
Abstract
Background:
Cannabidiol (CBD), one of the major cannabinoids derived from the cannabis plant, is available over the counter. CBD is often used by patients for the management of insomnia, yet research supporting CBDs effectiveness as a treatment for insomnia is inadequate.
Objective:
The objective of this review was to critically evaluate the literature regarding the therapeutic benefits of CBD in the management of insomnia.
Methods:
A comprehensive search of the following databases from inception to December 29, 2021, was conducted: Ovid MEDLINE® and Epub Ahead of Print, In-Process & Other Non-Indexed Citations and Daily, Ovid Embase, Ovid Cochrane Central Register of Controlled Trials, Ovid Cochrane Database of Systematic Reviews, and Scopus. The search included randomized controlled trials, nonrandomized experimental studies, cross-sectional studies, cohort studies, case series, and case reports. Risk of bias was assessed with the Agency for Healthcare Research and Quality design-specific recommended criteria.
Results:
Thirty-four studies were eligible for inclusion. All studies reported improvement in the insomnia symptoms of at least a portion of their participants. Of the 34 studies, 19 studies used CBD predominant therapy and 21 studies used nearly equal ratios of CBD to Δ9-tetrahydrocannabinol (THC). Of the studies that performed hypothesis testing, 4 of 7 studies with a CBD predominant arm and 12 of 16 studies with a nearly equal ratio of CBD to THC arm reported significant improvement in insomnia outcomes. However, only 2 of the 34 studies focused on patients with insomnia, of which 1 study was a case report. Additionally, several studies used nonvalidated subjective measures, and most studies failed to include objective measures for symptom assessment.
Conclusions:
The results of our systematic review suggest that CBD alone or with equal quantities of THC may be beneficial in alleviating the symptoms of insomnia. Nevertheless, future research assessing CBDs effectiveness in population of patients specifically with insomnia utilizing validated subjective and objective measures is necessary before definitive inferences can be made.
Introduction
Insomnia, a sleep disorder characterized by poor sleep quality and quantity, affects more than 10% of the population. 1 To meet the diagnostic criteria for insomnia, an individual must report difficulty with sleep initiation and maintenance at least three times a week for 3 months or longer. 2 Insomnia significantly impacts physical and mental health, social functioning, and quality of life and frequently coexists with multiple medical and psychiatric disorders. 3 Common medical disorders comorbid with insomnia include chronic pulmonary disorders, hypertension, diabetes, cancer, chronic pain, heart failure, rheumatologic disorders (such as osteoarthritis and rheumatoid arthritis), and neurological disorders (such as Parkinson's and dementia).4–8 Comorbid psychiatric disorders include depression, anxiety, substance use disorders, and post-traumatic stress disorder (PTSD).9–12 In addition, insomnia is also frequently comorbid with other sleep disorders such as sleep apnea, limb movement disorders of sleep, and circadian sleep disorders. 13
Despite the pervasive negative effects of insomnia on health and quality of life, currently available management modalities for insomnia have several limitations. Cognitive behavioral therapy (CBT) is the recommended first-line management for insomnia. 14 Although CBT has clinically meaningful effect sizes, compliance to CBT remains a challenge. 15 Reasons for this include the patient's time commitment to engage in the CBT strategies and changes in behaviors to improve sleep (sleep hygiene), which is challenging for individuals who are already chronically sleep deprived. For patients who have suboptimal clinical responses with CBT, a limited number of medications have been approved for the management of insomnia and include eszopiclone, zaleplon, zolpidem, lemborexant, suvorexant, ramelteon, and low-dose doxepin. 16
While these medications can at least partially alleviate insomnia symptoms, they all share the risk for common side effects such as central nervous system depression (impaired alertness and motor coordination), abnormal thinking and behavior changes, complex sleep-related behaviors, and a risk of worsening depression. These side effects along with concerns regarding dependence to these medications impact patient willingness to consider pharmacotherapy. 15 Therefore, despite limited evidence of efficacy and safety, patients frequently resort to over-the-counter medications such as diphenhydramine, dietary supplements such as melatonin, and botanicals such as valerian, chamomile, kava, passion flower, hops, and cannabis.17,18
In the United States, the 2018 farm bill legalized the production of hemp and hemp-derived products as agricultural products, removing them from their prior designation of controlled substances. 19 This made cannabidiol (CBD) legally available over the counter across the United States. CBD is one of the cannabinoids derived from the cannabis plant, and it is one of two major cannabinoids in therapeutic use today, the other being Δ 9 -tetrahydrocannabinol (THC). 20 CBD differs from THC in its lack of psychoactive effects, making it less controversial for therapeutic use than THC. The increased availability of CBD over the counter has resulted in heightened marketing of CBD for a wide variety of symptoms, including pain, anxiety, cancer treatment side effects, and insomnia. The majority of these indications are, however, not supported by rigorous clinical studies.
