
Abstract
Background:
The prevalence of Substance Use Disorder (SUD) is increasing along with the need to develop approaches to reduce the harm associated with substance use, including investigating alternatives such as cannabinoids, which show promising results, although the current evidence is limited. This scoping review focuses on the limitations and potentials of cannabinoid-based treatments for SUDs.
Methods:
We examined between-subject randomized controlled trials (RCTs) investigating the use of CBD and THC as pharmacological treatment for SUDs in adults, with the procedures attending the expectations of the Preferred Reporting Items for Scoping reviews and Meta-Analyses (PRISMA) for Scoping Reviews guidelines and assessed risk of bias using the Cochrane Risk of Bias Assessment Tool 2.
Results:
Ten RCTs were included, with six demonstrating low risk of bias, and positive results were found for treating Cannabis Use Disorder, while contradictory results were found for Opioid Use Disorder, and inconclusive results for treating Cocaine Use Disorder.
Conclusions:
CBD and THC demonstrate potential for treating some SUDs, but evidence is limited. Robust RCTs with larger samples and longer follow-up periods are necessary to assess carefully developed outcomes for different SUD patients. New cannabinoid-based medications and scientific-based policies may advance SUD treatment. A comprehensive approach to treatment and careful methodological choices may benefit patients with SUD.
Background
Substance Use Disorder (SUD), according to the DSM-5, is classified as a primary mental health disorder characterized by a persistent pattern of substance consumption that causes significant harm. The diagnostic criteria include increased tolerance, withdrawal symptoms, maintained use despite negative consequences, and the presence of craving. 1 The prevalence of SUD is escalating, resulting in increased overdose-related deaths and disproportionate rates of contact with infectious diseases associated with unsafe practices of substance consumption.2–4
Such important impacts have highlighted the need for increasing access to treatment and developing more comprehensive and evidence-based approaches to reduce the harm associated with substance use.5,6 This includes the investigation of alternative medications that might avoid the well-known limitations of traditional medications for SUD, including limited effectiveness, unwanted side effects, risk of harmful use, and restricted access or affordability.7,8
Experimental studies suggest the safety and feasibility of cannabinoid-based medications like CBD and THC preparations (i.e., nabiximols, dronabinol, purified CBD) in treating SUD, often combined with first-line treatment medication and, in some cases, medical cannabis, showing generally positive results. Recent reviews indicate limited evidence,9,10 however, investigations on the potential of cannabinoids for treating SUD are progressively increasing as the endocannabinoid system's role in modulating the response to SUD-related behaviors is demonstrated. 11
The current clinical evidence on the effectiveness of cannabinoid-based treatments for SUDs is promising, but also has important limitations. For instance, one of the most recent meta-analysis showed that cannabinoid-based treatments present beneficial effects for the treatment of SUDs, but effect sizes were small to moderate, and the analysis of results was limited. 12 There is also a majority of within-subject over between-subject randomized controlled trials (RCTs) of cannabinoid-based medications for treating SUDs.9,12
While within-subject RCTs have contributed to our understanding of the effects of cannabinoid-based treatments for SUDs, between-subject RCTs offer advantages such as isolating the effects of the intervention, avoiding carry-over effects, and allowing for straightforward data analysis.13,14 Additionally, recent SUD between-subject RCTs have addressed many of the limitations observed in previous within-subject experiments. 15
We conducted a thematic narrative scoping review to evaluate the effectiveness of cannabinoid-based treatments for SUDs. Our approach allowed for a nuanced understanding of the results, considering the context in which studies were conducted and the methodologies' limitations. By presenting the results in a narrative format, we identified key themes and limitations of the existing literature. Our focus was on RCTs studying cannabinoid-based medications for treating adults with SUDs, aiming to provide guidance for future research efforts.
Methods
This scoping review adhered to the expectations of the Preferred Reporting Items for Scoping reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR) Checklist. 16 The complete PRISMA-ScR Checklist is available in the Item 1 of the Supplementary Material. The research protocol has been registered at PROSPERO (CRD42021245610) and had its last update on March 19, 2023.
