucuronide) were evaluated in adult Sprague-Dawley rats following a single oral CBD ingestion (10 mg/kg in medium chain triglyceride oil; 24 male animals), and 1 or 14 days of repeated inhalation (0.9–13.9 mg/kg in propylene glycol [41%/59% by weight]; 5 male and 5 female animals per dose). Blood and brain tissue were collected at a single time point from each animal. Collection times were staggered from 5 min to 24 h postoral gavage or first (blood only) and final inhalation. Urine was collected 24 h postoral gavage or final inhalation. Samples were analyzed through liquid chromatography–mass spectrometry (LC-MS/MS).
Results:
CBD was more rapidly absorbed following inhalation than ingestion (Tmax=5 min and 2 h, respectively). Inhalation resulted in a dose–responsive increase in CBD Cmax and AUClast. CBD Cmax was 24-fold higher following the highest pulmonary dose (13.9 mg/kg) versus an oral dose of comparable concentration (10 mg/kg). Cmax and AUClast (0–16 h) trended higher following repeated exposure. Elimination was notably faster with repeated CBD inhalation (t1/2=5.3 and 2.4 h on days 1 and 14, respectively). While metabolites were detectable in plasma, AUClast (0–2 h) was at least 10- (7-OH-CBD, 7-COOH-CBD) to 100- (6-OH-CBD) fold lower than the parent compound. Metabolite concentration trended higher following repeated inhalation (6.7 mg/kg CBD); AUClast (0–16 h) was ∼1.8-, ∼1.4-, and ∼2.4-fold higher following 14 days of exposure for 6-OH-CBD, 7-OH-CBD, and 7-COOH-CBD, respectively. CBD was detectable in brain homogenate tissue 24-h after 14-day inhalation (>3.5 mg/kg deposited dose) or a single oral administration. CBD metabolites were only measurable in brain tissue following the highest inhaled dose (13.9 mg/kg CBD). CBD, but not metabolites, was detectable in urine for all dose groups following 2 weeks of CBD inhalation. Neither CBD nor metabolites were present in urine after oral administration.
Conclusion:
CBD pharmacokinetics differ across oral and pulmonary routes of administration and acute or repeated dosing.
Introduction
Cannabidiol (CBD) is a phytocannabinoid of increasing interest for its purported health benefits, including antidepressant, anxiolytic, anti-inflammatory, and anticonvulsant effects,1–4 but more research is needed to identify appropriate dose levels and frequency of administration.5,6 The main routes for human cannabinoid consumption are ingestion and inhalation; both are thought to result in low bioavailability (<20% and ∼31% following oral and pulmonary delivery, respectively).3,7 Inhalation may improve cannabinoid delivery into systemic circulation by circumventing the pharmacokinetic variability associated with gastrointestinal absorption and first-pass hepatic metabolism. 8
Few publications have explored systemic CBD concentration following inhalation exposure. In Wistar rats, acute oral administration of cannabinoids has been shown to delay peak serum levels and prolong blood and brain exposure as compared with inhalation through vaporizer. 9 CBD vapor inhalation was shown to result in dose-related plasma CBD levels in both male and female animals. 10 In humans, a single inhaled dose of CBD dry powder or crystalline isolate resulted in more rapid absorption and improved systemic delivery than an oral dose of equal or higher concentration.8,11 Whether CBD pharmacokinetics differ between acute versus repeated pulmonary administration is unknown.
Primary CBD metabolic reactions in the liver are catalyzed by cytochrome P450 (CYP) enzymes and include allylic hydroxylation at the six- and seven positions.12,13 While there are known interspecies differences in CYP isoenzyme expression, 14 and cannabinoid metabolism differs by species,15–17 shared rat and human metabolites include 6-hydroxy-cannabidiol (6-OH-CBD), 7-hydroxy-cannabidiol (7-OH-CBD), and 7-carboxy-cannabidiol (7-COOH-CBD), the product of 7-OH-CBD biotransformation.2,18 Animal studies indicate that CBD is largely excreted intact or in its glucuronide form through urine and feces.2,18–20 In humans, oral CBD administration has been shown to result in slower elimination and ∼3-fold higher urinary CBD concentration than vaporized CBD. 21 Little is known about how CBD metabolism and excretion differ between acute and subchronic inhalation.
