
Abstract
Introduction:
As more states pass recreational cannabis laws (RCLs) for adults, there is concern that increasing (and state-sanctioned) cannabis acceptance will result in a reduced perception of risk of harm from cannabis among children. We aimed to discover whether children in states with RCLs had decreased perception of risk from cannabis compared with children in states with illicit cannabis.
Methods:
We analyzed data from the multisite multistate Adolescent Brain and Cognitive Development Study to determine how the perception of cannabis harm among children (age at baseline: 9–10; N=10,395) changes over time in states with and without RCLs. Using multilevel modeling, we assessed survey responses from children longitudinally across 3 years, adjusting for state-, family-, and participant-level clustering and child-level factors, including demographics (sex, race, and socioeconomic status), religiosity, and trait impulsivity.
Results:
There was no significant main effect of state RCLs on perceived risk of cannabis use, and no differences in change over time by state RCLs, even after controlling for demographic factors and other risk (e.g., impulsivity) and protective (e.g., religiosity) factors.
Conclusions:
This analysis indicates that state-level RCLs are not associated with differential perception of cannabis risk among children, even after controlling for demographics, trait impulsivity, and religiosity. Future studies could assess how perception of risk from cannabis changes as children and adolescents continue to mature in states with and without RCLs.
Introduction
In the decade since Washington and Colorado became the first states to legalize cannabis use for recreational purposes in 2012, 16 more states in the United States and the District of Columbia have passed recreational cannabis laws (RCLs) permitting use of recreational cannabis and creating commercial markets for cannabis products for adults over age 21, as of December 2021. One potential concern about legalization is that state sanctioning of recreational cannabis use will reduce perception of risk from cannabis use among children.
Low perceived risk of using cannabis, often assessed by asking children how much they believe using cannabis will harm or cause problems to themselves or to others, is strongly associated with substance use.1–3 Because many studies show that use of cannabis at earlier ages is associated with increased risk for depression, anxiety, schizophrenia, and substance use disorder, 4 it is important to understand factors associated with how children perceive (or fail to perceive) risk from cannabis use, to inform efforts to target early preventive interventions.
Because medical cannabis laws (MCLs) have a longer history in the United States than RCLs, with California passing the first MCL in 1996, many studies have assessed how passage of MCLs affected perception of risk from cannabis use among adolescents. The effect of MCLs on risk perception remains unclear. Whereas one study found that the enactment of MCLs was associated with a small increase in perceived harmfulness of cannabis among 8th grade students, 5 another found a reduction in perceived harmfulness among adolescents. 6
Studies have also examined cannabis use itself, rather than harm perceptions, following MCLs, also with inconsistent results, with one finding no statistical change in cannabis use among adolescents, 7 and another showing a decrease in cannabis use in 8th graders and no change among 10th and 12th graders after MCL implementation. 8 More recent studies investigating cannabis use prevalence, using 1999–2015 9 and 1997–2017 10 Youth Risk Behavior Surveys, found small reductions or no change in measures of cannabis use.
Fewer studies have examined how RCLs have affected cannabis use or perceived harm among adolescents, as these laws were more recently enacted. The largest study to date 11 assessed the association of RCLs with occasional and frequent cannabis use, as well as with cannabis use disorder (CUD) across age groups, using a multilevel approach before and after the legalization of recreational cannabis throughout the United States. Data from this study indicated that adolescents' reporting of CUD increased, and in those 26 years or older, both frequent cannabis use and CUD increased slightly, after RCLs were enacted, 11 suggesting that RCLs may slightly increase risk for problematic cannabis use patterns. However, this study did not use longitudinal modeling to track responses in the same participants over time, preventing inferences regarding change over time in states with RCLs.
