
Abstract
Background:
The multicenter, randomized, double-blind, parallel-group, phase IIIb CANNA-TICS (CANNAbinoids in the treatment of TICS) trial showed clear trends for improvement of tics, depression, and quality of life with nabiximols versus placebo in adult patients with Gilles de la Tourette syndrome and other chronic tic disorders. Although in general nabiximols was well tolerated, it is unclear whether treatment using this cannabis extract influences driving skills in patients with chronic tic disorders.
Methods:
Here we report results of the “Fitness to Drive” substudy of the CANNA-TICS trial. The key endpoint was fitness to drive as a binary criterion with a computerized assessment at baseline and after 9 weeks of stable treatment (week 13) with nabiximols or placebo. A patient was considered unfit to drive according to the German Federal Highway Research Institute guidelines.
Results:
In the substudy, a total of 64 patients (76.6% men, mean±standard deviation of age: 36.8±13.9) were recruited at two study sites. The number of patients who were fit to drive increased from 24 (55.8%) at baseline to 28 (71.8%) at week 13 among 43 patients treated with nabiximols, and decreased from 14 (66.7%) to 10 (52.6%) among 21 patients who received placebo. The risk difference (nabiximols – placebo) was 0.17 (95% confidence interval=−0.08 to 0.43) in favor of nabiximols. Specifically, only 2 of 24 (8.3%) patients in the nabiximols, but 4 of 14 (28.6%) patients in the placebo group changed for the worse from fit (at baseline) to unfit (at week 13) to drive, whereas 8 of 19 (42.1%) patients in the nabiximols, and only 2 of 7 (28.6%) patients in the placebo group improved from unfit to fit.
Conclusion:
Treatment with nabiximols does not impair skills relevant to driving in those patients with tic disorders who were fit to drive at baseline and even improved fitness to drive in a subset of patients who were unfit to drive before start of treatment.
EudraCT number
: 2016-000564-42
Introduction
Gilles de la Tourette syndrome (TS) is a chronic neuropsychiatric disorder characterized by motor and vocal tics and associated with a range of behavioral disorders including attention-deficit/hyperactivity disorder (ADHD), obsessive-compulsive disorder (OCD), depression, anxiety, and rage attacks. 1 Although the etiology of TS is unknown, there is evidence to suggest an involvement of the endocannabinoid system.2,3 This hypothesis is supported by anecdotal reports (mainly case reports, case series, and open uncontrolled studies) of benefits with use of cannabis-based products 4 and by three small randomized controlled trials that reported significant tic reduction after treatment with oral dronabinol (tetrahydrocannabinol [THC])5–7 in the absence of detrimental effects to patients' neuropsychological performance.8,9 In contrast, from preliminary data it is suggested that cannabidiol (CBD) is not effective in reducing tics. 7 European clinical guidelines for TS position medical cannabis-based agents as an option for cases resistant to usual first-line therapy with dopamine-blocking agents. 10
Only recently, the results of CANNA-TICS (CANNAbinoids in the treatment of TICS), a multicenter, randomized, double-blind, parallel-group, phase IIIb trial, have been published. This study aimed to determine whether nabiximols is superior to placebo in reducing tics and comorbidities in adult patients with TS and other chronic tic disorders in Germany [Clinicaltrials.gov identifier: NCT03087201; Jakubovski et al. 11 ; Müller-Vahl et al. 12 ]. Nabiximols is an oromucosal spray containing balanced quantities of THC and CBD. 13 The primary efficacy endpoint was a reduction from baseline in tic severity of at least 25% on the Total Tic Score of the Yale Global Tic Severity Scale (YGTSS-TTS) 14 after 9 weeks of stable treatment. 11 Although the study formally failed to demonstrate superiority for nabiximols over placebo in the primary endpoint, the results show noticeable indications of improvement in tic severity, depression, and quality of life after treatment with nabiximols. 12
Driving is a complex activity requiring sound visual–auditory–sensory motor coordination. 15 The introduction of the “Cannabis as Medicine” law in Germany in 2017 raised concerns as to whether treatment with cannabis-based medicines might affect patients' ability to drive. 16 If cannabis is used recreationally, in Germany driving is generally not allowed in the presence of a positive THC test (>1 ng/mL). However, this threshold value (and THC limits in general) are highly controversial, because it is known for many years that there is no clear relationship between the degree of observed impairment and the detected THC concentration in blood.17,18 Regarding cannabis-based medicines prescribed and supervised by a medical doctor, there are no clear regulations in Germany at present.