Both researchers performed Boolean and conventional searching of reports retrieved from PubMed and PubMed Central, Research Gate, Google Scholar, and article reference lists from recent reviews on this topic.9,12,15,17 The Boolean search strategy is available in the Item 2 of the Supplementary Material. The last updated search was conducted across all employed sources on February 1st, 2023.
Eligibility criteria
We included English language between-subjects RCTs examining cannabinoid-based medications as primary treatment for adults diagnosed with or exhibiting patterns of SUDs. Additionally, studies that explored adjunct interventions, such as other medications or psychosocial treatments, were included. We excluded studies that investigated medical or adult cannabis as a primary intervention or had different outcomes other than treatment.
Peer-reviewed RCTs were selected after an initial search to remove duplicates. The primary author screened the abstracts and full-text versions, and the selection was confirmed by all authors to be between-subject RCTs evaluating cannabinoid-based medications' effects on SUD treatment outcomes. These outcomes included decreasing substance use, withdrawal symptoms, sustained abstinence, and improvement in physical and mental health and social function, as measured in validated instruments.
We selected 10 RCTs that examined the use of THC and/or CBD as a treatment for SUDs, including Cannabis Use Disorder (CUD), Opioid Use Disorder (OUD), and Cocaine Use Disorder (CoUD). The Preferred Reporting Items for Scoping reviews and Meta-Analyses (PRISMA) 2020 Flow chart 18 is provided in Figure 1.
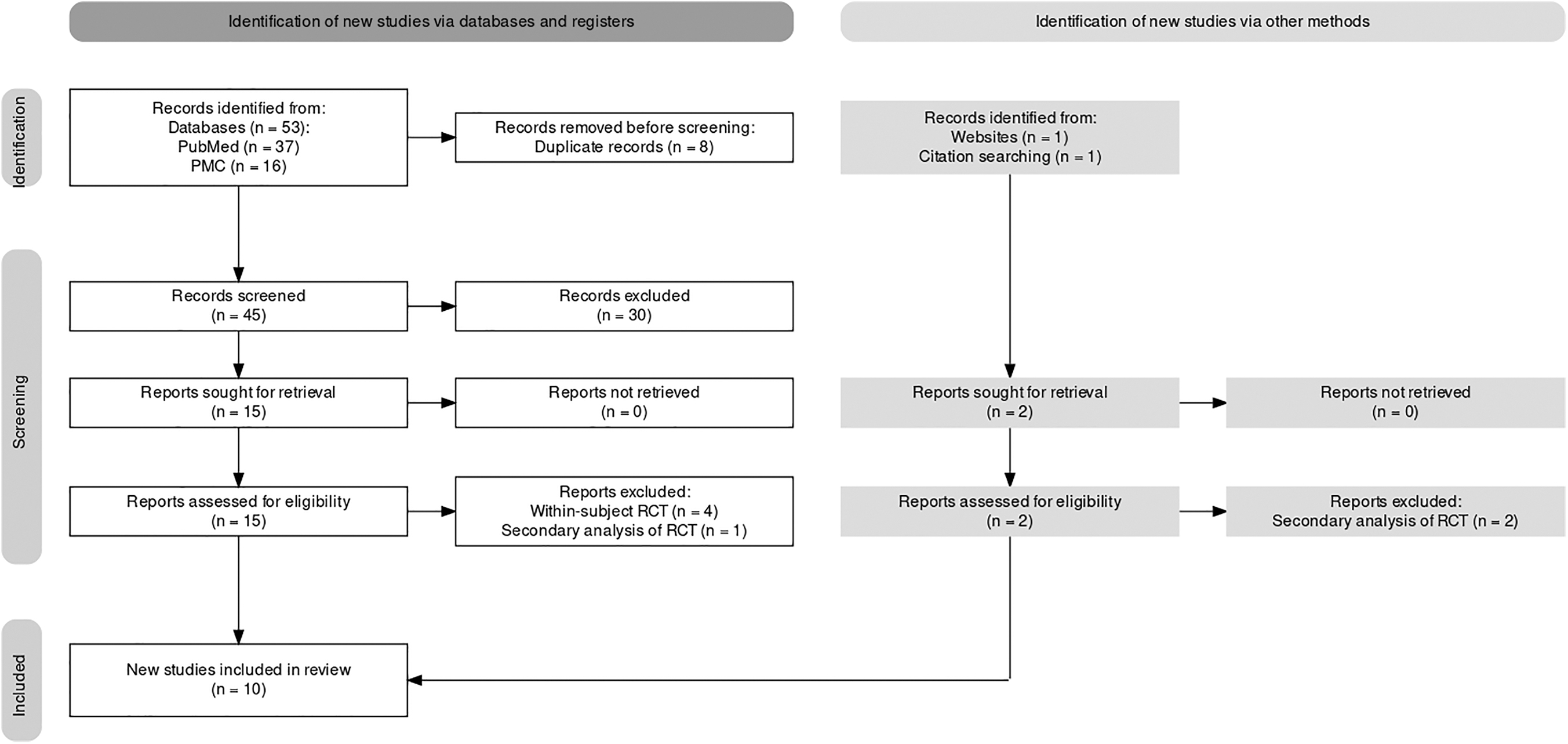
PRISMA 2020 flowchart. PRISMA, Preferred Reporting Items for Scoping reviews and Meta-Analyses.