A possible explanation for the conflicting results of the association between RCLs and cannabis risk perception is that most studies do not consider relevant child-level covariates that may explain some of the variation in cannabis risk perception. Certain groups of children with specific risk factors for substance use, such as high impulsivity, may be more likely than others to underweight the risk of cannabis in states with more permissive regulatory environments. Impulsivity, which is the tendency to act prematurely without foresight, is a well-known risk factor for most forms of drug-taking.12–16
High impulsivity often leads to behaviors that are maladaptive, including substance misuse, 17 with bidirectional relationships noted between impulsivity and cannabis use specifically. 18 Furthermore, not only is substance use behavior more likely in those who use substances, but also perception of risk from substances is lower in adolescents with higher impulsivity scores. 19 Similarly, most studies do not consider potential protective factors, such as religiosity, which may increase cannabis risk perception. Several studies indicate that higher degrees of religiosity, including religious attendance, involvement, and reliance on religious beliefs in decision-making, are associated with negative attitudes toward substance abuse. 20
As the Center for Disease Control has shown that biological, social, environmental, psychological, and genetic factors are associated with substance use, 21 we included a short list of demographic factors (sex, race, and income) to ask whether sociodemographic factors may also predict cannabis risk perception. Finally, perception of cannabis risk may decrease with age from childhood to adolescence and young adulthood, 22 and thus, analyzing longitudinal data in the same children over time may add important information to understanding how RCLs affect changes in cannabis risk perception over time.
In this study, we examined how the perception of cannabis risk differed among elementary- and middle-school aged children from states with and without RCLs. We assessed data from these children longitudinally across 3 years, using a multilevel model that accounted for state and participant-level clustering and adjusted for the relative contributions of child-level factors, including impulsivity, religiosity, and demographic factors. Our hypothesis was that children in states with RCLs would perceive cannabis as less risky compared with children in states with illicit cannabis, even after controlling for factors such as demographics, impulsivity, and religiosity. This research question is important for understanding the relative influence of state cannabis policy, as well as demographics, and child-level factors, on the perceived risk of cannabis in children as a growing number of states pass RCLs.
Methods
Participants
We used publicly available data from the Adolescent Brain and Cognitive Development (ABCD) Study (https://abcdstudy.org), a long-term population-based study of brain development and child health among 11,875 youth in the United States. Participants were enrolled at age 9–10 across 21 sites, including enrichment for siblings and twins. The ABCD Study obtained centralized institutional review board (IRB) approval from the University of California, San Diego. Each of the 21 sites also obtained local IRB approval. Parents or caregivers provided written informed consent, and children gave written assent. Details about recruitment and sample characteristics are reported elsewhere, as well as detailed full-text descriptions of survey items used. 23 Four waves of data: baseline and follow-up years 1, 2, and 3 were used in this analysis.
Measures
We selected the following measures from among the survey data collected.
Perceived risk of cannabis
Children were asked three questions assessing perceived risk of harm from cannabis: “How much do you think people risk harming themselves (physically or in other ways) if they use marijuana regularly?” (Question 1), “… if they try marijuana once or twice?” (Question 2), or “… if they use marijuana occasionally?” (Question 3). For each of these questions, possible response options were as follows: 0=No Risk; 1=Slight Risk; 2=Moderate Risk; and 3=Great Risk. In the current analysis, we summed the scores from these three questions, so the range of answers were from 0 to 9, with 0 being no risk, and 9 being greatest risk. These three questions were asked at follow-up years 1, 2, and 3, but were not asked at the baseline visit. We centered this variable in our analysis, so that we report observed changes in standard deviations.
State legal status
The children in the survey reside in 18 states. Because all states but one—South Carolina—had legal medical cannabis, we only examined variation in RCLs. Since questions about cannabis harm in this study were asked between 2016 and 2020, we created three categories of RCL status; states with RCLs before 2021 (RCL), states with RCLs passed in 2021, likely after the children were surveyed (Recent RCL), and states with illicit recreational cannabis (Illicit). In our data, five states (California, Colorado, Michigan, Oregon, and Vermont) passed RCLs before 2021, four states (Connecticut, Missouri, New York, and Virginia) passed RCLs in 2021, and the remaining eight states (Florida, Maryland, Minnesota, Oklahoma, Pennsylvania, South Carolina, Utah, and Wisconsin) did not have any RCLs by the end of 2021.