Although some people argue that for medicinal use of cannabis, the same rules should apply as for recreational use, others emphasize that there should be a medical defense for patients prescribed cannabis-based medicines taking it as directed and who are not impaired comparable with other prescription drugs. In practical terms, this means that patients receiving cannabis-based medicines have a primary responsibility to accurately self-assess their driving ability before operating a vehicle. An integrated analysis of an open-label driving study and real-world registries found no impairment of driving performance in patients with multiple sclerosis spasticity during treatment with nabiximols.19,20 With regard to TS, to date, only a single case study has reported improvement in a patient's driving ability after treatment with THC. 21
This article reports the design features and results of the CANNA-TICS substudy “Fitness to Drive,” which assessed patients' fitness to drive before and after 9 weeks of stable treatment with nabiximols or placebo.
Methods
Study design
The design and main features of the CANNA-TICS study are reported elsewhere [Clinicaltrials.gov identifier: NCT03087201; Jakubovski et al., 11 Müller-Vahl et al. 12 ]. In brief, in the CANNA-TICS trial 97 adult patients with confirmed TS or another chronic tic disorder were randomized and treated in a 2:1 ratio to receive nabiximols or matching placebo. The study duration was 17 weeks, which included a 4-week up-titration period, a 9-week maintenance phase, and 4 weeks of follow-up. Main relevant exclusion criteria were other severe psychiatric comorbidities, current diagnosis of substance use or dependence, and use of cannabis or any cannabis-based medicine in the 30-day period before study entry and/or a positive THC urine test at baseline.
For organizational reasons and owing to the expenses of the additional assessments only in two of the six participating TS centers (Hannover, Munich) patients were included in the “Fitness to Drive” substudy. Although it was planned that all patients from these two sites were to be included in the substudy, one patient was unable to participate because of severe vision impairment. Of note, inclusion in the “Fitness to Drive” substudy was even possible without a driver's license.
Specific assessments for the “Fitness to Drive” substudy were conducted at baseline and after 9 weeks of stable treatment with nabiximols or placebo (study week 13). Baseline assessments included the following: (i) patients' specific traffic medical history; (ii) patients' self-assessment of general and current driving ability (including self-assessment of being a safe driver and self-assessed fitness to drive); and (iii) objective assessment of psychomotor skills using the Vienna Test System, 22 a validated, Conformité Européenne-European Conformity-marked computerized assessment that has been approved by the German Federal Highway Research Institute (Bundesanstalt für Straßenwesen [BASt]). The test system has been developed in cooperation with the Austrian Road Safety Board and has been found to be predictive for driving performance. The validity of this method has been confirmed in samples of both healthy controls and clinical samples (for validation and a detailed description see the work of Bukasa et al. 23 and Karner and Biehl 24 ), although it may be discussed critically. 25 In any case, this test criterion complies with current legal regulations in Germany, Austria, and Switzerland, making it mandatory for every driver to certify their adequate psychological fitness.
The key endpoint of the “Fitness to Drive” substudy was defined as a binary criterion according to the BASt guidelines. 26 A patient was considered unfit to drive if he or she had a percent rank <16% on at least one of the following four domains: reaction time and choice reaction, stress behavior capacity, concentration, and perceptual speed. Perceptual speed was measured with the adaptive Tachistoscopic Traffic Perception Test (ATAVT). During the ATAVT images of typical traffic situations are presented to the test subject for 1 sec each. After each image, subjects must respond to a five-answer multiple-choice question on the contents of the displayed situation. Concentration was measured with the Cognitrone, where patients had to match simple figures within a defined time. Subjects are asked to decide if the presented figures are identical or different. Stress behavior capacity was measured on the adaptive Vienna determination test.
Subjects are presented with visual and acoustic stimuli to which they must respond by pressing several buttons, bars, and pedals using both their hands and feet. Reaction time to simple stimulus constellations was measured on the Choice-Reaction Test, in which subjects must respond to a specific combination of visual and acoustic stimuli. Reaching at least a percentage >15 is defined as a prerequisite to driving a car safely, according to the German guidelines for road and traffic safety.
In addition, we classified test results of patients according to previous studies27,28 into “no impairment” (defined as patients with a percent range ≥16 in all subtests), “mild impairment” (defined as patients failed in ≤40% of test values), and “severe impairment” (defined as patients failed in >40% of test values). As the above-mentioned dichotomization does not integrate information about performance above a percentage of 16, from a clinical point of view it seems justified to evaluate driving ability in the group labeled as mildly impaired individually taking into account compensational factors.
Estimation of detectable effects on the key endpoint fitness to drive
The noninferiority margin of the analysis of the key endpoint fitness to drive was based on the expected precision of the risk difference estimate, as the aim was to exclude negative effects as good as possible, while the overall sample size is determined by the primary objective. In the planning of the study, we assumed that at least 43 patients are expected to participate in the assessments of the “Fitness to Drive” substudy, as the Hannover Medical School planned to recruit at least 35 patients and the Ludwig-Maximilians-University Munich planned to recruit at least 8 patients. The determination of the noninferiority margin for the key secondary analysis of “Fitness to Drive” is based on the minimum number of expected patients. If more patients from other centers participate, the power to reject the null hypothesis of inferiority will increase.