Despite the promising evidence on the use of cannabinoid-based medications for the treatment of Tobacco Use Disorder,19,20 our search did not yield between-subjects RCTs with treatment endpoints. Additionally, consistent with the latest SUD literature, our scoping review did not identify RCTs of Alcohol Use Disorder, as the available evidence appears to be restricted to observational designs, as of this moment.15,17,21
Quality and bias assessment
As this scoping review included only between-subject RCTs, both the primary and coauthor conducted the quality and bias assessment using the Cochrane Risk of Bias Assessment Tool 2 (RoB 2). The RoB 2 assesses the risk of bias in RCTs across five domains and an overall risk of bias domain. Users of RoB 2 are asked questions in each domain to determine if there is low, moderate, or high risk of bias to identify potential sources of bias that could lead to inaccurate conclusions in trial design, conduct, and reporting. 22
Data extraction
The primary author assessed the full text of each RCT for data extraction. The data-charting process produced different tables based on the type of SUD assessed in the study and their publication date. Information was extracted regarding the participants' characteristics, treatment allocation, the main end-points of interest of each study, outcomes observed in the treatment and placebo group, and whether the treatment was effective. The results of each RCT were thematically categorized based on the type of SUD and were narratively described and analyzed according to their publication date, outcomes, and limitations. The coauthor and the principal investigator oversaw data extraction.
Results
A total of 55 studies were identified through a Boolean search on PubMed and imported for screening. Ten RCTs were thoroughly examined by both authors and approved for inclusion in the review by the principal investigator.
The 10 included studies had a median sample size of 55.5 subjects (range: 31–156) and were published between 2011 and 2021. Six studies investigated THC, CBD, or both for treating CUD. These studies were conducted in the United States (2),23,24 Australia (2),25,26 the United Kingdom (1), 27 and Canada (1). 28 Additionally, two studies from the U.S. examined the use of THC or CBD for the treatment of OUD,29,30 and two studies, one from Canada 31 and one from Brazil, 32 investigated the use of CBD for the treatment of CoUD. A total of 757 treatment-seeking participants were examined across these studies. The main or secondary outcomes assessed withdrawal severity, retention in treatment, days of substance use, abstinence, and mental health symptoms.
The RoB 2 results show that of the 10 RCTs, 6 demonstrated an overall low risk of bias,23,25,28,30,31,27 3 had some concerns regarding the randomization process, handling of the missing data, deviations from the procedure and outcome assessment,24,26,29 and 1 presented a high risk of bias due to unclear blinding procedures, possible deviations from the intervention and outcome assessment 32 (Table 1).
Cochrane Risk of Bias Assessment Tool 2
+Low risk of bias.
−High risk of bias.
? Some concerns.
Four of the six studies found positive results in the use of cannabinoids as a therapeutic intervention for CUD.23,25–27 CUD studies utilized different cannabinoid compositions, including nabiximols (CBD+THC),25,26,28 dronabinol (THC),23,24 and isolated CBD. 27 All were experiments for reducing cannabis use and achieving abstinence (Table 2).
