
Abstract
Background:
The literature supports the benefits of medical cannabis for core and comorbid symptoms in autistic individuals and anxiety-related symptoms in individuals without autism. However, no study has specifically investigated how cannabidiol (CBD)-rich cannabis affects anxiety subtypes in autistic children or its relationship with restricted and repetitive behaviors and interests (RRBI). Understanding the effects of CBD-rich cannabis treatment on anxiety subtypes and RRBI could offer more precise treatment approaches to managing anxiety symptoms and reducing RRBI frequency in autistic children.
Objectives:
To examine (1) the impact of CBD-rich cannabis treatment on autistic children’s (1a) anxiety levels and subtypes and (1 b) RRBI and subtypes and (2) whether changes in anxiety explain changes in RRBI following cannabis treatment.
Method:
In this open-label study, we analyzed data from 65 autistic children (5–12 years) who had participated in research on the effects of CBD-rich cannabis on children with autism. Their parents completed the Repetitive Behavior Scale-revised to assess the frequency and severity of six subgroups of their children’s recurrent behaviors and the Screen for Child Anxiety-Related Emotional Disorders for symptoms related to five types of anxiety disorders. They completed these assessments at three time points: (T1) before treatment, (T2) after 3 months, and (T3) after 6 months of treatment.
Results:
The results indicated reduced RRBI and symptoms related to various anxiety subtypes in autistic children following 6 months of CBD-rich cannabis treatment. Specifically, we observed significant differences in the autistic children’s overall anxiety and in some anxiety subtypes (i.e., general, social, panic, and separation anxieties). Significant improvements were observed in RRBI, including the total score, and specifically in compulsive, ritualistic, and sameness behaviors. Our findings revealed that reduced anxiety, particularly within the panic- and separation-related subtypes, predicted a subsequent decrease in RRBI, specifically sameness behaviors, following cannabis treatment.
Conclusions:
The findings of the cannabis treatment’s potential benefits for alleviating anxiety symptoms, leading to reduced RRBI, may provide evidence for the meaningful relationship between these variables and for the potential benefits of cannabis treatment for autistic children. We strongly recommend further double-blind, placebo-controlled studies using standardized assessments to validate these findings.
Introduction
Autism spectrum disorder
Autism spectrum disorder (ASD) is a lifelong neurodevelopmental disorder characterized by distinct features manifesting in various domains. 1 The ASD diagnostic criteria include two primary impairment areas: (a) social communication and interaction and (b) restricted and repetitive behaviors and interests (RRBI). 1 The RRBI are a collection of behaviors related to repetition, rigidity, fixation, and resistance to change. They include stereotyped or repetitive speech, movement, or use of objects; routines, rituals, and resistance to change; highly restricted and fixated interests; and hypo- or hyperreactivity to sensory input, including unusual sensory interests. 1 These behaviors tend to persist throughout the lifespan of autistic people.2–4 They significantly affect all aspects of an autistic child’s functioning and may present a major source of stress for child’s caregivers and family.3–5
The RRBI features are frequently classified into two groups: (a) low-order or repetitive sensory–motor behaviors (repetitive body movements or object manipulation and sensory-seeking actions) and (b) high-order behaviors (e.g., insistence-on-sameness behaviors, restricted interests, and ritualized verbal patterns).6,7 Children with ASD also commonly exhibit maladaptive behaviors, such as aggression, tantrums, hyperactivity, impulsiveness, noncompliance, and self-injury.8,9 Moreover, co-occurring anxiety symptoms could exacerbate the effects of ASD core symptoms and other maladaptive behaviors. 10
Anxiety in ASD
According to the Diagnostic and Statistical Manual of Mental Disorders (DSM; 5th edition), 1 anxiety disorders are diagnosed when an individual experiences excessive developmentally inappropriate fears or worries for more than 6 months. These fears are associated with three or more of the following symptoms: restless or feeling keyed-up or on edge, easily fatigued, difficulty concentrating or mind going blank, irritability, muscle tension, and sleep disturbance. Specific anxiety disorders commonly seen in children with ASD include general (characterized by ongoing, excessive worry lasting at least 6 months), panic (unexpected, repeated panic attacks), separation (excessive and developmentally inappropriate anxiety related to separation from home or attachment figures), and social (pronounced anxiety in particular social or performance situations, often resulting in avoidance behaviors and school anxiety).1,11,12
Research indicated that approximately 40% of autistic children and adolescents are diagnosed with at least one anxiety-related disorder 13 that substantially affects their lives. 14 Many autistic children may experience “subclinical anxiety,” 15 characterized by features that do not meet diagnostic criteria for anxiety disorders. 16 If left untreated, anxiety symptoms can persist from childhood into adolescence 17 and even adulthood. 18
Although all humans experience some fear and worry in their daily lives, anxiety can escalate stress levels and lead to more disruptive behaviors, such as self-injury, depression, aggression,19,20 and exacerbate core ASD symptoms like RRBI. 20 Ben-Sasson and Stephenson 21 offered three possible explanations for co-occurring anxiety and RRBI symptoms and their relationship in ASD: RRBI are a response to anxiety, anxiety results from RRBI, and neurobiological mechanisms (e.g., greater amygdala activation or oxytocin) and common mediators (e.g., intolerance of uncertainty) are common to both RRBI and anxiety.