Impulsivity
The Urgency, Premeditation (lack of), Perseverance (lack of), Sensation Seeking, Positive Urgency, (UPPS-P) Impulsive Behavior Scale is a 59-item measure of five distinct facets of impulsivity. 24 Children completed this instrument at each of the four study waves. We used impulsivity at baseline in our model, and we centered this variable, to show how high or low impulsivity, relative to a centered mean, would affect perceived risk from cannabis.
Religiosity
The variable “religiosity” was measured using the parent response to the following question: “In general, how important are your child's religious and spiritual beliefs in his/her daily life?” Answers were “1=Not at all; 2=Not very; 3=Somewhat; 4=Very Much; and 999=Don't know.”
Other demographic data
For household income, we categorized children at one of three levels of income: low (household income <$50,000 per year), medium ($50,000–$100,000 per year) or high (>$100,000 per year). We also included a variable of self-reported race. The race categories in the survey were self-reported, and were categorized as Asian, Black, Mixed/Other, or White. Sex was male or female, and was self-reported.
Analysis
We used a multilevel model in which time is nested in children and children are nested in states. Because states have different RCLs that could potentially affect the average baseline risk perception across the state, we allowed each state to have its own intercept. We then allowed each child to have their own intercept, reflecting how risk perception may also be the result of child-level factors. We note that to account for siblings and twins in the data set (as there were 11,875 participants from 9983 families), we considered and ran a four-level model in which children were nested in families; however, that model did not affect significance of any variable. Thus, to balance nested data structure and model complexity we used the three-level models described as follows.
A likelihood ratio test confirmed that adding random slopes at the child level would improve model fit (p≤0.001) reflecting how change over time in risk perception can differ across children. An additional likelihood ratio test confirmed that allowing random slopes for states would also be a statistically significant improvement (p<0.001) reflecting how change in risk perception over time may also be different according to the RCL status of the state. We, therefore, allow for random intercepts and random slopes (by time) at both the child and state levels in all models. For all analyses, we used the lmer function in the lme4 package for R, version 3.51.
After developing an initial three-level model, we simplified and tested three models of increasing complexity in the combination of covariates. The final analytic model was selected based on Akaike Information Criterion (AIC) and Bayesian Information Criterion (BIC). Our models were as follows.
Model 1
Demographics-only model. Regresses the perceived risk of cannabis on time, sex, family income, and race (fixed effects), allowing for random slopes by time and random intercepts at both the child and state levels.
Model 2
Simple RCL model. Beginning with all covariates included in Model 1, this model adds covariates for child-level impulsivity, religiosity, RCL status, and the interaction of these.
Model 3
Complex RCL interactions model. Beginning with all covariates included in Model 2, this model adds interactions between RCL status and all other demographics: sex, religiosity, family income, and race. We also allow two key covariates, RCL status and impulsivity, to predict the grand slope (interacting these two terms with time). This model allowed us to test whether RCL status might impact different groups in different ways.
In our comparison of models, we selected Model 2 because it had the best AIC/BIC, indicating that it maintained simplicity while still allowing us to focus on the parameters of interest. The multilevel equation for our final model (Fig. 1) has the following form, with level 1 as time, level 2 as child, and level 3 as state-level: risktij is the perceived risk of cannabis at time t by child i in state j.