With a sample size of 43, corresponding to 29 and 14 patients in the nabiximols and placebo arms, respectively, owing to the 2:1 randomization, we calculated that the risk difference of nabiximols minus placebo is −32% or smaller regarding the proportion of patients fit to drive if the true proportion is 84% in both groups (Wald Test, power=80%, one-sided significance level=2.5%). We further estimated before the study start that if the true proportions are equal and <84%, the power is diminished and if more patients participate in the fitness to drive assessments, and the sample sizes are 40 and 20 in the nabiximols and placebo arms, respectively, the procedure still would have a power of 80% if the true proportions would be 72% in both groups.
Power calculations were performed in nQuery Advisor 7.0 for a test of equivalence in proportions with unequal sample sizes. As the sample size calculation is based on an asymptotic method, it was rechecked with simulation in nQuery Advisor 7.0 based on the lower limit of the confidence interval (CI; test minus standard) by simulation (5000 simulations, seed: 84621354) resulting in a slightly higher power of 84%.
Statistical analyses
As the CANNA-TICS study failed to demonstrate formally the superiority of nabiximols over placebo for the primary endpoint of tic reduction, 12 assessment of the key secondary endpoint of the “Fitness to Drive” substudy can be regarded as exploratory only. In dependency on the primary hypotheses, it was prespecified that if the lower bound of the corresponding 95% CI exceeded the noninferiority margin of −32%, the noninferiority of nabiximols over placebo regarding fitness to drive could be concluded. That implies a minimum difference between nabiximols and placebo of 32% can be excluded. This noninferiority margin was specified at the planning stage based on the minimum difference that can be excluded with adequate power and not justified by relevance. The analysis is intended to exclude signals for detrimental effects on driving ability.
Noninferiority of nabiximols compared with placebo was assessed in the intention-to-treat (ITT) population, that is, in all patients that were included in the “Fitness to Drive” substudy. As per study protocol, patients in the ITT population with missing values for treatment response were designated as unfit to drive. Sensitivity analyses were conducted in the per-protocol (PP) population, that is, all patients who were compliant with the study protocol.
The fitness to drive criterion was analyzed using a Mantel–Haenszel estimate of risk difference (nabiximols − placebo) and respective 95% CI stratified by center. The prognostic value of gender (male/female), age (</≥ median of age), presence of comorbid ADHD (yes/no, detailed definition see Supplementary Methods in Supplementary Data), tic severity (</≥28 YGTSS-TTS), 29 and study drug dose (</≥ median of mean sprays/day in maintenance phase) on the fitness to drive criterion was also investigated by Mantel–Haenszel estimate of risk difference and 95% CIs and depicted by Forest plots.
For the descriptive comparison of the baseline and secondary endpoints mean values and standard deviations (SD) or absolute and relative frequencies per group were calculated. Nabiximols and placebo groups were compared using two-sided t-tests (continuous variables) or χ 2 -tests (categorical variables). Furthermore for the raw data of the five components analysis of covariance (ANCOVA) models were conducted for the change from baseline values on treatment adjusted for the respective baseline.
In all descriptive analyses, missing values were not imputed. Values of p<5% can be interpreted as showing a trend for a difference between nabiximols and placebo. All analyses were performed using SAS 9.4 (Cary, NC).
Ethics statement
The CANNA-TICS study and “Fitness to Drive” substudy were conducted following the principles of International Council for Harmonisation of Technical Requirements for Pharmaceuticals fir Human Use-Good Clinical Practice, the German Drug Law, and the Declaration of Helsinki. The study protocol was approved by the ethics committee of Hannover Medical School as the main committee and by the ethics committees of all participating centers.
Informed consent statement
Written informed consent was obtained from all individuals participating in the study.
Results
A total of 64 patients participated in the “Fitness to Drive” substudy (Fig. 1), of which 51 (80%) comprised the PP population. Most patients (54 [84%]) were recruited at the TS center in Hannover (Site 1).