The aims of the present study were to (1) evaluate acute CBD and metabolite pharmacokinetics across oral and pulmonary routes of CBD administration; and (2) compare the pharmacokinetic profiles of CBD and metabolites following acute versus 14-day repeated delivery of multiple doses (0.9–13.9 mg/kg) of inhaled CBD in rats. To this end, we used a nose-only exposure method, which avoids particle entry through other routes and therefore evaluates inhalation more accurately. 22
Materials and Methods
The experimental design is summarized in Figure 1. Detailed methods can be found in the Supplementary Data S1. In brief, for the ingestion study, rats (n=24 males) received a single oral gavage of 10 mg/kg CBD in medium-chain triglyceride (MCT) oil. Blood and brain tissue were collected from three animals per necropsy time point at 5 and 30 min, and 1, 2, 4, 8, 16, and 24 h postdose. Urine was collected from animals euthanized at 24 h postdose only. Each animal was sampled at one time point only. For the inhalation study, Sprague-Dawley rats (n=65; 35 males, 30 females) were divided into 6 groups. Groups 1–4 and 6 included five males and five females per group. Group 5 included an additional 5 males (n=15 total; 10 males, 5 females) to accommodate additional blood draws and allow for comparison of later time points (2–16 h) against oral dosing. Animals were exposed to filtered air (3 h; group 1) or CBD formulated in propylene glycol (PG) at a target concentration of 1.0 mg/L CBD and 1.3 mg/L PG (12, 23, or 45 min, 1.5 or 3 h; groups 2–6, respectively) through nose-only inhalation once daily for 14 consecutive days.
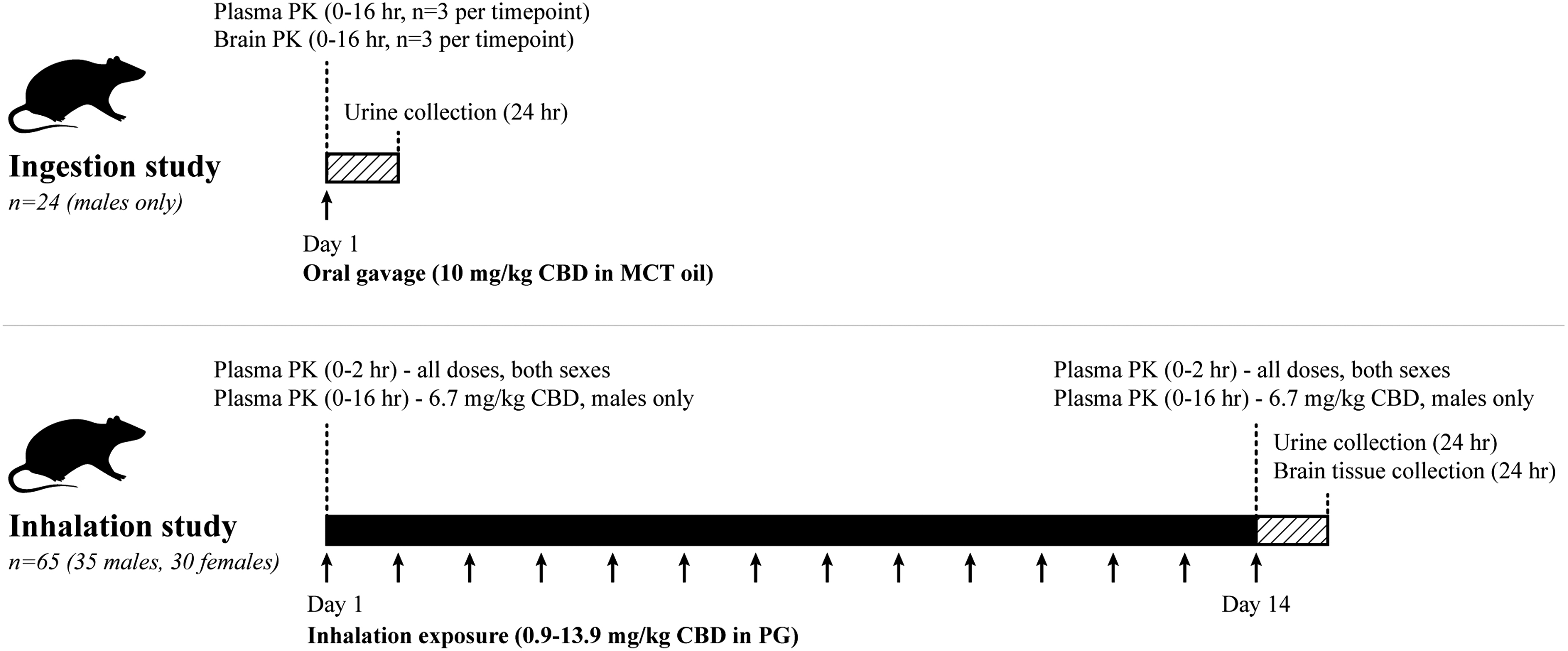
Summary of experimental design.
Blood was collected 5 min (groups 1–6, n=5 per sex per group), 30 min, 1 h, and 2 h (groups 2–6, n=5 per sex per group), and 4, 8, and 16 h (group 5, n=5 males only) postfirst and final exposures. Urine and brain tissue were collected 24 h postfinal dose. Samples were analyzed for CBD, 6-OH-CBD, 7-OH-CBD, and 7-COOH-CBD (plasma, urine, and brain tissue), and CBD-glucuronide (urine only) through liquid chromatography–mass spectrometry (LC-MS/MS). All urine samples, and plasma and homogenized brain tissue samples from orally dosed animals, were analyzed using a Sciex API 4000 paired with a Waters Acquity H-Class Ultra Performance Liquid Chromatography (quantification range=4–2000 ng/mL). Plasma and homogenized brain tissue from animals dosed through inhalation were analyzed using a Sciex Triple Quad 6500+ paired with a Shimadzu Nexera X2 Ultra-High-Performance Liquid Chromatography (quantification range=0.25–250 ng/mL). Methods were partially validated (Supplementary Data S2).