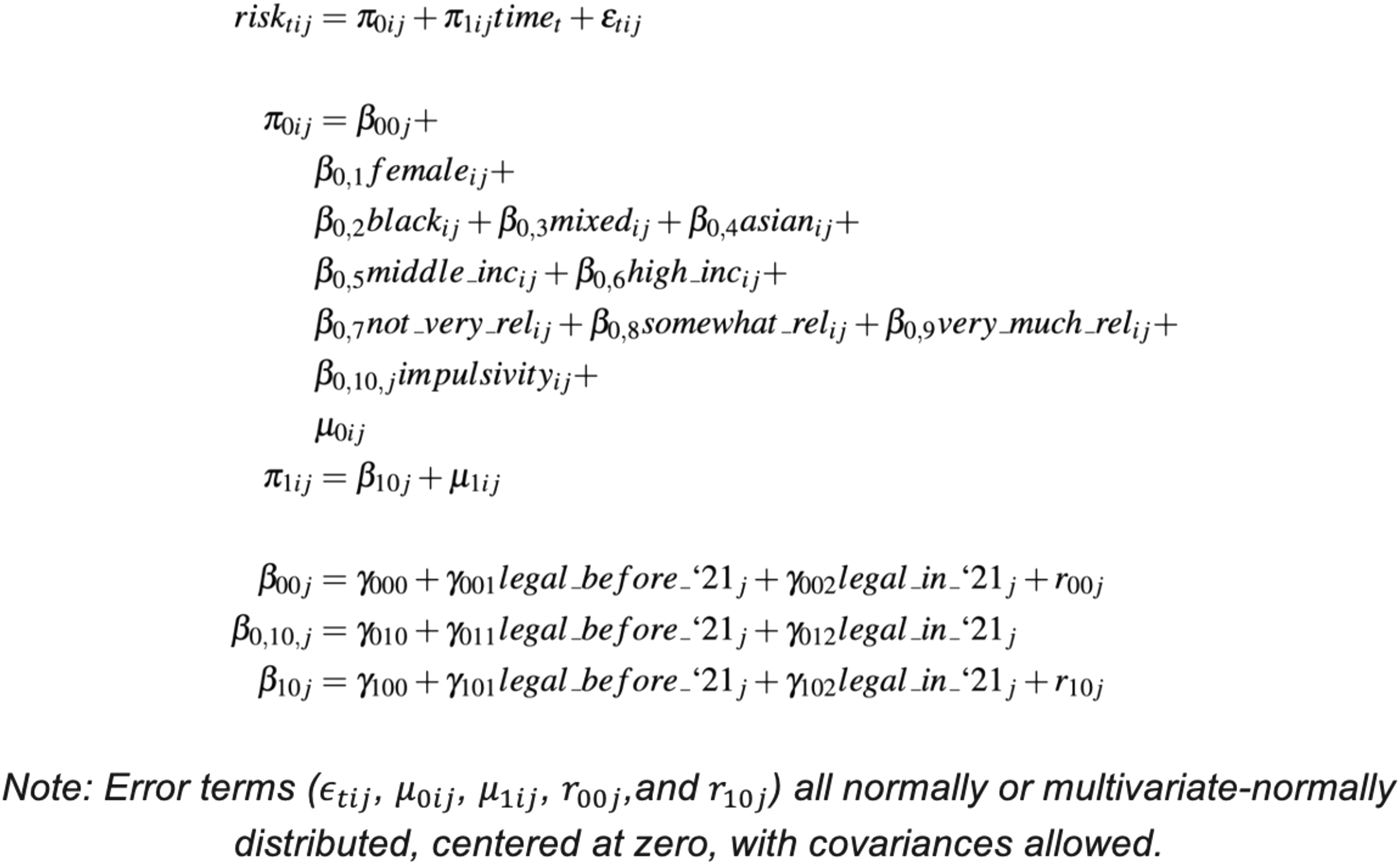
Three-level model equations for our preferred model specification: Model 2.
Results
After excluding those with missing data, we analyzed 10,395 children at baseline, 10,170 (98% of baseline sample) at follow-up year 1, 10,395 (100%) at follow-up year 2, and 6132 (59%) at follow-up year 3. See Table 1 for demographic information.