Cannabis Use Disorder Studies
Lintzeris et al. (2020).
✗ Favors placebo.
✓ Favors medication.
↓ Decrease.
↑ Increase.
The two OUD RCTs found in this scoping review examined participants using heroin. Both studies are from the east coast of the U.S. and have different study designs with contradictory results. The first study investigated the potential of THC (dronabinol) in decreasing withdrawal and increasing time to relapse after an inpatient withdrawal period and found no differences compared with placebo. 29 The second one tested the effectiveness of CBD in preventing participants from relapsing after a drug-cue experiment and found significant reductions in withdrawal severity and anxiety scores compared with the placebo 30 (Table 3).
Opioid Use Disorder Studies
✗ Favors placebo.
✓ Favors medication.
↓ Decrease.
↑ Increase.
Finally, two RCTs have investigated the use of CBD as a treatment for CoUD.31,32 One study was a relapse-prevention trial with people who had used cocaine at least 2 weeks before enrolling in a drug-cue experiment, 31 and the other examined the retention of participants in an inpatient SUD treatment facility. 32 Both studies were inconclusive (Table 4).
Cocaine Use Disorder Studies
✗ Favors placebo.
CUD studies
The earliest parallel-group RCT identified in our research was conducted by Levin et al. 23 This 12-week outpatient trial found that THC significantly reduced withdrawal symptoms, but not the number of days of cannabis use among participants who frequently used cannabis. Additionally, THC significantly promoted retention in treatment, but abstinence was not reached. A similar finding was noted by Allsop et al., 25 which did not consider abstinence rates as an endpoint of interest but observed significant reductions in withdrawal symptoms in a 6-day inpatient trial of CBD+THC. However, participants returned to their regular pattern of use after 30 days.
Levin et al. 24 found no effects on withdrawal and abstinence rates when combining THC with lofexidine in a 10-week outpatient trial. Even though an early exploratory study by Haney et al. 33 had previously observed the effectiveness of combining THC and lofexidine for cannabis withdrawal symptoms, Levin et al. 24 pointed out that the lofexidine dose was not tolerated, which may have resulted in outcome assessment bias and the high dropout rate, thus contributing for inconclusive results.
Later, a crossover trial found decreasing withdrawal symptoms among participants who received CBD+THC. 34 However, a subsequent 12-week outpatient RCT by Trigo et al. 28 did not find differences in abstinence rates, days of use, and withdrawal symptoms. Subanalyses showed a trend for better outcomes with nabiximols compared with placebo when the medication was taken in higher doses. 28
After a 12-week trial of CBD+THC combined with CBT counseling and medical case management in the RCT by Lintzeris et al., 26 participants reduced their frequency of cannabis consumption and maintained it during the 3-month follow-up but did not achieve abstinence. 35 Differently from Trigo et al., 28 higher doses of medication were associated with lower odds of staying in treatment, but those who engaged during the follow-up period achieved significant rates of abstinence and reductions in cannabis-related problems and depressive symptoms. 35 Increased adherence to both psychosocial and pharmacotherapy treatment was associated with improved, longer-term outcomes and improved general health markers, suggesting that combining both techniques may ensure better results for treatment-seeking CUD patients. 36
The latest CUD study was conducted by Freeman et al. 27 and was the first RCT to explore oral CBD's potential to treat CUD symptoms, with a 4-week outpatient phase and a 24-week follow-up assessment. Participants received motivational interviewing sessions and significantly reduced cannabis use, achieving small but significant abstinence effects. The study had a 96% adherence rate, the highest in this scoping review.