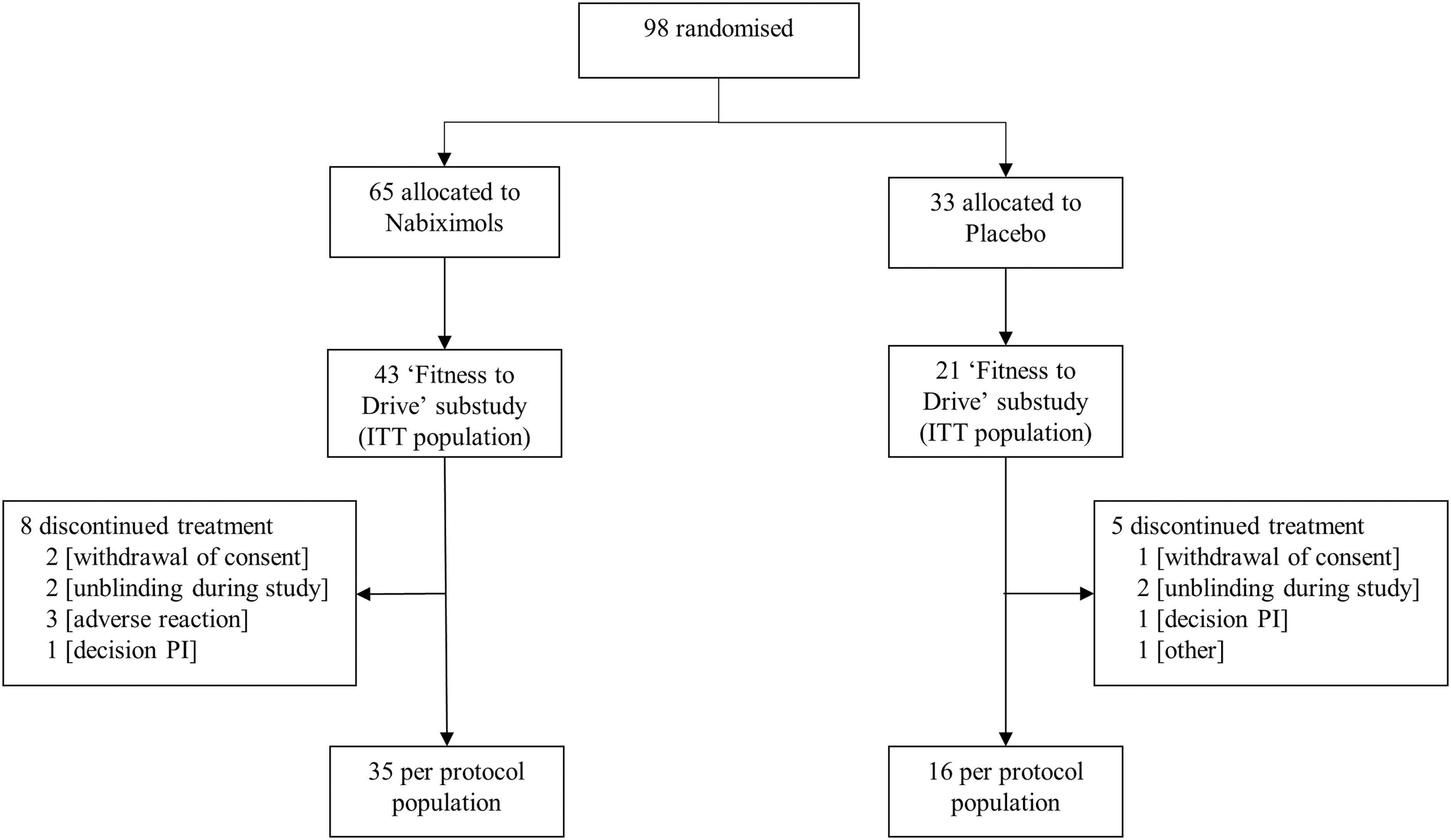
Patient disposition.
Baseline demographic and clinical characteristics of the substudy cohort are summarized in Table 1. The study population was predominantly men (77.6%), mean age was 36.8 years (SD=13.9), and mean age at tic onset was 8.3 years (SD=4.9). Most patients had TS (95.3%). Tic severity was similar between nabiximols and placebo groups. Treatment groups were comparable for family history of tics and psychiatric comorbidities. The proportion of patients receiving concomitant anti-tic and other psychopharmacological medication at baseline was notably higher among those treated with nabiximols. Nine patients (20.9%) in the nabiximols group presented comorbid ADHD versus none in the placebo group. There was a tendency toward higher incidences of anxiety, OCD, and rage attacks in the nabiximols group. In addition, no significant differences were observed between treatment groups at baseline for specific traffic medical history (Supplementary Table S1).
Baseline Characteristics of Patients in the “Fitness to Drive” Substudy
Data are expressed as absolute and relative frequencies or mean±standard deviation per treatment group for all patients who were included in the “Fitness to Drive” substudy (intention-to-treat population).
Values are missing for one patient in the placebo group.
Definition of ADHD can be found in the Supplementary Methods in Supplementary Data.