Demographics for Adolescent Brain and Cognitive Development Data
Please note: All states but SC have legalized cannabis for medical use. NY, VA, MO, and CT legalized cannabis for recreational use in 2021. The following states have legalized recreational cannabis use before 2021: CA (2016), CO (2012), OR (2015), MI (2018), and VT (2018). Cannabis remains illegal for recreational use in FL, OK, SC, FL, MD, MN, PA, UT, and WI. Biological sex assessed by self-report. Impulsivity assessed by self-report in the UPPS-P Scale. UPPS-P, Urgency, Premeditation (lack of), Perseverance (lack of), Sensation Seeking, Positive Urgency.
The child-level intraclass correlation coefficient (ICC) was 0.31, meaning that child-level variation over time accounted for 31% of the variance in risk perception of cannabis. The state-level ICC was 0.013, meaning that state-level variation accounted for 1.3% of the variance in risk perception of cannabis. Thus, most of the variation in reported perception of cannabis harm was due to children changing their response across time. Very little, if any, of the variation was explained by systematic differences between states. See Figure 2 for perceived risk of cannabis by state.
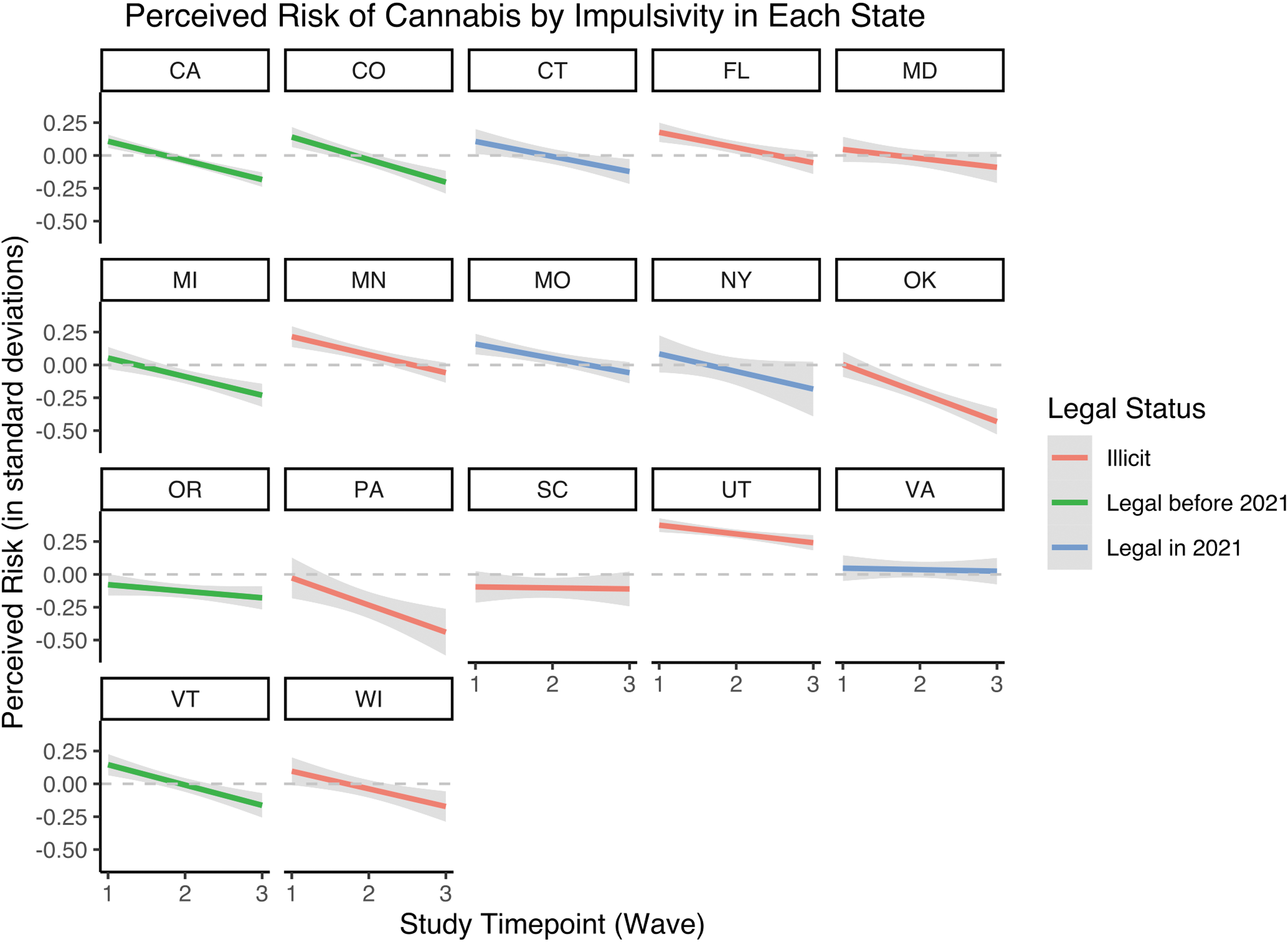
Perceived risk of cannabis at each study wave in each state.