Observational studies report that sleep difficulties are one of the primary reasons for cannabis/CBD use.21,22 However, research on CBDs effectiveness as a treatment for insomnia is scant and varying in results. 23 The majority of studies evaluating cannabinoids and sleep have focused on the effects of THC; very few studies have specifically examined CBD.24–26 For example, a recent systematic review by Kuhathasan et al 27 examining cannabinoids and sleep reported 13 studies on nabiximols (1:1 ratio of CBD to THC), but only 1 study that examined the effectiveness of CBD alone. Another systematic review on cannabinoids and sleep that included at least three studies with CBD reported improvements in several sleep outcomes but concluded that there was insufficient evidence for their use in clinical practice. 25 Although it appears that cannabinoids may be beneficial in the management of insomnia and sleep disorders, more research is needed to determine if CBD specifically is beneficial in the management of insomnia.
The aim of this systematic review was to evaluate the possible benefits of CBD in the management of insomnia. While past reviews on this topic have focused broadly on cannabinoids in the treatment of sleep disorders, this review specifically examines the effects of CBD on insomnia.
Methods
The protocol for this review was registered with the PROSPERO International Prospective Register of Systematic Reviews (ID: CRD42021257197). This review followed the 2020 Preferred Reporting Items for Systematic Review and Meta-Analyses (PRISMA) guidelines. 28
Search strategies
A comprehensive search of the following databases from inception to December 29, 2021, was conducted: Ovid MEDLINE® and Epub Ahead of Print, In-Process & Other Non-Indexed Citations and Daily, Ovid Embase, Ovid Cochrane Central Register of Controlled Trials, Ovid Cochrane Database of Systematic Reviews, and Scopus. One reviewer also searched the reference lists of previous reviews for relevant publications. The specific inclusion criteria were as follows: (1) human participants, (2) age 18 years or older, (3) written in English, (4) measured CBD use, and (5) at least some participants took CBD in an equal or higher concentration compared with other cannabinoids taken simultaneously by the individual. Studies of any design were eligible for inclusion. Review articles, conference proceedings, book chapters, and study protocols were excluded. The complete search strategy for each database can be found in Table 1.
Search Strategies for All Databases
Article screening and data extraction
Covidence systematic review software (Veritas Health Innovation, Melbourne, Australia) was utilized for the article screening process. Two reviewers independently screened each article against the eligibility criteria by abstract and title. Articles that met the eligibility criteria were then moved to the full-text screening stage and screened by two reviewers independently. Two reviewers then independently extracted data from all eligible articles. Disagreements at each step of the screening and data extraction process were settled via discussion with a third reviewer.
During data extraction, only measures pertaining to insomnia (subjective or objective difficulty in falling asleep, staying asleep, or early awakening; restful or refreshing sleep; sleep quality; sleep duration) or placebo were included. For these measures, data for each time point (means and standard deviations or medians and ranges) and intervention details were extracted. Specific data extracted included country in which the study was conducted, sample size, participant demographic information (sex, age, race, ethnicity, body mass index, comorbidities, experience with cannabis), primary and secondary outcomes, intervention characteristics (types of cannabinoids studied, dose route of administration, frequency, and type of cannabinoid strain or product), and funding sources.