ADHD, attention deficit/hyperactivity disorder (detailed definition see Supplementary Methods in Supplementary Data); BAI, Beck Anxiety Inventory 35 ; BDI-II, Beck Depression Inventory-II 36 ; OCD, obsessive–compulsive disorder; RAQ, Rage Attacks Questionnaire 37 ; Y-BOCS, Yale-Brown Obsessive Compulsive Scale38,39; YGTSS-TTS, Yale Global Tic Severity Scale–Total Tic Score. 14
In the primary analysis of fitness to drive (Table 2), the number of patients who were fit to drive increased from 24 (55.8%) at baseline to 28 (71.8%) at week 13 with nabiximols, and decreased from 14 (66.7%) at baseline to 10 (52.6%) at week 13 with placebo. The respective patient flow is given in Figure 2. The fitness to drive responder criterion showed a risk difference (nabiximols – placebo) of 0.17 (95% CI=−0.08 to 0.43) in favor of nabiximols in the ITT population. Results were consistent in the PP population (0.14; 95% CI=−0.15 to 0.42). As the lower bound of the corresponding CI was above the noninferiority margin of −32%, the noninferiority of nabiximols is shown.
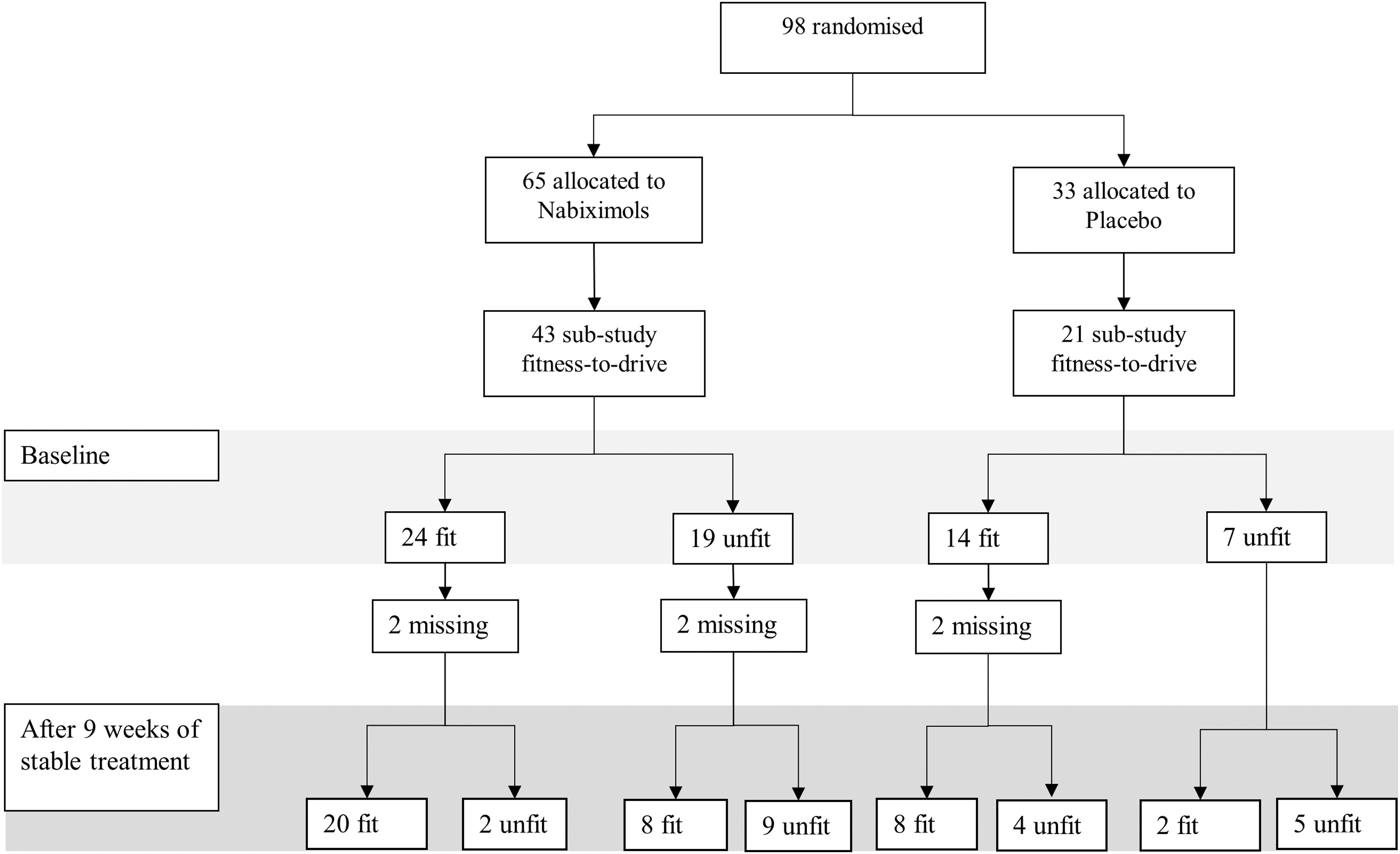
Patient flow chart for primary endpoint (intention-to-treat population).