Because ASD and anxiety disorders are complex, interventions for them are numerous. Interventions may be behavioral, rehabilitation-based, emotional, or pharmacological in nature. 22 Commonly prescribed medications such as antipsychotics and Selective Serotonin Reuptake Inhibitors (antidepressants) are used to treat ASD’s comorbidity symptoms but do not target its core symptoms.22,23 Around 40% of individuals with ASD seeking treatment for severe behavioral problems may not respond well to medication. 24
The challenges of finding effective treatment for ASD and anxiety symptoms lead parents and professionals to search for alternative therapies and eventually try medical cannabis. Currently, over 100 cannabinoids have been identified in the cannabis plant. Past research has concentrated on the two primary cannabinoids, tetrahydrocannabinol (THC) and CBD. THC activates the endocannabinoid system by binding to CB1 and CB2 receptors in the brain, leading to effects such as sensory alterations, euphoria, sedation, and appetite changes. However, high THC doses can cause anxiety and negatively affect brain development and memory.25–28 In contrast, CBD has numerous therapeutic properties, including sedative, anticonvulsant, sleep-inducing, antianxiety, antipsychotic, and anti-inflammatory effects. It promotes neurogenesis and acts as an antioxidant.29–31 Although both substances are neuroactive, THC is primarily responsible for the psychoactive sensations.
The ability to isolate the main cannabinoids has enabled the use of cannabis for medical treatment by adapting doses and tailoring interventions to meet medical needs. Recent open-label studies have shown the potential benefits of CBD-rich cannabis in treating autistic children.32–34 Other open-label studies found it benefitted anxiety symptoms in people without ASD.32–34 A recent review demonstrated CBD-rich cannabis’s potential for treating anxiety in animal studies and double-blind studies with healthy human volunteers. 34
In the past decade, the U.S. Food and Drug Administration approved the use of epidiolex, a pure cannabis-derived CBD compound, for treating two severe forms of epilepsy. 35 Notably, parents of autistic children undergoing CBD-rich cannabis for epilepsy reported improvements in ASD symptoms, 36 and a recent review described other studies demonstrating its effectiveness for conditions and symptoms associated with ASD. 37 These significant findings prompted further research indicating the efficacy and safety of cannabis treatment for children with ASD.38–41
These open-label studies reported improved ASD core symptoms37,38,40–42 and reduced comorbid behavioral symptoms, including self-injury, tantrums, restlessness, and anxiety.38–40,42 Common side effects were found to be mild and temporary, such as appetite changes, gastrointestinal symptoms, somnolence, irritability, psychoactive effects, and sleep disturbances.40,41,43,44
To date, only two blinded placebo-controlled studies on medical cannabis to treat symptoms associated with ASD in children have been published.43,45 The former compared the efficacy of an oral cannabinoid solutions at a 20:1 CBD to THC ratio with a solution of pure CBD and pure THC at the same ratio to the placebo. The results demonstrated improvements in disruptive behaviors in 49% of participants in the whole-plant extract group compared with 21% in the placebo group. The whole-plant extract group’s median social responsiveness scores improved by a mean of 14.9 points (versus 3.6 points after placebo). The latter study used CBD-rich cannabis in a ratio of 9CBD:1THC and found improved social interaction, anxiety, psychomotor agitation, number of meals per day, and concentration.
Although the literature supports the positive effects of CBD-rich cannabis treatment on ASD core symptoms and comorbid behavioral symptoms for autistic children, no research specifically examined its treatment impact on autistic children’s RRBI and anxiety subtypes or the relationship between the two in light of CBD-rich cannabis treatment. Hence, our study aimed to examine (1) the impact of CBD-rich cannabis treatment on children’s (1a) anxiety levels and subtypes and (1b) RRBI subtypes and (2) whether changes in anxiety explain changes in RRBI after CBD-rich cannabis treatment.