Risk of bias assessment
Two reviewers independently assessed the risk of bias utilizing the Agency for Healthcare Research and Quality design-specific criteria. 29 The questions used to assess the risk of bias are included in Table 2. Disagreements were settled via discussion with a third reviewer.
Agency for Healthcare Research and Quality Design-Specific Recommended Criteria Questions and Types of Biases
AHRQ, Agency for Healthcare Research and Quality; Q, question.
Data synthesis
Data were synthesized via summary tables. Study author, year, sample demographic information, intervention/study description, and results of CBD-dominant/equal CBD:THC preparations on insomnia symptoms are reported. The results of all cannabinoid preparations compared with placebo or baseline for clinical trials are also summarized, along with the risk of bias results.
Results
Study identification, screening, and inclusion
Details of the identification, screening, and inclusion of studies are reported in Figure 1. Our primary search identified a total of 286 studies. After duplicates were removed, 209 studies remained for screening. Of the 209 studies, 47 were eligible for full-text review. Following the full-text review, 15 studies were eligible for inclusion. An additional 19 eligible studies were identified through citation searching, resulting in 34 studies22,30–62 eligible for inclusion in this systematic review.
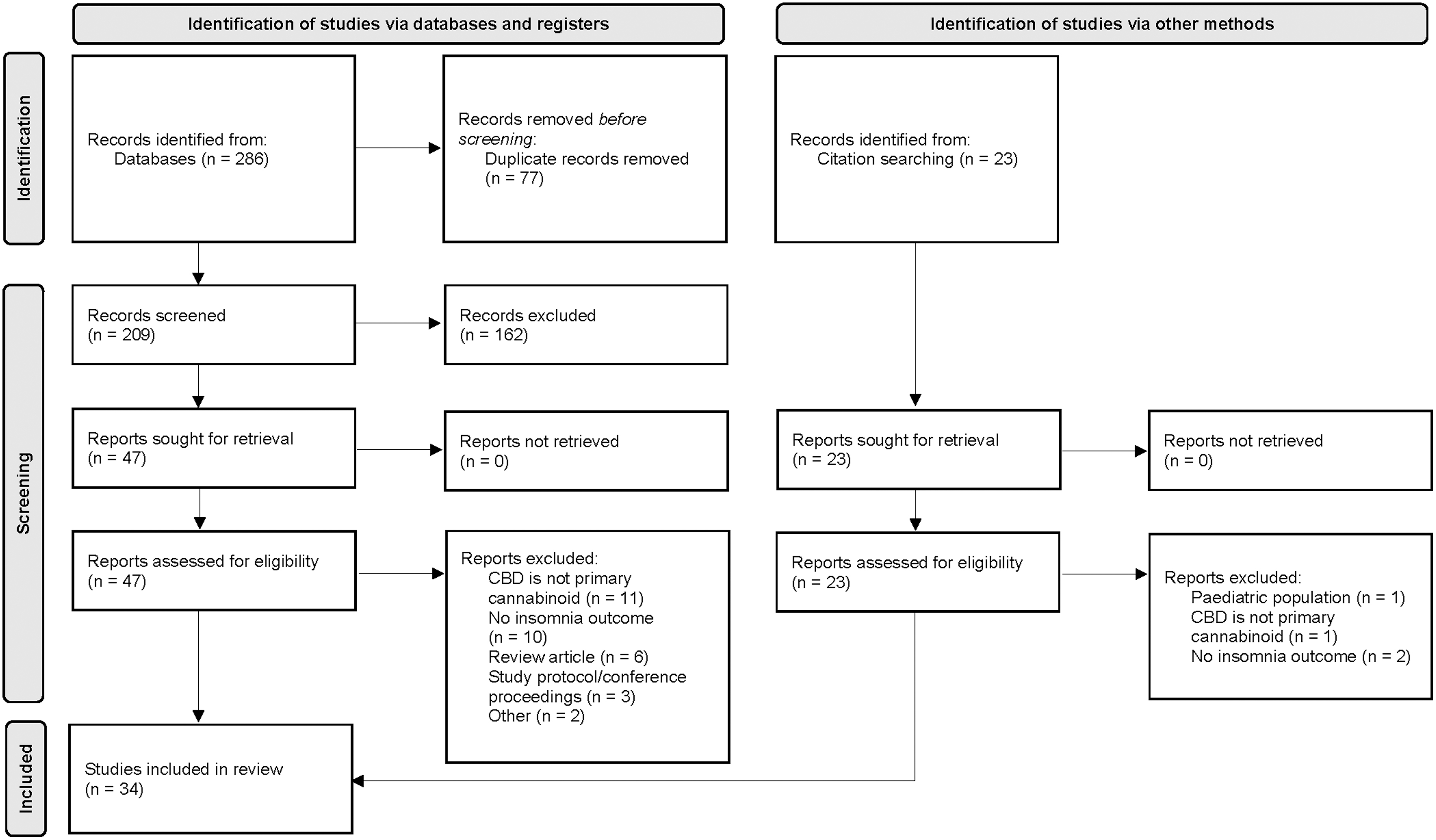
PRISMA flow diagram of identified, included, and excluded articles. PRISMA, Preferred Reporting Items for Systematic Review and Meta-Analyses.