Results of Specific Fitness to Drive Endpoints
Data are expressed as absolute and relative frequencies per treatment group for all patients which were included in the “Fitness to Drive” substudy (intention-to-treat population).
The risk difference was consistent for gender, age, presence of comorbid ADHD, baseline tic severity, and dosage of study drug in the ITT (Fig. 3) and in the PP (Supplementary Fig. S1) population. Of interest, we observed a greater benefit in patients with lower tic severity at baseline (YGTSS-TTS <28, risk difference=0.41; 95% CI=0.02–0.80). The more clinical evaluation with the fitness to drive three-point categorical scale revealed that with nabiximols the number of patients with mild impairment decreased from 17 (39.5%) to 11 (28.2%) and with severe impairment from 2 (4.7%) to 0 patients. In contrast, in the placebo group, the number of patients with mild impairment increased from 7 (33.3%) to 9 (47.4%), whereas in neither group a patient exhibited severe impairment (Table 2).

Forest plot of subgroup analysis for the “fit to drive” criterion (intention-to-treat population). Displayed are absolute and relative numbers per treatment group and RD with respective 95% CIs. *Stratified for study center. ADHD, attention-deficit/hyperactivity disorder; CI, confidence interval; RD, risk differences; YGTSS-TTS, Yale Global Tic Severity Scale–Total Tic Score.
Irrespective of the treatment group, at baseline the vast majority of patients (92.1% and 95.2%, respectively) considered themselves to be a “safe driver” and all patients (100%) considered themselves to be “fit to drive.” Changes in patients' self-assessment of driving ability at week 13 were minimal (Table 2).
ANCOVAs of raw values of the components of the BASt guidelines 26 showed statistical differences with respect to mean reaction time between patients treated with nabiximols compared with placebo. For all other components, no differences were observed between treatment groups (Table 3).
Results of Raw Values of the Components of the German Federal Highway Research Institute (BASt) Guidelines
Presented are results from ANCOVAs of the change from baseline values for the five components adjusted for baseline for all patients, which have available data for the fitness to drive test at both visits. For each component, LSM for the changes in the nabiximols and placebo group and LSM for difference of the changes including 95% CIs and p-values are reported.
ANCOVA, analysis of covariance; CI, confidence interval; LSM, least square means.
No differences were observed between patients who were fit to drive (n=38) compared with those unfit to drive (n=26) with respect to concomitant anti-tic medication, other concomitant psychopharmacologic medication, or comorbid ADHD (detailed results see Supplementary Table S2). In addition, we observed no differences in tic severity as assessed by YGTSS-TTS between patients deemed unfit or fit to drive, in both the nabiximols and the placebo group (Supplementary Fig. S2).
On average, patients in the nabiximols group (n=38) used 6.83±3.41 puffs/day corresponding to 18.4 mg THC and 17.1 mg CBD during the maintenance phase. Similar to findings in the CANNA-TICS study the average dose in the placebo group was higher (n=21, 9.0±3.38 puffs/day, p=0.0226).
Discussion
The ability to drive is important for most people in terms of employment, social activities, and general independence. In patients with neurological and psychiatric disorders, daily life activities such as driving may be compromised by the condition itself or by medications used to treat the condition. At present, knowledge about the influence of cannabis-based medicines on driving ability in patients with tic disorders is limited. CANNA-TICS was the first large, double-blind, randomized, controlled study of nabiximols to be conducted in patients with TS or other chronic tic disorders and is particularly relevant given the current positioning of cannabis-based medicines as an option for patients with treatment-resistant disease. 10
According to the Vienna Test System, 22 the objective driving ability assessment indicated an increase in the proportion of patients who were fit to drive after 9 weeks of stable treatment with nabiximols but not placebo. The Mantel–Haenszel estimate of risk difference allowed us to conclude that nabiximols is noninferior to placebo with regard to fitness to drive in patients with TS or other chronic tic disorders. However, because CANNA-TICS formally failed to demonstrate superiority for nabiximols over placebo in the primary endpoint, 12 the results can be interpreted as exploratory only. Nevertheless, our results compare favorably with those of a driving ability study of nabiximols conducted in patients with treatment-resistant multiple sclerosis where frequencies of patients classified as “fit” or “unfit” to drive based on the Vienna Test System 22 did not change between baseline and study end. 19
The positive results in our study may be attributable to the variation in clinical manifestations of chronic tic disorders versus multiple sclerosis, which may affect driving differently, differences in positive treatment effects between both disorders using nabiximols, the higher dose used (on average 6.8 puffs/day in the “Fitness to Drive” study during the maintenance phase vs. 5.1 puffs/day 19 in the multiple sclerosis study), and the longer treatment duration (9 vs. 6 weeks).