CBD was more effective than placebo at reducing cannabis use and achieving abstinence. Participants also had reduced withdrawal and anxiety symptoms, consistent with previous studies showing CBD's effectiveness in reducing cannabis withdrawal symptoms during abstinence.37,38 This RCT included patients with CUD who reported co-use of cannabis cigarettes with tobacco and regular tobacco cigarettes, and found that while CBD reduced the number of tobacco cigarettes consumed, it did not address the co-use of cannabis and tobacco. 27 Notably, most trials do not investigate how tobacco use may influence the direction of their outcomes. 39 The combined use of cannabis with tobacco is a prevalent form of cannabis consumption in many regions, leading to more significant health burdens and difficulties in assessing the effects of cannabis consumption. Hence, these findings hold significant implications for the SUD literature.19,20,40
OUD studies
In the study by Bisaga et al., 29 participants using opioids were admitted to an inpatient unit for opioid withdrawal and induction into XR-naltrexone, followed by outpatient treatment with weekly therapy sessions and additional contingency management sessions with a psychiatrist. The RCT investigated whether using THC would reduce withdrawal symptoms during initial naltrexone treatment. The use of different medications in this standardized procedure may have influenced the outcomes. All participants provided urine samples to monitor substance use. 29
No differences between the THC and placebo groups regarding withdrawal symptoms and retention rates were found. As early studies were concerned with the safety of THC, participants had experience with smoking cannabis as an attempt to avoid unexpected effects. Cannabis smoking was reported by two-thirds of the participants and was associated with a reduction in withdrawal symptoms and improved retention in the outpatient phase and was associated with lower scores of depression and insomnia. This is aligned with a recent review, which observed that cannabis does not produce negative impacts on OUD treatment outcomes, 41 and with several observational studies, which suggest that cannabis use may substitute or mitigate the use of opioids, although further evidence is still needed to draw conclusions.42–44
After 4 years of the first OUD RCT publication, Hurd et al. 30 evaluated the effectiveness of CBD in promoting sustained abstinence and preventing relapse among individuals with OUD who have abstained from using heroin in a 10-day outpatient program with cue-induced craving sessions on days 1 and 2. Participants were given a 3-day regimen of either CBD or placebo, followed by a 1-week follow-up period. The final cue-induced craving session occurred on day 4. Participants provided urine samples each visit to monitor CBD and opioid use. 30
The results of this RCT indicated that cue-induced craving sessions were effective in eliciting craving and that both doses of CBD had a similar significant effect of decreasing cue-induced craving, with a medium-to-high effect size (Cohen's d=0.79), despite the small sample size (n=42). Additionally, both doses effectively reduced anxiety scores and that such significant effects were maintained during the follow-up assessment after participants received CBD. 30 These are consistent with the results of a previous pilot study by the research team, providing further support for the potential therapeutic benefits of CBD for OUD patients. 45
Furthermore, CBD did not affect heart rate, temperature, or blood pressure but did significantly impact salivary cortisol levels, suggesting that CBD prevented cortisol levels from increasing during the cue sessions. No effects were found on affect and cognition scores. Participants abstained from 1 to 3 months before the study and did not receive medical or psychological treatment. Instead, they were oriented to perform relaxation exercises after the cue sessions and received guidance to seek treatment. Three participants relapsed after the study. 30
CoUD studies
In the RCT Mongeau-Pérusse et al., 31 participants reported cocaine use at least 2 weeks before admission. The objective was to assess the effectiveness of CBD in reducing cue-triggered cravings, extending the time until relapse, and diminishing stress-stimulated cravings and cocaine consumption. The study was conducted in two phases: a 10-day inpatient and a 12-week outpatient follow-up. In addition, weekly psychosocial group sessions and medical check-ups every 4 weeks were conducted to ensure participant safety and monitor progress. On day 8, they underwent the cue session experiments. Participants provided weekly urine and blood samples to monitor cocaine and CBD use. No significant differences were found between the CBD and placebo groups regarding time to relapse and sustained abstinence duration.
The second RCT of CoUD in this scoping review was conducted by de Meneses-Gaya et al. 32 and examined the effectiveness of CBD in decreasing cocaine craving. Participants seeking treatment at an inpatient clinical facility were evaluated for inclusion in the study during the initial days of their hospitalization. Those who met criteria underwent a 10-day treatment utilizing CBD. They performed a cue-induced craving assessment and self-reported their cocaine craving daily. Additionally, they were offered a weekly group psychotherapy session as a standard psychosocial intervention provided by the institution. The study was based on self-reported data and did not gather substance use data as patients were hospitalized, and using substances would result in the termination of treatment.