Calibration standards and quality control samples were prepared in the equivalent naive matrix. Standard curve parameters for calibration standards in rat plasma, brain, and urine matrices are listed in Supplementary Table S1. All animal work complied with the Final Rules of the Animal Welfare Act regulations (9 CFR Parts 1, 2, and 3) and the Guide for the Care and Use of Laboratory Animals. 23
Results
Oral dosing pharmacokinetics
CBD and all measured metabolites were detected in plasma within 5 min of oral dosing (Fig. 2). Time of maximal concentration (Tmax) was estimated at 2 h for all analytes (Table 1). Maximal concentration (Cmax) and area under the curve from dosing to time of the last measured concentration (AUClast) were highest for CBD and 7-COOH-CBD. This was also reflected in the metabolite to parent ratios, which were 0.5 for Cmax and 1 for AUClast compared with ratios of 0.2 or lower for 6- and 7-OH-CBD. The 6- and 7-OH-CBD were below the quantification limit (BQL) ≥8 h after dosing; CBD and 7-COOH-CBD remained quantifiable 24 h after dosing. Terminal elimination half-life (t1/2) was only calculatable for CBD (4.2 h) and 7-COOH-CBD (2.7 h).

Mean±SD plasma and brain concentration (ng/mL) of CBD and metabolites following a single oral dose of CBD (10 mg/kg in MCT oil, oral gavage) in Sprague-Dawley rats (0–24 h postdose; n=3 males per time point, n=24 males total). CBD, cannabidiol; MCT, medium chain triglyceride; SD, standard deviation.
Pharmacokinetic Parameters of a Single Ingested Dose of Cannabidiol (10 mg/kg in Medium Chain Triglyceride Oil, Oral Gavage) in Plasma and Brain of Sprague-Dawley Rats (0–24 h Postdose; n=3 Males Per Time point/Group)
Values shown are median for Tmax, mean±SE for Cmax, and AUClast and population-level estimates for remaining PK parameters.
BQL was 0.25 ng/mL for plasma and 1.25 ng/g for brain.
Metabolite to parent ratios were calculated with adjustments for molecular weights as follows: CBD=314.5 g/mol, 6- and 7-OH-CBD=330.5 g/mol, 7-COOH-CBD=344.4 g/mol.
6-OH-CBD, 6-hydroxy-cannabidiol; 7-COOH-CBD, 7-carboxy-cannabidiol; 7-OH-CBD, 7-hydroxy-cannabidiol; AUClast, area under the curve from dosing to time of the last measured concentration; BQL, below quantitative limit; CBD, cannabidiol; Cmax, maximal concentration; MPR, metabolite to parent ratio; NC, not able to be calculated; PK, pharmacokinetics; SE, standard error; t1/2, half-life; Tmax, time of maximal concentration.
Brain and urine
In brain, CBD, 6-OH-CBD, and 7-OH-CBD were detected within 5 (CBD) or 30 min (metabolites) of oral dosing (Fig. 2). Tmax was estimated at 2 h for all detectable analytes (Table 1). Cmax and AUClast were highest for CBD. The 6- and 7-OH-CBD (approximately equivalent concentrations in brain) had metabolite to parent ratios of 0.07 for Cmax and 0.05 for AUClast. All analytes were BQL ≥8 h after dosing. Brain t1/2 was only calculatable for CBD (2.0 h). All analytes were BQL in urine (collected 24 h after dosing).
Pulmonary dosing pharmacokinetics
Inhalation exposure and pulmonary doses
Mean aerosol concentration for CBD and PG was 1.02 and 1.26 mg/L, respectively, resulting in daily presented/deposited doses of CBD ranging from 8.9/0.9 to 138.5/13.9 mg/kg (Table 2). Average daily presented/deposited doses of PG ranged from 11.3/1.1 to 176.0/17.6 mg/kg. Aerosol mass median aerodynamic diameter was 1.4 μm (geometric standard deviation=2.1).
Summary of Daily Cannabidiol Inhalation
Mean±SD.
Presented/deposited dose is calculated using the following formula: Dose=(C×RMV×T×DF)/BW; C (mg/L)=average total aerosol concentration, RMV=0.608×BW0.852, BW (kg)=body weight, T (min)=exposure time, DF is assumed to be 100% for the presented dose and 10% for the pulmonary deposited dose. 24
Additional five male animals in this group were used for late PK time points (2–16 h) to allow for comparison against oral dosing.
DF, deposition fraction; F, female; M, male; N, number of animals; PG, propylene glycol; RMV, respiratory minute volume; SD, standard deviation.