Method
Participants
Initially, participants comprised 87 autistic children (5–12 years old; M = 7.39 years, SD = 2.02): 71 (81.6%) boys and 16 (18.4%) girls. Sixty-five (74.7%) children completed the 6-month treatment; the other 22 (25.3%) dropped out before it ended. The dropout reasons included adverse effects, such as worsened functioning (n = 2), violence (n = 3), abdominal pain (n = 1), weight gain (n = 1), and sleeping problems (n = 1); parents feeling “the treatment did not work” (n = 9); and intake difficulty and parent–child cooperation issues (n = 5).(See 46 )
We analyzed data from the 65 children who completed the 6-month cannabis treatment (5–12 years old, M = 7.37 years, SD = 2.05). Among the participants, 53 (81.5%) were boys, and 12 (18.5%) were girls. We measured weight (M = 30.69 kg, SD = 13.45), height (M = 128 cm, SD = 17.13), and Z-scores (M = .52, SD = 1.54). On average, participants demonstrated moderate-to-severe ASD severity, as indicated by Autism Diagnostic Observation Schedule™ 2nd edition (ADOS-2) 47 scores (M = 8.38, SD = 1.61). Of the 65 autistic children, 20 (30.7%) used prescribed medications (Table 1).
Concurrent Medications Taken by Participants during the Study (n = 20/65)
Procedure
We recruited participants via social media platforms and in collaboration with the Israeli Society for Autistic Children, ALUT. A specialized pediatric neurologist with expertise in ASD interviewed the parents of prospective participants. The parents detailed their children’s medical information, including ASD diagnosis and concurrent medications (Table 1). Inclusion criteria were children aged 5–12 years with a medical diagnosis of ASD recognized by the Ministry of Health and confirmed by the ADOS-2 47 and parental reports of disruptive child behaviors persisting for at least 6 months. Exclusion criteria were children with known genetic syndromes that cause autism symptoms, with diagnosed metabolic diseases, or whose parents had severe mental health problems (e.g., psychosis or drug addiction).
We advised parents of participants who were using medications before the study not to change their child’s regimen during the study period. We personalized the medicine approach in the cannabis treatment protocol for each participant. All received a medical cannabis extract infused in medium-chain triglycerides (MCT) oil with a CBD:THC ratio of 20:1 (Nitzan Spectrum®, Seach Medical Group, Israel) for 6 months. This CBD:THC ratio was chosen based on open-label studies that found it safe and effective for autistic children.36,39,43 Moreover, the decision to treat autistic children with CBD-rich cannabis was motivated by concerns about THC-rich cannabis side effects.25,48
All participants began with a daily dosage of one drop (each drop contained 0.3 mg THC and 5.7 mg CBD). The dosage was then gradually increased until parents reported improvement in their child’s condition. The timing of the doses throughout the day was customized based on individual requirements, such as higher doses at night if necessary for sleep support. The final dosage did not surpass 10 mg/kg/day (total 400 mg/day) of CBD and 0.5 mg/kg/day (total 20 mg/day) of THC. By the end of treatment, the mean total daily CBD:THC doses were 2.87(SD = 1.22): 0.15 (SD = 0.062) mg/kg body weight. The CBD:THC range doses were 0.42–6.67 CBD: 0.02–0.35 THC mg/kg body weight.
We conducted biweekly follow-up interviews throughout the 6-month study to gather information on any changes in the child’s behavior, participation, health, or comorbid symptoms and to ensure safety. The participants visited the medical center before the treatment started (T1), after 3 months (T2), and at the end of the treatment period, after 6 months (T3).
At all three timepoints, parents completed the Repetitive Behavior Scale-revised (RBS-R) 2 to examine the frequency and severity of recurrent behaviors they observed in their child and the Screen for Child Anxiety-Related Emotional Disorders (SCARED), 49 which screens for children with anxiety disorders. At T1, they also completed the demographic data questionnaire. We analyzed each variable from the 65 children who completed the 6-month cannabis treatment only if the parents reported the relevant information at all three time points.
Measures
Medical demographic questionnaire
This questionnaire comprised demographic and medical inquiries encompassing variables such as age, gender, co-occurring diagnoses, and medications.
RBS-R
Parents completed the RBS-R, 2 which assesses the frequency and severity of recurrent behaviors observed in autistic individuals over the past month. It comprises 43 items rated on a four-point Likert scale from 0 (behaviors do not occur) to 3 (behaviors occur and are a serious problem). 2 These items are categorized into six subgroups: stereotypic, self-injurious, compulsive, ritualistic, sameness, and restricted behavior. Subscores and total scores are obtained by summing all related items. The questionnaire has demonstrated good reliability 50 and test–retest reliability 51 in the autistic population.