The study showed a low dropout rate of 19.4% but no significant effects of CBD on reducing cocaine craving, despite showing good tolerability. Both groups showed similar decreases in depression and anxiety symptoms, suggesting the clinical treatment was effective. 32 This aligns with the findings of the RCT by Mongeau-Pérusse et al., 31 which also showed no significant impact of CBD on reducing cocaine cue-triggered cravings. However, these findings contradict previous studies that found CBD could reduce anxiety and depression.46,47
Discussion
CUD studies
Most CUD studies presented high dropout rates. As a strategy to increase adherence in CUD studies, abstinence has been recently suggested as a secondary rather than primary endpoint for CUD, such as decreased consumption associated with reduced related problems and increased general and mental health markers.48,49 Recommendations have emphasized the need to focus on developing other, more reliable and meaningful endpoints of treatment, including decrease in CUD severity, the time until treatment response is observed, and the number of patients who still meet CUD criteria at the end of treatment, instead of just measuring exposure to cannabis.49,50
Additionally, our review observed that most CUD patients can benefit from psychosocial interventions, aligned with studies that suggest that some patients may not require abstinence-based medical treatment depending on the severity of their CUD, and that treatment should be conducted in a stepwise manner.35,48 For instance, 3-year naturalistic follow-up study observed that most CUD patients had achieved complete or partial remission of cannabis use and were no longer within the diagnostic criteria.51,52 Considering that abruptly interrupting cannabis use instead of gradually decreasing may cause compensatory use of other, more harmful substances, developing strategies for safer cannabis use can prevent upscaling their associated risks and harms.53–55
Finally, a finding explored by Lintzeris et al. 26 shows that 82.4% of participants from the experimental group could guess that they were using the medication. Recent studies have shown that while CBD+THC (nabiximols) may have a good level of blinding efficacy, there are several ways in which participants may become unblinded during a trial. This includes correctly guessing their allocation group, being randomly tested for substances during traffic stops, and intentionally unblinding themselves using THC urine tests, which can easily be purchased.56–58 Although all studies adopted adequate blinding procedures, the success of blinding is rarely examined or reported across the SUD literature.
OUD studies
The RCT conducted by Bisaga et al. 29 found that while participants in the THC group exhibited a reduction in withdrawal symptoms during the initial stages of the trial, this effect was not maintained during the outpatient phase. The authors suggested that the small sample size (n=60) and limited duration of the withdrawal period may have been contributing factors to this lack of sustained efficacy. These findings suggest that while THC may have potential as a treatment for the acute phase of opioid withdrawal, its effectiveness in managing protracted or naltrexone-induced withdrawal remains uncertain and warrants further investigation.
In a later within-subject experiment, THC administration was associated with tachycardia among OUD patients. Although reductions in withdrawal severity were observed, they were not superior to those produced by oxycodone. This has led to a cessation of clinical trials investigating the use of THC as a treatment for OUD.59,60 However, while oxycodone is still commonly used as a medication-assisted therapy for OUD, it plays a significant role in the ongoing opioid epidemic due to its aggressive marketing campaign, which have been linked to the rising use of heroin and synthetic opioids. Therefore, it is crucial to continue exploring alternative, nonopioid medications for OUD.61–63
Another limitation in the RCT by Bisaga et al. 29 is that baseline measures showed that participants in the THC group presented significantly higher rates of cocaine use than the placebo group (p=0.03). These differences can lead to selection and confounding bias. They may increase the likelihood of type II error, making it difficult to determine the true effects of THC on OUD treatment. Additionally, it was observed that both the experimental and placebo groups presented alcohol consumption levels that exceeded low-risk levels at baseline. Hurd et al. 30 also observed a history of multiple substance use among participants, including CUD, Alcohol Use Disorder, and tobacco smoking. This polysubstance use may have influenced the outcomes of the study, as the severity and development of SUDs were not monitored throughout the studies. 64
In both OUD RCTs, participants predominantly used heroin, but with different routes of administration: Bisaga et al. 29 reported intravenous use as the most common form (50%), while intranasal use was the most common (33%) among participants in Hurd et al. 30 The severity of withdrawal symptoms may differ between these routes, as injecting results in higher levels of the substance in the bloodstream. The variety of heroin found on the illegal market may also have different chemical characteristics and health impacts, highlighting the need to monitor the route and type of heroin used in future studies for better insights.62,65 Additionally, the participation of patients attempting to sustain abstinence in cue-induced craving experiments may outweigh the benefits of this study design. Three participants relapsed in the study by Hurd et al., 30 highlighting the need for further investigation into the risks and benefits of this approach.