Single-dose pharmacokinetics
CBD and all measured metabolites were detected in plasma within 5 min of pulmonary dosing across exposure groups (Figs. 3 and 4). Across analytes, Tmax (0–2 h) ranged from 5 min to 2 h, with higher CBD doses generally associated with increased Tmax (Table 3). Across exposure levels, Cmax and AUClast (0–2 h) were highest for CBD, followed by 7-COOH-CBD >7-OH-CBD >6-OH-CBD. Terminal elimination half-life (t1/2) could generally not be calculated or is not reported because acceptance criteria were not met (terminal elimination phase adjusted R2>0.70 and %AUClast extrapolated in the terminal phase <30%). The few estimated values indicate t1/2 ∼1 h for CBD and 7-OH-CBD.
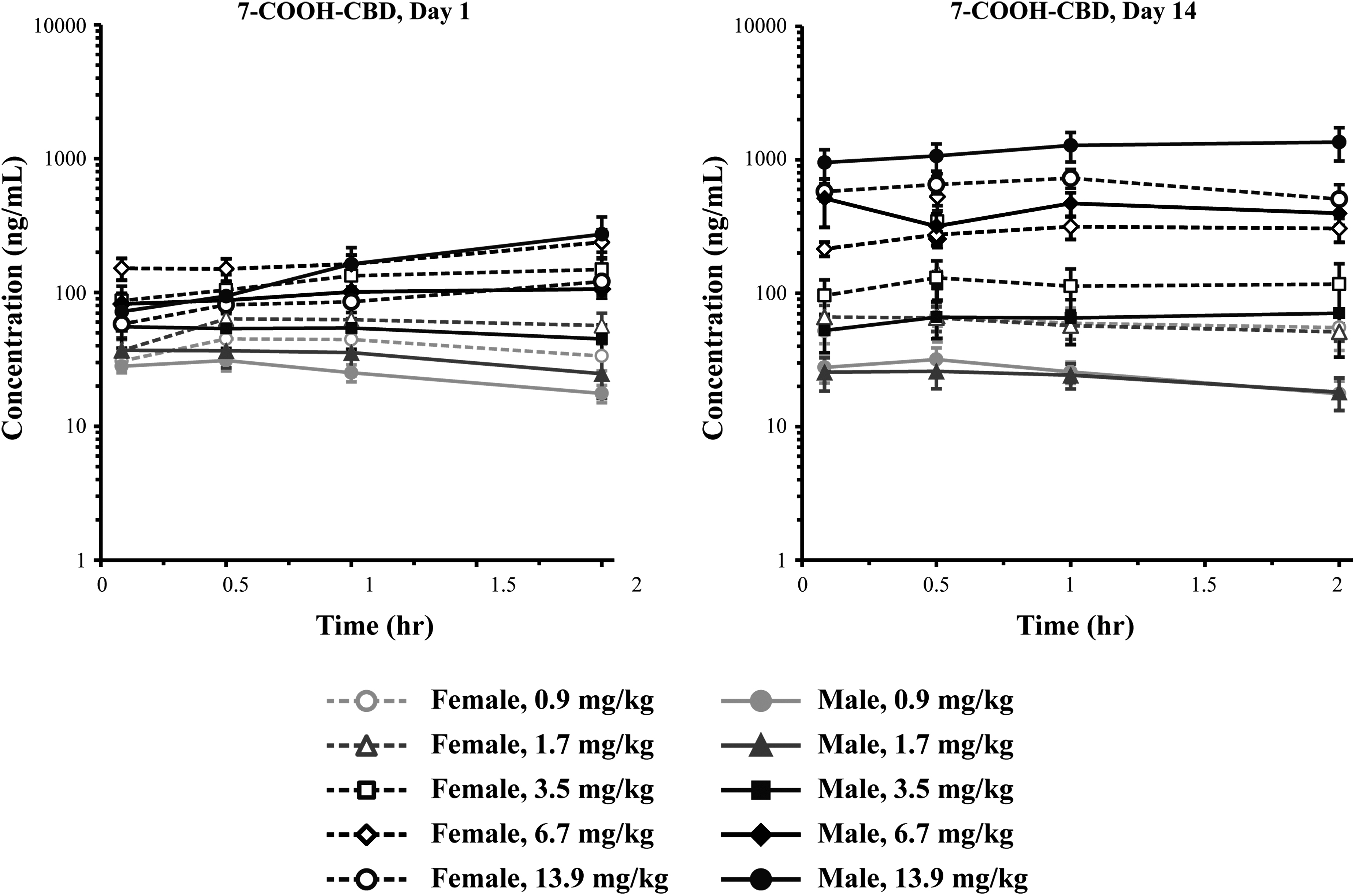
Mean±SEM plasma concentration (ng/mL) of CBD and metabolites following single or 14-day CBD inhalation (0.9–13.9 mg/kg in 41%/59% PG by weight) in Sprague-Dawley rats (0–2 h postexposure; n=5 per sex per group). PG, propylene glycol; SEM, standard error of the mean.