We used effects coding for all categorical variables. Thus, the reference groups (coded as −1) were as follows: race=white, sex=male, income=low-income, religiosity=not at all religious, and RCL status=illicit. Because impulsivity was continuous, we used a z-score in the analyses. Therefore, the intercept can be interpreted as the grand mean, and coefficients can be interpreted as deviations from the grand mean (Table 2).
Models Showing Factors Associated with Perception of Cannabis Risk Among Children
p<0.001; **p<0.01; *p<0.05
For each variable, the coefficient is listed to the right of the variable, and the standard error is below the coefficient. Results in the text are based on Model 2, as it showed the lowest AIC and BIC. AIC, Akaike Information Criterion; BIC, Bayesian Information Criterion.
There was no main effect of RCL status, either recent or before 2021, on perception of cannabis risk, even after controlling for sex, race, family income, impulsivity, and religiosity (Fig. 3 and Table 2). As seen in Figure 3, there was a significant main effect of time (study visit), as children's perception of cannabis risk decreased by about 0.13 standard deviations from Waves 1 to 3, but the lack of a significant interaction between RCL and time indicates that the rates of change of cannabis riskiness over time did not differ by RCL status. We note that there was a small effect of RCLs enacted before 2021, with children rating cannabis as slightly less risky (Fig. 3); however, the effect was nonsignificant at only 0.04 standard deviation difference in risk perception between states with RCLs before 2021 versus states with illicit cannabis.
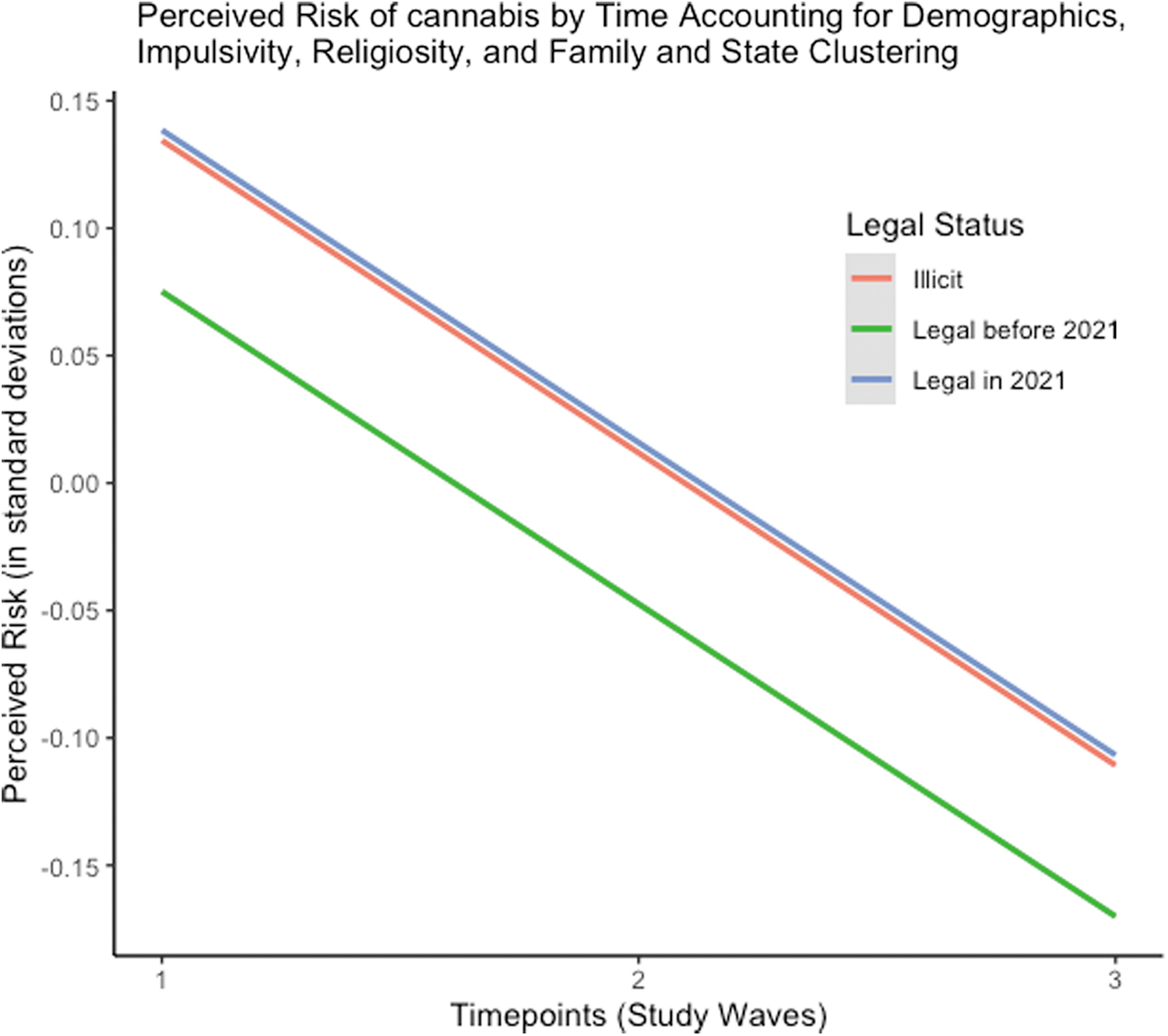