Characteristics of included studies
Details of the included studies can be found in Table 3, and results of clinical trials are included in Table 4. Of the 34 studies included in this systematic review, 18 studies were clinical trials (randomized controlled trials [n=16]31,32,39,43,46,47,50–53,55–58,60,61 and nonrandomized experimental studies [n=2]34,42), 7 were cross-sectional studies,22,33,35,37,44,48,49 5 were cohort studies,36,38,41,45,62 3 were case series,40,54,59 and 1 was a case report 30 (Table 3). Only two studies30,45 (including one case report) focused specifically on patients with insomnia.
Details of the Included Studies Examining the Use of Cannabidiol for the Management of Insomnia Symptoms
Mean (SD) unless otherwise noted.
AIH, autoimmune hepatitis; CBD, cannabidiol; CI, confidence interval; EORCT QLQ-C30, European Organization for the Research and Treatment of Cancer Quality of Life Questionnaire; F, female; IQR, interquartile range; M, male; MS, multiple sclerosis; NRS, numerical rating scale; PCL-5, Post-traumatic Stress Disorder Checklist; PROMIS, Patient-Reported Outcomes Measurement Information System; PSQI, Pittsburgh Sleep Quality Index; PTSD, post-traumatic stress disorder; SD, standard deviation; THC, Δ 9 -tetrahydrocannabinol; VAS, visual analog scale.
Insomnia Outcome Results of All Cannabinoid Preparations in Clinical Trials
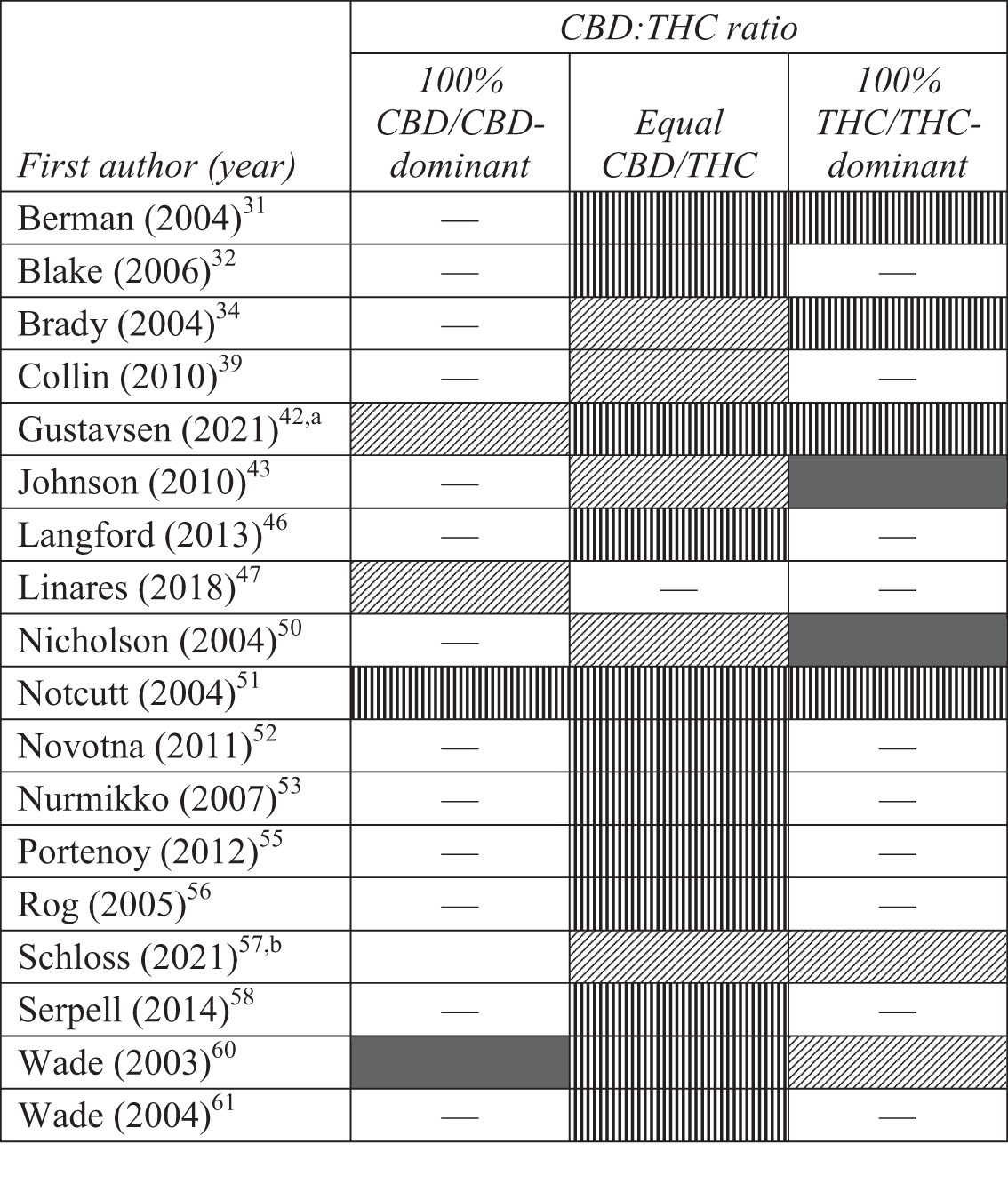
— Signifies no preparation in that category identified; vertical lines signify significant benefits in at least one insomnia outcome compared with placebo (or baseline if no placebo was included); diagonal lines signify benefits (although insignificant) in at least one insomnia outcome compared with placebo (or baseline if no placebo was included); solid fill signifies no benefits in any insomnia outcome compared with placebo (or baseline if no placebo was included).