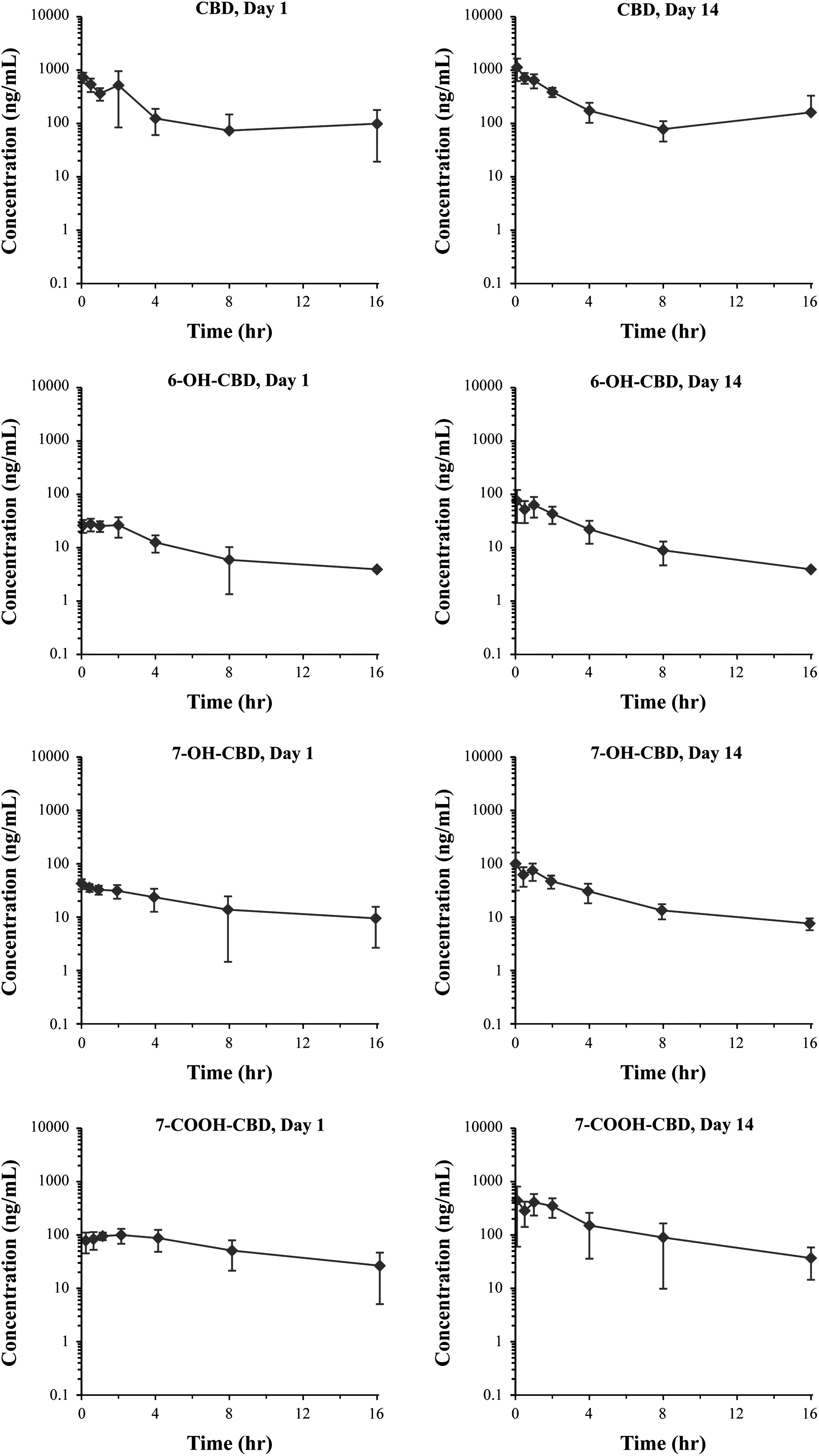
Mean±SD plasma concentration (ng/mL) of CBD and metabolites following single or 14-day CBD inhalation (6.7 mg/kg in 41%/59% PG by weight) in Group 5 Sprague-Dawley rats (0–16 h postexposure; n=10 males).
Pharmacokinetic Parameters of Cannabidiol and Metabolites in Plasma Following Cannabidiol Inhalation (0.9–13.9 mg/kg in 41%/59% Propylene Glycol by Weight) in Sprague-Dawley Rats (0–2 h Postexposure; n=5 Per Sex Per Group)
Values shown are median for Tmax and mean±SD (95% CI) for all other parameters.
Group 6 on day 14 had n=3 for M and n=4 for F.
BQL (4.00 ng/mL).
Ninety-five percent CI does not overlap with group 2.
Ninety-five percent CI does not overlap with group 3.
Ninety-five percent CI does not overlap with group 4.
Ninety-five percent CI does not overlap with group 5.
Ninety-five percent CI does not overlap with group 6.
CI, confidence interval.
In male animals exposed to 6.7 mg/kg CBD, both Tmax and Cmax (0–16 h) were comparable to Tmax and Cmax (0–2 h) across analytes (Table 4). AUClast (0–16 h) was notably higher for CBD (2.7-fold) and metabolites (3.0-, 4.0-, and 5.1-fold for 6-OH-CBD, 7-OH-CBD, and 7-COOH-CBD, respectively). The t1/2 (0–16 h) on day 1 was estimated at 5.29, 2.42, and 3.79 h for CBD, 6-OH-CBD, and 7-OH-CBD, respectively.