The fitness to drive responder criterion showed a risk difference of 0.17 (95% CI=−0.08 to 0.43) in favor of nabiximols over placebo in the ITT population. A subgroup analysis according to selected baseline characteristics and dose of the study drug indicated that patients with lower tic severity at baseline (<28 YGTSS-TTS) experienced greater benefit from nabiximols than those with a higher baseline YGTSS-TTS. Conversely, factors such as gender, age, presence of comorbid ADHD, and study drug dose had no prognostic value for predicting the benefit of nabiximols.
At baseline, 56% of nabiximols-treated patients and 67% of placebo-treated patients were assessed as fit to drive according to the validated computerized test battery. By their own assessment, 100% of evaluable patients in both treatment groups considered themselves fit to drive at baseline. This self-estimation of driving ability is consistent with an international survey study in which 91.5% of individuals with TS or chronic tic disorders reported no to minimal interference of tics on their driving ability. 30 The discordance between objective testing and patients' subjective assessment of their driving ability merits further consideration given that primary responsibility rests with the individuals themselves. It has been suggested that persons with tic disorders be screened for severe motor tics, which may affect their driving ability to prevent harm to themselves and others. 15
The presence of psychiatric comorbidities in patients with tic disorders may further impact their fitness to drive. A large (n>6 million) population-based cohort study found an increased risk of serious transport injuries in individuals with TS or chronic tic disorders compared with the general population (HR=1.50; 95% CI=1.33−1.69) or unaffected siblings (HR=1.41; 95% CI=1.18−1.68) that was driven mainly by comorbid ADHD. 31 However, in a case study from 2007, a 28-year-old man with significant ADHD symptoms showed improvement in driving performance tests (four subtests of ART2020 and the attention test module TAP) after smoking cannabis, suggesting atypical or potentially performance-enhancing effects of THC in patients with ADHD. 32 In line with this case report, in our study, the nabiximols group performed better in driving ability tests despite a higher incidence of comorbid ADHD compared with the placebo group (21% vs. 0%).
In the CANNA-TICS study, the maximum dose of study drug was 12 sprays/day (corresponding to 32.4 mg THC and 30 mg CBD) in the nabiximols group as per approved nabiximols posology for the treatment of multiple sclerosis spasticity (Sativex® SmPC). However, on average, patients in the nabiximols group (n=56) used 7.21±3.42 puffs/day (corresponding to 19.5 mg THC and 18 mg CBD) during the maintenance phase, which was significantly less compared with the placebo group (n=32, 9.19±3.07 puffs/day). 12 In the subsample of the “Fitness to Drive” study similar doses were used in both groups. This dose range is in line with general recommendations for the use of nabiximols and THC, respectively, in different patient groups.4,5,7,8,33
The study has several limitations. Since nabiximols is a fixed-dose combination of THC and CBD, the results may not extend to all cannabis-based medicines. There is preliminary evidence to suggest that the beneficial effects of medical cannabis in patients with TS may be attributable to THC, rather than CBD, although in Abi-Jaoude et al.'s study THC was associated with more adverse events (mainly cognitive and psychomotor) than THC/CBD or CBD. 7 The modest sample size, especially in the placebo group, limits generalizing the results to the wider population of patients with TS as tic type and severity can vary considerably among patients. Because it is well-known that there is no relation between THC blood concentrations and patients' driving performance,17,18 we decided not to investigate THC concentrations. Based on a 9-week maintenance phase, no conclusions can be drawn about the long-term effects of nabiximols on driving ability. Although additional use of cannabis can be excluded in the placebo group, it cannot be entirely excluded in the nabiximols group given that THC is a component of nabiximols. 34 A “learning effect” may exist when using computerized tests, although assumedly would have affected patients in both treatment groups. Finally, despite the use of the validated Vienna Test System 22 to measure skills relevant to driving, driving performance is more realistically assessed in on-the-road tests than in an experimental design.
Notwithstanding these limitations, the results show that nabiximols has the potential to improve driving ability in patients with TS and other chronic tic disorders even in the presence of comorbid ADHD and further pharmacotherapy. Our results corroborate the assumption that treatment of TS with cannabinoids results in comprehensive improvement of the disease. Further studies involving larger numbers of patients treated for a longer duration would be worthwhile to confirm these preliminary results.
Footnotes
Acknowledgments
The authors express their gratitude toward patients who participated in this trial. The authors thank the German advocacy groups Tourette Gesellschaft Deutschland e.V. and Interessenverband Tourette Syndrom e.V. for their help with the recruitment of patients.