SCARED
The 41-item parent-reported SCARED assesses symptoms related to the five types of anxiety disorders appearing in the DSM-IV. 52 Higher scores indicate greater levels of worry. The SCARED has demonstrated good convergent and divergent validity.49,52
Data analysis
We processed data for the quantitative study using IBM SPSS (version 27). The participants’ demographic characteristics were described using descriptive statistics. Owing to non-normally distributed data, we used Friedman tests to examine the treatment effects on the frequency and severity of recurrent behaviors in children and symptoms related to five anxiety disorder types. We conducted Wilcoxon signed-rank tests to determine whether there were significant differences between time period frequencies. Nonparametric tests, specifically Spearman correlations, were used to examine the association between the SCARED and the RBS-R after treatment. In addition, we conducted multiple regression analyses to explore the anxiety type’s contribution in predicting the severity of RRBI scores after treatment.
Results
Descriptive statistics
Of the 65 participants, 20 (30.7%) took concurrent medications during the study, including sleep remedy treatments (Table 1). Table 2 presents descriptive data with the RBS-R and SCARED overall and subscores at T1, T2, and T3. Figure 1 shows category means.
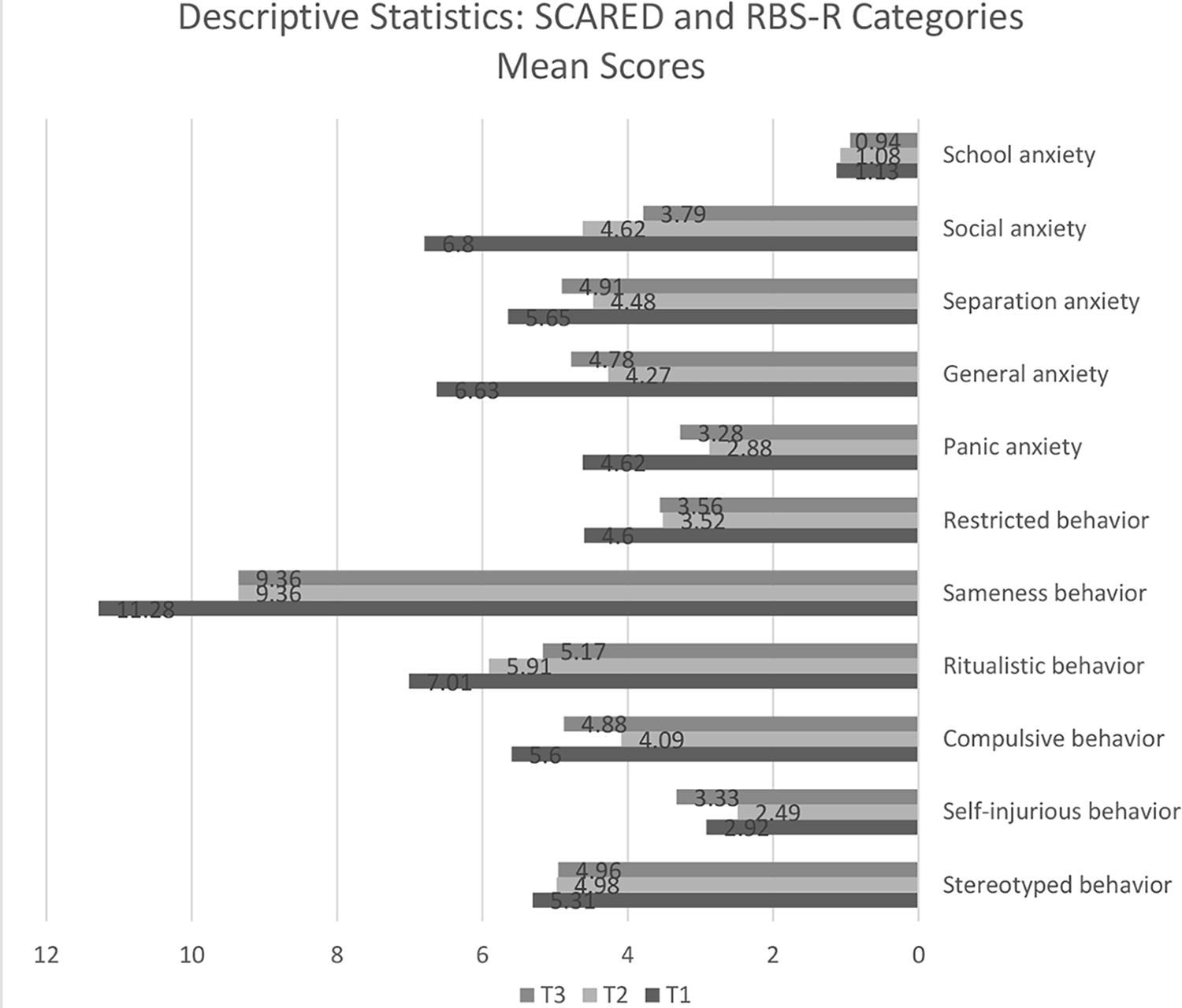
Descriptive statistics: Repetitive Behavior Scale-revised (RBS-R) and Screen for Child Anxiety-Related Emotional Disorders (SCARED) category means.