Perception of harm of cannabis over time in states with different recreational cannabis law status, controlling for demographics, time, and clustering.
Compared with the reference group “not at all religious,” self-identifying as very religious was associated with a 0.14 standard deviation higher rating in the perceived riskiness of cannabis (p<0.001) and identifying as not very religious was associated with a 0.05 standard deviation lower rating (p<0.001). Compared with the reference group “white,” self-identifying as Asian was associated with a 0.14 standard deviation higher rating (p<0.01), and self-identifying as Black was associated with a 0.19 standard deviation lower rating (p<0.001). Compared with the reference “low-income” group, high family income was associated with a 0.08 standard deviations higher rating in the perceived risk of cannabis (p<0.001). Impulsivity was associated with lower perceived riskiness of cannabis; a one standard deviation increase in impulsivity was associated with a 0.10 standard deviation decrease in perceived riskiness (p<0.001). These results suggest that factors other than state RCLs can be important indicators of perceived cannabis risk.
Discussion
In this analysis, we examined whether state RCLs were associated with perceived risks of cannabis, when covarying for child-level factors such as demographics, and two well-known risk and protective factors associated with cannabis risk perception, impulsivity, and religiosity. Consistent with the literature on other substances, we found that more impulsive children perceived less harm from cannabis throughout the three waves of the study,12–15 and that greater religiosity was associated with greater perception of risk from cannabis, 20 but there was no main effect of RCLs on perception of harm from cannabis.