All THC-containing products were analyzed for significance together.
No statistical comparisons by group were reported.
The remainder of the 32 studies evaluated insomnia symptoms in patients with cancer,43,55,57 multiple sclerosis and other neurological diagnoses,34,35,39,42,46,52,56,60,61 psychiatric disorders,40,59 chronic pain,36,37,51,53,58 autoimmune hepatitis, 49 brachial plexus injury, 31 rheumatoid arthritis, 32 fibromyalgia, 33 cannabis/CBD users,22,38,41,62 and healthy adults.44,47,50,54 Insomnia was the primary outcome in 10 studies30,32,35,45,47,49,50,54,59,62 and a secondary outcome for the remaining 24 studies. Other primary outcomes included pain,31,32,36–38,41,43,46,53,55,56,58,60,61 spasticity,39,52,60,61 mobility, 41 anxiety and other psychiatric disorders,30,38,40,41,54,62 fatigue/sleepiness,49,50 urinary tract symptoms,34,39 safety/tolerability of CBD/cannabis use,33,42,51 and reasons for CBD/cannabis use.22,33,44,48
Sleep measures and outcomes
Studies utilized a variety of sleep outcomes related to insomnia, including number of sleep disturbances per night,30,31,35,42,52,53,55,56 sleep quality,31,32,36,39,40,43,44,46,57–61 ability to fall asleep or stay asleep,22,35,47,50 and total sleep duration47,50,61 (Table 3). All but two studies47,50 used subjective self-report questionnaires such as numeric rating scales,31,32,35,38,39,42,43,46,52,55,56,58 Likert scales, 33 visual analog scales,34,60,61 purpose-developed survey questions,44,49 the Pittsburgh Sleep Quality Index,36,59 or specific questions within questionnaires such as the European Organization for the Research and Treatment of Cancer Quality of Life Questionnaire.35,40,43,57 Two studies47,50 utilized polysomnography to objectively measure CBDs impact on sleep outcomes. However, the participants in both studies were healthy adults with no preexisting insomnia symptoms.