Descriptive Statistics: Repetitive Behavior Scale-Revised (RBS-R) and Screen for Child Anxiety-Related Emotional Disorders (SCARED)
Friedman tests indicated a significant difference and medium effect size in total RBS-R between the three times (Table 3). Specifically, the Wilcoxon signed-rank tests showed a significant difference and medium effect size based on positive ranks between T1 and T2 (Z = −3.336, p = 0.001, r = −0.440) and between T1 and T3 (Z = −3.323, p = 0.001, r = −0.438). However, the comparison between T2 and T3 revealed no significant difference between the median ranks of positive and negative differences.
Differences in Repetitive Behavior Scale-Revised (RBS-R) and Screen for Child Anxiety-Related Emotional Disorders (SCARED) Outcomes: Means and p-Values of Friedman Test and Side Effect Outcome Measures
Further investigation of each participant trajectory suggested high interindividual variability in RRBI to a fixed ratio of CBD-rich treatment (see Fig. 2).
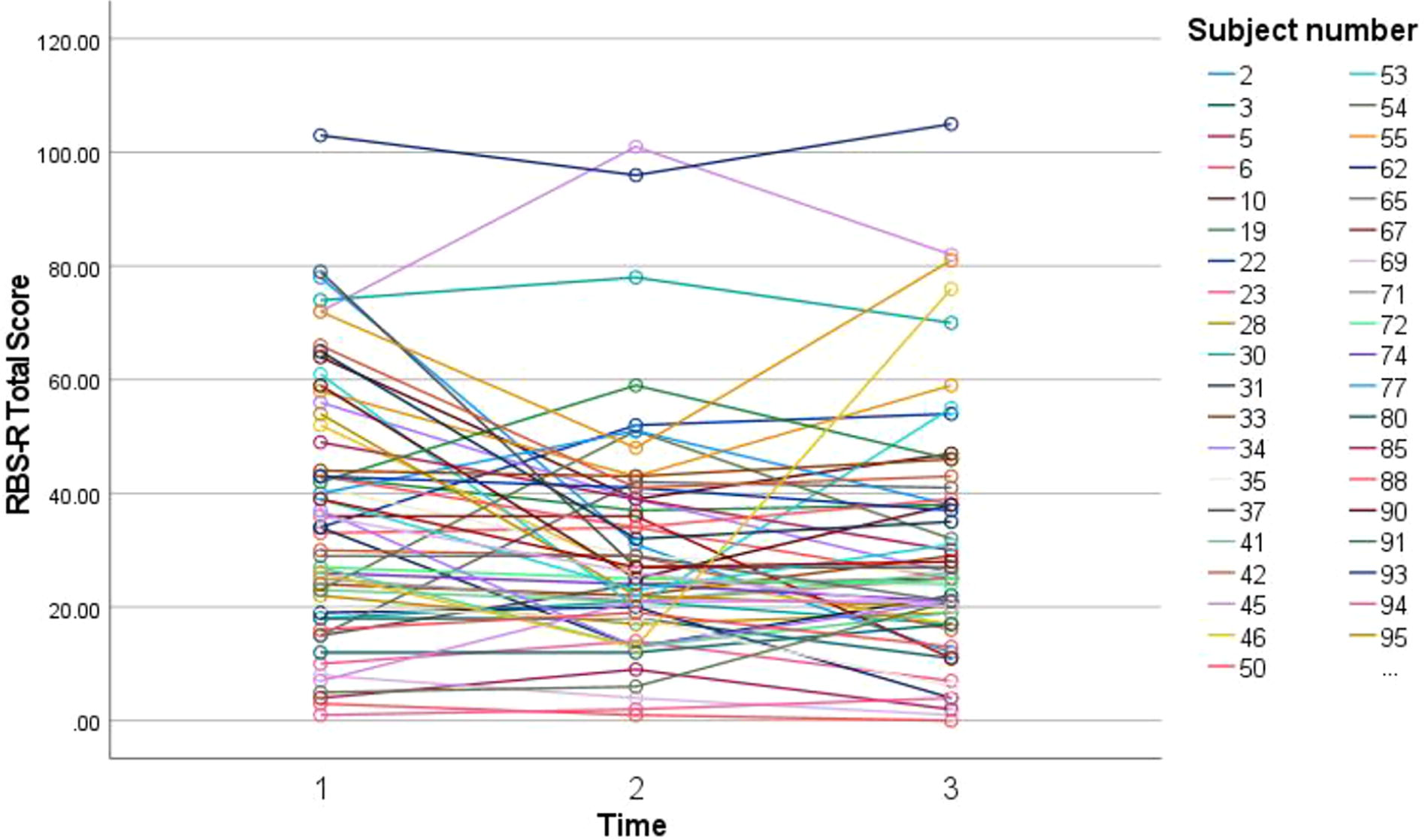
Trajectory of interindividual variability in restricted and repetitive behaviors and interests after cannabidiol-rich treatment.