Furthermore, both RCTs examined cannabis use under different approaches: Bisaga et al. 29 discovered that smoking cannabis during the trial positively impacted treatment retention. Participants who used cannabis presented better sleep and anxiety outcomes and were more likely to remain in treatment, regardless of whether they received dronabinol or a placebo. Although this finding is in line with several observational studies indicating that cannabis may be a substitute or adjunct for OUD treatment, the later RCT by Hurd et al. 30 considered cannabis use as an exclusion criterion for their study.44,54,66,67
CoUD studies
The study by Mongeau-Pérusse et al. 31 faced limitations due to the absence of 19.2% of data and a smaller sample size than planned, reducing its statistical power to 56.4%. Conversely, the study by de Meneses-Gaya et al. 32 had a low dropout rate, but its sample size was still small and underpowered. Both studies enrolled populations from vulnerable communities with challenging social conditions and severe concurrent SUDs, which may have impacted the outcomes of the studies. Additionally, the study by de Meneses-Gaya et al. 32 had a high overall risk of bias due to unclear blinding and allocation procedures. For instance, the authors acknowledge that the study participants received differentiated treatment at the facility, which may have influenced the results.
In the Brazilian study, all participants consumed inhaled crack-cocaine, 32 whereas different intake forms were observed in the Canadian study, including inhaled (43%), nasal (24%), and intravenous (10%). Concerningly, one participant developed Hepatitis during the study. 31 Similarly to what was observed among the OUD studies with heroin, different methods of consumption can influence health consequences and increase the risk of exposure to contaminants and diseases, owing to the unavailability of safe supplies and the emergence of new forms of cocaine in illicit markets in different locations.68–71
The CoUD RCTs showed positive outcomes for participants who received medical and psychosocial treatment, similar to the CUD studies. However, inpatient programs often disconnect patients from their routines and environments, posing a challenge for sustained behavioral changes post-treatment. 72 The Brazilian study did not include any follow-up, and dropouts were assumed to have abandoned the institution. This highlights a common drawback of inpatient strategies that focus solely on abstinence.
There are concerns regarding inpatient SUD facilities in Brazil, known as “therapeutic communities,” due to a history of human rights violations and religious activities that may overtake medical care.73–75 While this was not the case in the study by de Meneses-Gaya et al., 32 the shortage of specialized SUD facilities continues to hinder Brazil and many other developing nations. CoUD participants often have a history of higher exposure to infectious diseases, vulnerability, and violence, and these factors must be considered to develop alternative, effective treatments that address these challenges.76–79
Finally, similarly to the latest OUD study, both CoUD studies adopted cue-induced craving experiments to test the efficacy of CBD. While such studies may offer valuable insights into the mechanisms of craving and SUDs, studies that provided follow-up measures observed important rates of relapse and contact with infectious diseases among their participants.30,31
The evolving goals of SUD research with cannabinoid-based medications
The initial RCTs with THC were inconclusive for both CUD and OUD treatment, with one out of three studies demonstrating positive results.23,24,29 Recent RCTs have focused on isolated CBD's effects and demonstrated conflicting results. Methodological constraints and inconsistent findings due to limited sample sizes underline the necessity for improved RCTs since these are the first clinical studies conducted since this scoping review.27,30–32
RCT availability is concerningly limited. CUD studies have had a small number of publications from 2011 to 2020,23–28 while limitations in OUD experiments resulted in a lack of RCT publications investigating the potential of THC or other cannabinoid preparations from 2015 to 2019.29,30 Clinical evidence of cannabinoid-based medications for treating CoUD was only published in 2021, highlighting the scarcity of available studies in the SUD field.31,32 Legal constraints have largely contributed to this scarcity of available evidence, as cannabis and its derivates are still considered dangerous and without therapeutic value in many regions, despite numerous documented medical applications.