We also replicated the finding that perception of cannabis risk decreased as children aged, which likely reflects an effect of age as well as an effect of time, as perceived risk of cannabis use has declined significantly in the United States since 2002. 22 We did not detect any significant interaction between time (i.e., study visits) and our variables of interest, indicating that the effect of decreased risk perception over time was not different among children living in states with different RCL status.
Although RCL status was not associated with risk perception, the variables of impulsivity, religiosity, household income, and race were significant in our models. Impulsivity and religiosity are well-known risk and protective factors for perception of risk of substance use, and this study provides further evidence of this. Household income and race are important components of social determinants of health (e.g., education, employment, neighborhood characteristics, and other experiences related to social phenomena) that are associated with health behaviors and disparities. We note that race is a social construct associated with health disparities due to historical and ongoing structural racism, and as such, the relationship between race and cannabis risk perception is not causal and likely reflects these systemic factors.
One of the strengths of this study is the use of multilevel modeling techniques in the analysis. We test the hypothesis that the perception of cannabis risk might be influenced not only by cannabis policy, but also by other factors that may vary from state to state (such as values or political views). However, we found that states only accounted for 1.4% of variance in risk perception of cannabis, despite a wide range of state-level policies. Future studies could perhaps examine whether more local neighborhood characteristics may be more predictive of attitudes toward cannabis than the state at a whole.
A limitation of our analysis is that only three time points were collected, with significant attrition at follow-up year 3. Additional waves of data from the ABCD cohort will also allow for more complex models of change (e.g., nonlinear growth curves). A second limitation is that the outcome of “perceived risk” is compiled by questions that ask about other people's potential harm from substances. The children surveyed were 9–12 years old, and there was not significant cannabis consumption yet in this population (although this is also a strength of the analysis, as children's perception of cannabis risk before use is less likely to be confounded by their own use history).
In this sample <1% of children had ever tried cannabis. As cannabis use increases among the sample, our models can be adapted to include cannabis use as the outcome. Finally, to simplify complex models, we chose to control for only a small set of factors; a risk factor (impulsivity) and a protective factor (religiosity), which have both been shown to predict risk perception of substances, and demographic factors. However, there is a much larger list of variables, such as psychiatric/mental health variables, or any experiences that the participants had with people around them using cannabis, which could have been considered when assessing whether RCL status affects risk perception of cannabis.
Discovering factors that predict risk perception of cannabis, however, was not the goal of this analysis, which aimed to discover whether RCL status affected risk perception over time. Future analysis can examine factors such as psychiatric/mental health variables and other behavioral measures (peer substance use, sports team membership, parent substance use, etc.), to predict the factors that determine cannabis risk perception.
Despite these limitations, this analysis shows that state RCLs alone do not play a significant role is perception of cannabis risk in children. This could have important implications for prevention and for policy, as this report shows that individual child-level characteristics, rather than state policy, contribute to attitudes toward risk of cannabis.
Footnotes
Data Sharing Statement
The ABCD dataset is publicly available. All code used in the analyses can be provided by Jodi Gilman and Massachusetts General Hospital. Requests for all materials should be submitted to Jodi Gilman.
Authors' Contributions
J.M.G., J.L.R., and A.E.E. contributed to concept for the analysis. J.M.G., M.I., E.G.P., E.M.K., K.P., and B.T.C. contributed to the analysis and interpretation of the data. J.M.G., M.I., E.G.P., and E.M.K. drafted the article. B.T.C., J.L.R., and A.E.E. contributed to the critical revision of the article for important intellectual content.
Author Disclosure Statement
A.E.E. has served as a consultant to Charles River Analytics (NIDA SBIR grant) and Karuna Pharmaceuticals (Chair Data Monitoring Board). Other investigators report no potential conflicts.
Funding Information
This study was funded by K02DA052684-01A1; PI: J.M.G. and K24DA303444; PI A.E.E. The funder had no role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; preparation, review, or approval of the article; and decision to submit the article for publication.