A significant difference was found between the three times in three of the six RBS-R subscales (Table 3). Specifically, significant differences were found between T1 and T2 in compulsive (Z = −3.628; p = 0.001, r = 0.479), ritual (Z = −2.712, p = 0.007, r = 0.357), and sameness (Z = −2.452, p = 0.014, r = 0.323) behaviors and between T1 and T3 in compulsive (Z = −3.111; p = 0.002), ritual (Z = −3273, p = 0.001, r = 0.432), and sameness (Z = −2669, p = 0.008, r = 0.352) behaviors. However, there were no significant differences between the median ranks of positive and negative differences for the T2–T3 comparison.
Anxiety
Friedman tests showed a significant difference between the three times in total SCARED scores (Table 3), indicating decreased anxiety levels after cannabis treatment. Specifically, the Wilcoxon signed-rank tests showed significant differences and large effect sizes based on positive ranks between T1 and T2 (Z = −4.326, p = 0.001, r = 0.721) and between T1 and T3 (Z = −3.142, p = 0.002, r = 0.524). However, there was no significant difference between the median ranks of positive and negative differences for the T2–T3 comparison.
Friedman tests also indicated a significant difference between the three times in four of the five SCARED subscales (Table 3). Specifically, the Wilcoxon signed-rank tests showed significant differences based on positive ranks between T1 and T2 in panic (Z = −3.397, p = 0.001, r = 0.566), general (Z = −4.014, p = 0.001, r = 0.669), separation (Z = −3.308, p = 0.001, r = 0.551), and social (Z = −3.589, p = 0.001, r = 0.598) anxiety and between T1 and T3 in panic (Z = −2.546, p = 0.011, r = 0.424), general (Z = −2.616, p = 0.009, r = 0.436), separation (Z = −2.164, p = 0.031, r = 0.361), and social (Z = −2.658, p = 0.008, r = 0.443) anxiety. However, there was no significant difference between the median ranks of positive and negative differences for the T2–T3 comparison. Correction for multiple tests indicated a significant p-value of 0.008. After the corrections, except for sameness behavior, all differences were still significant. Further investigation of each participant trajectory suggested high interindividual variability in anxiety to a fixed ratio of CBD-rich treatment (see Fig. 3).

Trajectory of interindividual variability in anxiety after cannabidiol-rich treatment.
An examination of the relationship between anxiety and RRBI subtypes revealed that the total SCARED score was significantly positively related to sameness behaviors only, r(37) = 0.40, p = 0.02 (Fig. 4). Further investigation of the relationships demonstrated a positive correlation between panic anxiety and sameness behaviors, r(39) = 0.37, p = 0.01, and between separation anxiety and sameness behaviors, r(41) = 0.34, p = 0.02, after cannabis treatment.
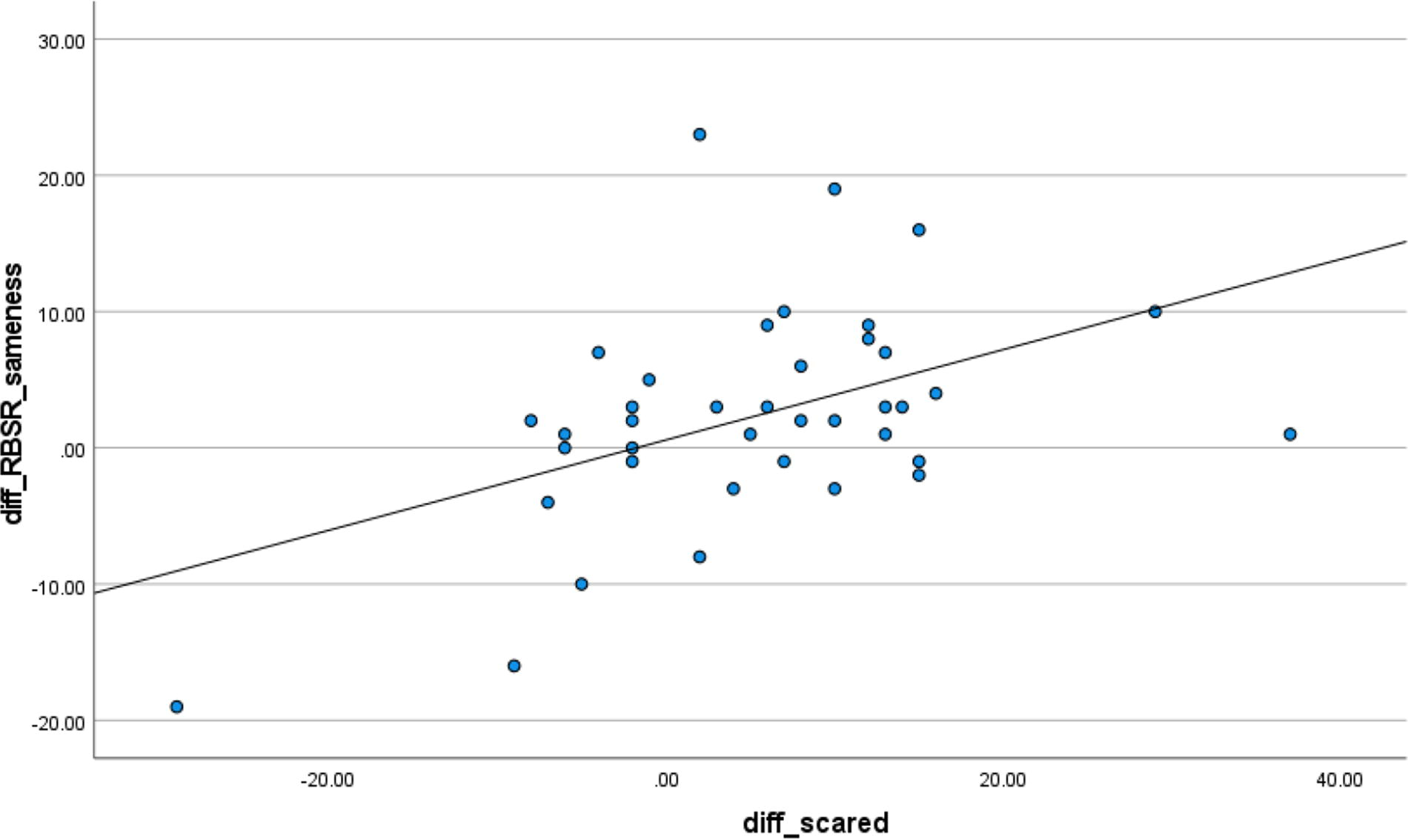