In the context of this review, THC (dronabinol) and CBD are synthetic isolated cannabinoid preparations, whereas CBD+THC (nabiximols) are derived from the cannabis plant. 7 Evidence suggests that plant-derived cannabinoid-based medications may present a more extensive therapeutic potential and metabolic profile than synthetic, isolated cannabinoids, however, investigations are still under development.80–85 In this scoping review, RCTs with plant-derived CBD+THC presented some positive potential but were limited to CUD studies only, and results were inconsistent, with two out of three RCTs reporting positive results.24,26,28
While the clinical evidence supporting the use of plant-based CBD+THC extracts for treating SUD is still limited, recent observational studies indicate that the synergistic effects of cannabinoids and other compounds present in cannabis may improve treatment retention and reduce SUD-related harms, as well as rates of other substance consumption among patients with OUD and CoUD, which suggests the need for more investigations on these fields.44,67 Aligned with these findings, the RCT conducted by Bisaga et al. 29 found that cannabis use was associated with increased retention and improved treatment outcomes, regardless of being in the experimental or placebo group. This contributes to the growing body of evidence exploring whether plant-based cannabinoids could be used as a primary treatment or adjunct to first-line medications to improve treatment retention and reduce adverse events, thereby enhancing medical treatment.54,86–88
These findings emphasize the need to recognize the contradictory limited efficacy of currently available cannabinoid-based medications and consider them preliminary evidence in the SUD field. As research progresses, newly developed cannabis extracts may demonstrate extensive clinical effects.89–91 However, access to cannabinoid-based medications is currently limited by federal legal restrictions and scientifically unjustifiable bureaucratic procedures in most countries, which leads to high costs and limited access for patients. 92 Therefore, further research is needed to evaluate their efficacy and practicality as a treatment option for SUD along with the development of cannabis-extracted medications that account for these factors, thus, the currently available RCTs may represent the initial stages of studies developed in this area.90,91
Over time, SUD research with cannabis-based medications has evolved from focusing on achieving abstinence and withdrawal severity23–25,29 to include frequency and quantity of use, mental health, and wellbeing indicators.26–28 The latest trend involves cue-induced craving experiments to understand how specific triggers can lead to substance use and if it can be prevented.30–32 Notably, the rates of relapse and infectious disease transmission observed among participants in cue-induced craving RCTs should not be regarded as typical consequences and underscore the need for approaches that prioritize the wellbeing of vulnerable populations, public health, and ethical considerations. It is crucial to select the appropriate study design for the specific population of SUD patients, which requires consideration of their exposure to risk, social and mental health factors, and ensuring their safety and wellbeing both during and after their participation in the study. 93
Conclusions
Some studies indicate that CBD and THC have significant potential as treatments for severe forms of CUD and OUD, but results are limited, and research in the field of CoUD is inconclusive. To address these limitations, more robust and well-designed RCTs with larger sample sizes, longer follow-up periods, and improved blinding procedures are necessary. Developing new cannabinoid-based medications could provide more consistent and effective treatments for SUD. A comprehensive approach to treatment, including psychosocial and contingency management, and carefully selected methodological designs are critical for ensuring participant safety and maximizing the benefits of these medications.
Footnotes
Acknowledgments
The authors express gratitude to their colleagues Dartiu Xavier da Silveira, PhD and Paulo César Barbosa, PhD who helped developing the early drafts of this review.
Authors' Contributions
J.A.B.F. contributed to the conceptualization, design, data curation, formal analysis, investigation, methodology, project administration, software, validation, visualization, and writing of the original draft, and reviewed and edited the article. R.F. contributed to the conceptualization, data curation, formal analysis, methodology, project administration, supervision, validation, and writing of the original draft, and reviewed and edited the article. T.M.F. contributed to the conceptualization, data curation, methodology, project administration, software, supervision, validation, visualization, and writing of the original draft, and reviewed and edited the article.
Author Disclosure Statement
All authors declare no competing financial interests.
Funding Information
The primary author received a full-time master's degree scholarship by the Coordination of Superior Level Staff Improvement (CAPES) program. No other sources of funding were received.
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.