Pharmacokinetic Parameters of Cannabidiol and Metabolites in Plasma Following Cannabidiol Inhalation (6.7 mg/kg in 41%/59% Propylene Glycol by Weight) in Group 5 Sprague-Dawley Rat Plasma (0–16 h Postexposure; n=5 Males Per Group/Day)
Values shown are median for Tmax, mean±SE for Cmax and AUClast, and population-level estimates for Cmax/dose and AUClast/dose.
AUClast for inhaled CBD was calculated from 0 to 16 h, while AUClast for oral CBD was calculated from 0 to 24 h. Concentrations were near the quantitative limit of 0.250 ng/mL or BQL at the 24-h time point after oral dose; AUClast for oral and inhaled dosing should be comparable although the final time point is different.
For all analytes, both Cmax and AUClast increased with increasing dose. Following a single inhaled dose, Cmax was dose proportional (6-OH-CBD, male and females; 7-OH-CBD and 7-COOH-CBD, males) or less than dose proportional (CBD, males and females; 7-OH-CBD and 7-COOH-CBD, females) across doses studied (Supplementary Table S2). AUClast was dose proportional (CBD and 6-OH-CBD, males and females; 7-OH-CBD and 7-COOH-CBD, males), or less than dose proportional (7-OH-CBD and 7-COOH-CBD, females) across doses studied.
There was no notable (<0.5- or >2.0-fold) difference in CBD Cmax or AUClast between sexes (Supplementary Table S3). Male animals in the highest dosing group (13.9 mg/kg) had >2-fold higher 6-OH-CBD (both Cmax and AUClast) and 7-COOH-CBD (Cmax only) than females. However, doses of 3.5 and 6.7 mg/kg CBD resulted in lower 7-COOH-CBD levels in males. For 7-OH-CBD, both Cmax and AUClast were consistently lower in male versus female animals (∼0.30- to 0.38-fold across 0.9–6.7 mg/kg CBD groups).
Determination of AUClast/dose ratios for inhaled/oral administration resulted in higher levels of CBD (∼15-fold) and all metabolites (∼5-fold) after single-dose inhalation compared with single oral dosing (Table 4).
Repeated dose pharmacokinetics
CBD and all measured metabolites were detected in plasma following 14 days of once-daily CBD exposure (Fig. 3). Tmax remained at 5 min across most analytes and time points (Table 3). As reported above, Cmax and AUClast were highest for CBD, followed by 7-COOH-CBD >7-OH-CBD >6-OH-CBD across exposure groups.
Both Tmax and Cmax (0–16 h) were comparable to Tmax and Cmax (0–2 h) across analytes for male animals administered 6.7 mg/kg (Table 4). AUClast (0–16 h) was notably higher for CBD (2.6-fold) and metabolites (2.4-, 2.6-, and 2.9-fold for 6-OH-CBD, 7-OH-CBD, and 7-COOH-CBD, respectively). The t1/2 (0–16 h) on day 14 was generally lower than day 1, estimated at 2.40 h, 1.97 h, and 2.21 h for CBD, 6-OH-CBD, and 7-OH-CBD, respectively.
Both Cmax and AUClast increased with increasing dose. Dose proportionality was as reported above for single-dose pharmacokinetics, with the exception of 7-COOH-CBD, which was dose proportional in females and greater than dose proportional in males for both Cmax and AUClast following 14 days of dosing (Supplementary Table S2).
As reported above, there was no notable difference in CBD Cmax or AUClast between sexes following repeated exposure (Supplementary Table S3). The 6-OH-CBD AUClast was also comparable between sexes across exposure groups, whereas Cmax was notably higher (>2.0-fold) in males receiving 0.9 or 6.7 mg/kg CBD. The 7-OH-CBD and 7-COOH-CBD trended lower in males versus females for both Cmax and AUClast.
There was no notable accumulation of plasma CBD following repeated CBD exposure across groups; both Cmax and AUClast were comparable between 1 and 14 days of dosing (Supplementary Table S4). Contrarily, there was notable accumulation (Cmax and/or AUClast ratio >2.0 for day 14 vs. day 1) of 6-OH-CBD, 7-OH-CBD, and 7-COOH-CBD in both males and females that was generally associated with CBD exposure ≥6.7 mg/kg.
Brain and urine
In brain, exposure to 6.7 mg/kg CBD resulted in quantifiable levels of CBD in male (70.4±62.1; p≤0.05 vs. air control) and female (64.1±29.6; not significant) animals. Exposure to 13.9 mg/kg CBD increased CBD brain levels in both males (2449.1±2863.2 ng/mL; p≤0.05) and females (699.5±920.1 ng/mL; p≤0.05). While this dose also resulted in detectable concentrations of 6-OH-CBD, 7-OH-CBD, and 7-COOH-CBD (all ≤60 ng/mL), there was no significant difference from the control group. All CBD metabolites were BQL following CBD doses ≤6.7 mg/kg.