Relationship between anxiety in children measured by the Screen for Child Anxiety-Related Emotional Disorders (SCARED) and sameness-related recurrent behaviors according to the Repetitive Behavior Scale-revised (RBS-R).
A multiple regression analysis to examine whether the reductions in panic and separation anxieties explained the decrease in sameness-related behaviors revealed that those two variables predicted the reduction, F(2, 37) = 6.58, p = 0.004, explaining 26% of the variance in sameness behavior (R2 = 0.263, adjusted R2 = 0.223, SE = 6.973). However, only panic anxiety exhibited statistical significance (β = 0.466, p = 0.008). Based on multiple regression analysis using G*Power calculation, the achieved power was 0.91.
Discussion
This open-label study investigated the impact of CBD-rich cannabis treatment on autistic children’s anxiety subtypes and relationships to RRBI. It examined whether a change in anxiety symptoms predicted a change in RRBI after cannabis treatment. The results show reduced symptoms related to various anxiety subtypes and reduced RRBI in autistic children after cannabis treatment.
We found significantly reduced total SCARED scores, with specific improvements in general, panic, separation, and social anxiety severity. The literature indicates the contribution of cannabis treatment to reducing total anxiety for individuals with38,40,42,53 and without32–34 autism. Our results align with studies on animal models demonstrating the effectiveness of CBD-rich cannabis in reducing anxiety and stress.54,55 Particularly aligned with our results are recent systematic reviews reporting positive effects of cannabis treatment on general and social anxiety.56,57 Furthermore, Babayeva et al.’s 56 review presents preclinical data suggesting that CBD-rich cannabis treatment holds promise as a therapy for panic disorder.
In addition to changes in anxiety subtypes, our study presents changes in the children’s RRBI. Significant positive changes were observed in three of six RBS-R categories: compulsive, ritual, and sameness behaviors. These behaviors fall under the high-order RRBI classification. The literature indicates that most currently available ASD treatments aim to address mainly lower-order RRBI 58 that interfere with the individual’s function. 6 However, the literature suggests high-order RRBI may appear peculiar and age inappropriate. Thus, they could result in social stigma, 59 limit opportunities to develop flexible cognitive and social skills, 60 and significantly constrain social interactions. 61 Recent studies demonstrated the advantages of tailored behavioral intervention models to address high-order RRBI.59,62 Our study is the first to distinguish between low- and high-order RRBI in a medical cannabis intervention context and suggest it specifically benefits high-order RRBI.