The authors thank the Center for Clinical Trials at Hannover Medical School for their support in performing the study as well as Ms. Daniela Ihlenburg-Schwarz, Martina Lenz-Ziegenbein, Martina Haas, Bettina Baltin, and Susanne Brunke from Hannover for their continued support in several different parts of the study.
The authors thank the DFG (German Research Association) for funding of the study and GW Pharmaceuticals Ltd. for providing the study medication.
Medical writing assistance was provided by Kerry Dechant, ISMPP CMPP™ on behalf of Content Ed Net (Munich, Germany).
Authors' Contributions
Study concept and research design: K.R.M.-V., A.P., A.B. Methodology: K.R.M.-V., A.P., A.B., C.-L.C., E.B.J., R.R., A.G. Data organizing: K.R.M.-V., A.P., C.F., R.M. Writing—original draft preparation: K.R.M.-V., R.R., A.G. Editing: A.P., A.B., C.-L.C., E.B.J., R.M. Supervision: K.R.M.-V., A.B., A.G. Funding acquisition: K.R.M.-V. All authors have read and agreed to the published version of the article.
Author Disclosure Statement
K.R.M.-V. received financial or material research support from European Union (FP7-HEALTH-2011 No. 278367, FP7-PEOPLE-2012-ITN No. 316978), German Research Foundation (DFG) (GZ MU 1527/3-1 and GZ MU 1527/3-2), Federal Ministry of Education and Research (01KG1421), National Institute of Mental Health, Tourette Gesellschaft Deutschland e.V. Else-Kröner-Frese-nius-Stiftung, GW Pharmaceuticals, Almirall Hermal GmbH, Abide Therapeutics, and Therapix Biosciences. She has received consultant's honoraria from Abide Therapeutics, Boehringer Ingelheim International GmbH, Bionorica Ethics GmbH, CannaMedical Pharma GmbH, Canopy Grouth, Columbia Care, CTC Communications Corp., Demecan, Eurox Deutschland GmbH, Global Praxis Group Limited, IMC Germany, Lundbeck, Sanity Group, Stadapharm GmbH, Synendos Therapeutics AG, and Tilray. She is an advisory/scientific board member for CannaMedical Pharma GmbH, Bionorica Ethics GmbH, CannaXan GmbH, Canopy Growth, Columbia Care, IMC Germany, Leafy Deutschland GmbH, Sanity Group, Syqe Medical Ltd., Therapix Biosciences Ltd., and Wayland Group. She has received speaker's fees from Aphria Deutschland GmbH, Almirall, Cogitando GmbH, Emalex, Eurox Deutschland GmbH, Ever Pharma GmbH, Meinhardt Congress GmbH, PR Berater, Spectrum Therapeutics GmbH, Takeda GmbH, Tilray, Wayland Group. She has received royalties from Deutsches Ärzteblatt, Der Neurologie und Psychiater, Elsevier, Medizinisch Wissenschaftliche Verlagsgesellschaft Berlin, and Kohlhammer. She served as a guest editor for Frontiers in Neurology on the research topic “The neurobiology and genetics of Gilles de la Tourette syndrome: new avenues through large-scale collaborative projects,” is an associate editor for Cannabis and Cannabinoid Research and an Editorial Board Member of Medical Cannabis and Cannabinoids and MDPI-Reports and a scientific board member for Zeitschrift für Allgemeinmedizin.
R.M. has received financial research support from the EU (H2020 No. 754740), the Tourette Gesellschaft Deutschland e.V., Abide Therapeutics, Böhringer-Ingelheim, Emalex, Lundbeck, Nuvelution TS Pharma, Inc., Otsuka Pharmaceuticals, and Therapix Biosciences. He has received speakers' honoraria from Otsuka Pharmaceuticals and Lundbeck. R.M. is member of the advisory board of the Tourette Gesellschaft Deutschland e.V.
A.B. received speakers honoraria, financial research support and travel grants from Recordati Pharma GmbH and Schuhfried GmbH within the last 3 years. He received royalties from Medizinisch Wissenschaftliche Verlagsgesellschaft Berlin, is a member of the executive board of the Deutsche Gesellschaft für Verkehrsmedizin and in the panel of experts of the BASt.
A.P., E.W., C.-L.C., C.F., E.B.J., R.R. and A.G. have no commercial or financial conflicts of interest.
Funding Information
The CANNA-TICS study was funded by the DFG (GZ MU 1527/3-1 and GZ MU 1527/3-2). GW Pharmaceuticals Ltd. (Cambridge, United Kingdom) provided nabiximols and placebo for the study. Almirall (Barcelona, Spain) kindly offered funding for the “Fitness to Drive” substudy. Almirall holds marketing rights to Sativex in Europe (except in the United Kingdom).
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.