CBD preparations and usage
Nineteen studies investigated the effects of CBD monotherapy/predominant therapy on insomnia symptoms (seven cross-sectional studies,22,33,35,37,44,48,49 four cohort studies,36,38,41,45 four clinical trials,42,47,51,60 three case series,40,54,59 and one case report 30 ) (Table 3). Twenty-one studies investigated the effects of products with nearly equal ratios of CBD to THC (17 clinical trials,31,32,34,39,42,43,46,50–53,55–58,60,61 2 cross-sectional studies,35,37 and 2 cohort studies38,62). CBD-containing products were administered through various routes, including oromucosal or sublingual sprays/drops,31,32,34,39–41,43,44,46,49–56,58,60,61 oral capsules/gelatine,40,44,47,49,59 inhalation,38,49 or topical application 49 with varying dose and frequency. For studies that reported the quantity of CBD used, doses ranged from 2.5 mg of CBD to 330 mg daily.
Effects of CBD on insomnia symptoms
All the 34 studies reported some level of improvement in the insomnia symptoms of at least a portion of their participants following the administration of CBD-containing products (Table 3). Of the 19 studies that investigated the effects of CBD monotherapy/predominant therapy on insomnia symptoms, 7 studies36,42,45,47,51,54,60 tested for significant versus insignificant improvement compared with baseline or placebo. Four of these studies reported statistically significant improvements in insomnia symptoms (two cohort studies,36,45 one case series, 54 and one clinical trial 51 ). Of the 21 studies that investigated the effects of products with nearly equal ratios of CBD to THC, 16 studies31,32,34,39,42,43,46,50–53,55,56,58,60,61 tested for significant versus insignificant improvement compared with baseline or placebo. Twelve of these studies reported statistically significant improvements in insomnia symptoms (12 clinical trials31,32,42,46,51–53,55,56,58,60,61).
Risk of bias
A similar number of studies had low versus high risk of bias (Table 5). Overall, 16 studies had a low risk of bias (15 clinical trials31,32,39,43,46,47,50,52,53,55–58,60,61 and 1 cross-sectional study 33 ), 4 studies had a moderate risk of bias (2 case series/case reports,30,59 1 cohort study, 45 and 1 clinical trial 51 ), and 14 studies had a high risk of bias (6 cross-sectional studies,22,35,37,44,48,49 4 cohort studies,36,38,41,62 2 case series/case reports,40,54 and 2 clinical trials34,42). Common problems among studies with cohort designs included not attempting to balance the allocation between the groups, not selecting an appropriate comparison group, and not having similar baseline characteristics between the groups.
Risk of Bias of Individual Studies Using the Agency for Healthcare Research and Quality Design-Specific Recommended Criteria
Articles with a score less than 60% of the highest possible score are designated as high risk of bias; articles with a score 60%–69.9% of the highest possible score are designated as moderate risk of bias; articles with a score greater than or equal to 70% of the highest possible score are designated as low risk of bias.
—Signifies that question is not relevant to the study design; 1 signifies desirable, low risk of bias answer to question; 0 signifies undesirable, high risk of bias answer to question (including “unsure”). Questions can be found in Table 2.