The literature well documents the co-occurrence and relationship between anxiety and RRBI symptoms in ASD.7,21,63–65 Our results indicate a significant positive correlation between overall anxiety and RRBI, specifically insistence on sameness. These findings align with prior studies64,66 suggesting that insistence-on-sameness behaviors can be a strategy for managing anxiety because they involve an attempt to control one’s environment. Uljarević and colleagues 7 added to this meaningful relationship the idea of interplay between anxiety and delayed self-regulation and its significant role in maintaining insistence-on-sameness behaviors in individuals with ASD. The common neurobiological mechanisms that anxiety and RRBI may share are another possible explanation for this correlation. 21 Medical findings that antianxiety medications also reduce RRBI 67 support this concept. The suggested meaningful relationship between these variables emphasizes the importance of seeking treatments that can effectively target both conditions.
Our second goal was to elaborate on the relationship between anxiety and RRBI symptoms in the CBD-rich cannabis treatment context and explore whether changes in anxiety predict changes in RRBI after this treatment. Our results suggest that reduced panic and separation-related anxiety subtypes predict a decrease in RRBI, specifically sameness behaviors. In our study, panic anxiety exhibited statistical significance, explaining 26% of the variance in sameness behavior. These results elaborate on the associations previously found between panic anxiety and increased RRBI 68 and between insistence-on-sameness and separation anxiety. 66
Although we observed significant improvements in anxiety and RRBI after 3 months (T2) and 6 months (T3) of CBD-rich cannabis treatment, this improvement did not reach statistical significance between the 3rd (T2) and 6th month (T3) treatment points.
These findings suggest the possibility of a ceiling effect in the child’s anxiety and RRBI improvements after cannabis treatment. Another possible explanation is that these results reflect a placebo effect driven by parents’ hope for a promising new treatment. As identified in our recently published study, 46 such hopes and unrealistic parental expectations pose adherence challenges for this treatment. Our results in that adherence study highlighted that this treatment was not free of barriers, emphasizing the importance of providing professional guidance and knowledge to parents of autistic children on the impact of CBD-rich cannabis treatment for their children. Moreover, our results regarding each participant trajectory suggested high interindividual variability in both anxiety and RRBI to a fixed ratio of CBD-rich treatment.
This variability underscores the complex and individualized nature of how CBD affects anxiety and RRBI levels, suggesting that factors such as underlying biological differences could significantly influence treatment outcomes. Understanding these individual differences is crucial for tailoring CBD-rich treatment effectively for anxiety and RRBI management.
The cannabis dosage was indeed customized for each participant in the current study, resulting in a varied dosage schedule. Although this individualized approach offers flexibility tailored to the participants’ and their families’ needs, it limits accurately monitoring the effects of different dosages and schedules and their associations with efficacy.
Lastly, we implemented an open-label approach. The literature mentions this method as enhancing generalizability, reflecting usual—but less complex and costly—clinical practice, and allowing more patient recruitment and potentially better trial results. 69 Notably, however, our open-label study did not control for the placebo effect, necessitating caution in its interpretation. We strongly recommend future double-blind, placebo-controlled studies using standardized assessments to validate these findings. Moreover, we recommend additional longitudinal studies to investigate whether changes in children’s anxiety and RRBI are sustained over the long term (i.e., years of treatment) and persist once treatment ends.
Conclusion
Our study suggests positive implications for CBD-rich cannabis treatment in alleviating anxiety and RRBI symptoms in autistic children. The findings reveal that reduced anxiety, particularly within the panic- and separation-related subtypes, predicts decreased RRBI sameness behaviors. These results highlight the compelling evidence for the meaningful relationship between these variables and the potential benefits of medical cannabis treatment for autistic children and encourage further double-blind, placebo-controlled studies to determine the efficacy of CBD-rich cannabis treatment.
Footnotes
Acknowledgments
The authors thank all participants who contributed to this research, the research team at Shamir Medical Center, Israel and Nitzan Spectrum®, Seach Medical Group, Israel for providing the medicinal cannabis without cost.
Authors’ Contributions
A.D.: Conceptualization, methodology, data curation, writing—original draft preparation, formal analysis. O.S.: Conceptualization, methodology, formal analysis, Resources, writing—review & editing, supervision, project administration. M.B.: Resources, data curation, software. E.K.: Resources, data curation, software. A.H.: Resources, data curation, project administration. D.W.: Data curation, project administration. E.G.: Conceptualization, methodology, formal analysis, writing—review & editing, supervision. All authors have read and agreed to the published version of the article.
Statement of Ethics
Ethical approval was obtained from the Institutional Review Board of the University of Haifa (no. 274/21) and the Shamir Medical Center Helsinki committee (ASF-0056-21).
Author Disclosure Statement
No conflict of interest was reported by any of the authors.
Funding Information
No funding was received for conducting this study.