In urine, CBD was detectable in all dose groups. As compared with the air control group, urine CBD concentration was significantly (p≤0.05) higher in both sexes following 6.7 or 13.9 mg/kg and in females following 3.5 mg/kg CBD. Of the metabolites analyzed, only 7-COOH-CBD (3.3 ng/mL) was detected in urine for the highest exposure group, and only in female animals.
Discussion
The present study explored the effects of route of administration (oral vs. inhaled), and inhalation frequency (acute vs. repeated daily dosing) and dose (0.9–13.9 mg/kg) on systemic CBD concentration, metabolism, brain distribution, and urinary excretion in adult Sprague-Dawley rats. Single-dose inhalation resulted in more rapid absorption and higher plasma levels than acute ingestion. Repeated CBD inhalation further improved CBD systemic delivery and increased metabolite concentration. While all measured metabolites were detectable in plasma, their concentration was substantially lower compared with the parent compound. CBD, but not metabolites, was detectable in urine 24 h following inhalation. Importantly, we also report detection of CBD and metabolites in brain tissue following selective oral/inhaled doses and time points.
Direct comparison of pharmacokinetics following oral versus pulmonary routes of administration is difficult. Whereas oral dosing involves delivery of a CBD bolus over a few seconds, inhalation necessitates altering exposure time to achieve each target deposited dose. The time needed for dosing through inhalation and sample collection may inadvertently result in onset of elimination mechanisms during ongoing exposure, leading to differences in the presence and amount of CBD and metabolites across administration routes. In the present study, we observed more rapid absorption after inhalation versus ingestion (Tmax=5 min and 2 h, respectively), and 15-fold higher AUClast/dose following the 6.7 mg/kg pulmonary dose as compared with an oral dose of comparable concentration (10 mg/kg). AUClast after oral gavage was most comparable to that measured after inhalation of a deposited dose of 1.7 mg/kg or lower. Higher CBD bioavailability after inhaled versus oral delivery has been reported in humans. 7
Only one other study has compared acute oral (10 mg/kg) and pulmonary (20 mg, 5 min vaporization) routes of CBD delivery in rats, 9 concluding instead that cannabinoids were best absorbed after oral administration. The design of the nose-only inhalation system reduces ingestion of CBD during postexposure grooming activity and therefore the impact of pharmacokinetics data is considered negligible. Differences in aerosolization method, oral CBD formulation, and sample preparation make the comparison of findings between the two studies challenging. In the present study, CBD was aerosolized and administered through a nebulizer for inhalation, MCT oil was used for oral formulation and plasma samples were collected, whereas Hložek et al vaporized CBD and formulated in sunflower oil, collecting serum samples for determination of CBD pharmacokinetics. 9
The present study is the first to compare CBD pharmacokinetics following a single inhalation versus repeated daily subchronic inhalation in rats. While CBD Tmax was largely unchanged between 1 and 14 days of inhalation, both Cmax and AUClast (0–16 h) trended higher following repeated exposure, in agreement with previous data for repeated oral administration of CBD isolate (in sunflower oil) in dogs 25 and a CBD-dominant cannabis formulation (in MCT oil) in humans. 26 Elimination was notably faster with repeated CBD inhalation (t1/2=5.3 and 2.4 h on days 1 and 14, respectively). In contrast, CBD elimination has been reported to be faster (lower t1/2) after a single acute dose versus 28-day oral CBD administration (1–12 mg/kg) in dogs. 24 Similarly, human oral CBD studies suggest faster elimination following acute (t1/2=1.09 and 1.97 h for 10 and 20 mg, respectively) versus chronic (t1/2=2–5 days, 10 mg/kg daily for 6 weeks) administration.27–29
Discrepancies observed may be a result of enterohepatic recycling following oral administration.30,31 Importantly, human studies have also noted much slower CBD elimination following acute inhalation, with t1/2 of 31±4 h subsequent to 19.2±0.3 mg CBD, than that observed in this study. 32 Whether this is due to species, route of administration, or formulation differences is unclear. Exploring changes in CBD kinetic profile after repeated oral versus inhaled administration was beyond the scope of the present study, but also warrants investigation.
Urinary metabolites of CBD in rats and humans show a preference for C-7 hydroxylation following intravenous and oral delivery. 20 Herein, we confirm that C-7 hydroxylation is also the preferred metabolic route in rat plasma following pulmonary CBD delivery. At lower dose levels, plasma 7-OH-CBD was ∼10 times higher and reached peak plasma concentration sooner (Tmax ∼5 min), whereas 6-OH-CBD showed a delayed peak (Tmax=1–2 h) after CBD administration. Moreover, the lack of dose–response in 6-OH-CBD Cmax and AUClast, and accumulation of both 6- and 7-OH-CBD in higher dose groups suggest daily exposures of ≥6.7 mg/kg CBD result in saturation of cannabinoid elimination pathways in the rat. As 7-OH-CBD is further metabolized to 7-COOH-CBD, peak plasma 7-COOH-CBD occurred last (Tmax=2 h), with plateau in plasma levels until the 2-h time point.