Additionally, only clinical trials addressed the impact from concurrent interventions or unintended exposure that might bias results. Thirteen studies22,30,35–38,40,41,44,48,54,59,62 did not assess confounding variables using valid and reliable measures. Seventeen studies22,30,34–38,40–42,44,48–50,54,59,62 did not have outcome assessors blinded to the intervention or exposure status of participants. Attrition was also a potential problem for 19 studies.32,34,36,38–43,45,47,51–53,55,57,60–62
Discussion
The results of this systematic review suggest that CBD, either alone or in combination with equal amounts of THC, may be beneficial in the management of comorbid insomnia in patients with cancer, multiple sclerosis, psychiatric disorders, chronic pain, and PTSD. However, because only two included studies focused on patients with insomnia (including one case report), these results cannot be generalized to patients with primary insomnia.
Our results are consistent with previous reviews examining the effects of CBD on sleep outcomes. For example, a systematic review by Khan et al 63 examined the therapeutic benefits of CBD in psychiatric disorders and reported that CBD may be beneficial in patients with insomnia related to seasonal affective disorder and PTSD. However, based on the level of evidence, the authors graded their recommendation for the use of CBD for insomnia as weak. The results of another systematic review that evaluated the use of THC alone or THC in combination with CBD for sleep outcomes in patients with multiple sclerosis, PTSD, and chronic pain also concurred with the results of our study. 27 However, the authors reported several shortcomings, including a dearth of studies in which sleep was the primary outcome and the use of nonvalidated questionnaires to measure sleep outcomes.
Although the initial goal of this review was to exclusively evaluate CBD (and not THC) for insomnia, it became clear following our literature searches that there were few clinical studies with CBD alone that included sleep as an outcome. Consequently, we elected to include all studies that had a treatment arm with CBD in equal or higher concentration compared with other cannabinoids. This decision resulted in the inclusion of studies with nabiximols (which have a nearly equal ratio of THC to CBD). In these studies, it is difficult to differentiate the specific effects of CBD versus THC, and nabiximols require further study.
For example, high doses of CBD have been shown to be sedative while also being nonintoxicating and having a low addiction risk. 64 THC, however, is psychoactive and with chronic use may decrease sleep latency, interfere with the circadian sleep–wake cycle, reduce somnolence (while increasing daytime sleepiness and delaying sleep onset the next night), and decrease slow-wave sleep.24,64,65 However, given that the 12 studies using nearly equal ratios of CBD to THC found significant improvements in insomnia outcomes, it is possible that CBD balances the effects of THC on sleep and the combination of the 2 cannabinoids may be synergistic for insomnia.
Study limitations
Our study had several limitations. First, only three clinical trials in this systematic review investigated CBD monotherapy/predominant therapy, and none of these three studies were conducted in patients with insomnia (one focused on healthy adults, one on patients with neurological diagnoses, and one on patients with chronic pain). Second, only 1 study 50 of the 34 studies reported being specifically powered to detect insomnia-related outcomes. Third, the majority of the studies lacked objective measures of insomnia, and several studies used nonvalidated instruments to measure insomnia symptoms. Fourth, there was a high degree of variability in outcomes and treatments. Finally, nearly half of our included studies had a high risk of bias.
Conclusions
Despite these limitations, the results of our systematic review suggest that CBD (alone or in combination with THC) may be helpful in managing insomnia symptoms. Additional studies examining the effects of CBD in patients with insomnia are needed, particularly studies that use validated subjective and objective measures to assess insomnia, before CBD can be strongly recommended in clinical practice.
Availability of Data and Material
The data supporting the conclusions of this article are available from the corresponding author upon request.
Footnotes
Acknowledgments
The authors would like to acknowledge Mayo Clinic Librarians Leslie Hassett, MLS, and Julie Taylor, MLS, for their valuable help in conducting literature searches for this systematic review.
Authors' Contributions
R.M.R., M.O.W., L.L.T., and A.V. were responsible for the conception and design of the work. R.M.R., M.O.W., and A.V. were responsible for the acquisition and interpretation of data. All authors were involved in drafting the article, critically revised it for intellectual content, and approved the final version of the article.
Author Disclosure Statement
No competing interests have been declared by the authors.
Funding Information
No funding was received for this systematic review.