Differences in Cmax and AUClast between dose groups, as well as the accumulation profile, was similar to 7-OH-CBD. While metabolite plasma concentrations were at least 10- (7-OH-CBD, 7-COOH-CBD) to 100 (6-OH-CBD)-fold lower than CBD, their functional significance cannot be precluded. Like CBD, concentration of all measured metabolites trended higher following repeated inhalation. The most notable difference was for 7-COOH-CBD, wherein Cmax and AUClast (0–16 h) were ∼5- and ∼2.5-fold higher, respectively, following 14 days of exposure.
The terpenophenolic structure of CBD imparts lipophilic properties, allowing for passage across the blood–brain barrier.33,34 Many of CBDs reported therapeutic properties (e.g., anxiolytic and anticonvulsant effects) imply some level of brain activity. Brain distribution of CBD has previously been described in rats following CBD delivery through different routes; 9 cannabinoid levels peaked (5 min) and diminished rapidly after pulmonary (20 mg, 1 min) administration, while oral delivery (10 mg/kg CBD in sunflower oil) resulted in higher concentration, later peaks, and longer lasting CBD levels in brain. In the present study, we detected CBD at low levels in brain after higher dose 14-day inhalation (>3.5 mg/kg deposited dose) and after single oral administration of 10 mg/kg.
All CBD metabolites were measurable in brain tissue following the highest inhaled dose (180 min, 13.9/17.6 mg/kg CBD/PG deposited dose), albeit at much lower concentrations than CBD. Given these data, significant brain exposure, and in turn therapeutic neurological effects, may necessitate higher CBD inhalation doses. Notably, this study measured CBD and metabolites in brain tissue at a single time point (24 h) after final inhalation exposure. Exploration of earlier time points will more accurately determine the pharmacokinetic profile of CBD and metabolites in the brain.
CBD and its metabolites are excreted through urine and feces;2,19,20 only CBD was detectable in urine following 2 weeks of CBD inhalation (24 h postfinal dose). No analytes were detected after a single oral administration. In humans, higher urinary concentrations of CBD were achieved after oral versus pulmonary administration of 100 mg CBD (corresponding to <0.9 mg/kg CBD in rats), with a mean Cmax (Tmax) of 776 (5 h) and 261 (1 h) ng/mL, respectively. Urine CBD levels were below 10 ng/mL 24 h after dosing. 21 Further understanding of CBD excretion will necessitate investigation of additional time points and excretion routes.
While several rodent and human studies have reported sex differences in the pharmacokinetics of THC, few preclinical studies have explored CBD plasma concentration, metabolism, or excretion in males versus females. In humans, CBD plasma concentration is reported to be significantly higher in females following a single acute oral dose (25 mg CBD in MCT) with 2.4- and 1.5-fold higher AUC0–8h and AUC0–24h, respectively. 35 However, a second study reported no difference in CBD plasma levels in males versus females following a single inhaled dose (13.75 mg CBD only or 13.75 mg each CBD and THC), whereas females had significantly higher 7-COOH-CBD. 36 In the present study, inhalation did not result in any discernable differences in CBD, 7-COOH-CBD, or 6-OH-CBD Cmax or AUClast between sexes at the doses tested. However, female rats tended to have higher 7-OH-CBD Cmax and AUClast (0–2 h) than males following both acute and repeated CBD inhalation.
As a growing number of women are reporting medical cannabis use, 37 further delineation of sex differences in CBD pharmacokinetics at physiologically relevant doses is prudent.
In conclusion, the present study delineates differences in CBD pharmacokinetics as related to route and frequency of administration. This work is relevant to human use patterns, given the wide availability and increasing use of oral and inhaled CBD products, and the fact that many therapeutic applications of CBD relate to chronic conditions and necessitate repeated delivery. While both inhalation and ingestion are suitable routes of CBD administration, depending on desired onset or durability of effects, one route may be favored over the other.
Footnotes
Authors' Contributions
Dr. Schwotzer—conducted study (study director), and wrote the article.
Dr. Kulpa—wrote the article.
Dr. Trexler—wrote the article.
Mrs. Dye—ran statistics and pharmacokinetic analysis, and wrote the article.
Mr. Jantzi—ran bioanalytical sample analysis, and wrote the article.
Mr. Irshad—ran aerosol exposure, and wrote the article.
Dr. Ware—wrote the article.
Dr. Bonn-Miller—wrote the article.
Dr. McDonald—designed study, and wrote the article.
Mr. Lefever—designed study, and wrote the article.
Author Disclosure Statement
Authors J.K., K.T., M.W., M.B.-M., and T.L. are full-time employees of Canopy Growth Corporation, a producer and retailer of cannabis and hemp products. No competing financial interests exist for authors D.S., W.D., J.J., H.I., and J.M., as Lovelace Biomedical is a nonprofit research institution.
Funding Information
This work was funded by Canopy Growth Corporation.
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.