
Abstract
Abstract
Background:
Evidence indicates obese children have increased health care utilization. It is unknown if this is true within the emergency department (ED) setting. Our purpose is to determine if overweight children presenting for emergency care have increased resource utilization over normal weight peers.
Methods:
We conducted a retrospective cohort study of children 2 to <18 years old presenting to a pediatric ED in 2007. Overweight was defined as >95th percentile sex-specific weight-for-age, and normal weight was defined as ≤95th percentile. We used a subsample validation to compare these study definitions to BMI-based definitions. We compared total billed charges and secondary outcomes of ED length of stay and admission rate using multivariate and logistic regression models. Outcomes were reported for admitted and discharged patients. Four diagnoses were examined for primary and secondary outcomes.
Results:
Of 32,996 included visits, 6333 (19.2%) were for overweight children. Study definitions correctly classified 98.3% of normal weight children but only 51.3% of overweight children. Overweight children were more likely to be older, black, and publicly insured. Median charges for overweight and normal weight children, whether discharged or admitted, were not different in the adjusted model. Admitted overweight children with asthma and fractures or dislocations had higher median charges than normal weight $4617 (2065–375,669) versus $4177 (1980–37,432, p=0.01) and $9855 (6681–58,546) versus $8137 (1461–52,557, p=0.01), respectively.
Conclusions:
Overall acute care costs for overweight children are not different from normal weight children. However, admitted overweight children have disease-specific increased use of resources.
Introduction
Although the increase in health care spending associated with obesity has been clearly documented in adult patients, there are fewer studies evaluating the direct cost of obesity in children.6,7 Overweight children may place an increased burden on our healthcare system as evidenced by increased admissions for obesity-related diagnoses, lengthened hospital stays, increased hospital admissions for certain diagnoses, and increased hospital costs.8–11 Acute care, emergency department (ED) visits, and unplanned hospitalizations are expensive methods of care. 12 If overweight and obese children have increased acute care costs, this could place a significant burden on the healthcare system. To our knowledge, no study has evaluated the difference between overweight and normal weight children at presentation to the ED and compared their ED, hospital-billed charges, and ED lengths of stay. The purpose of this study is to compare overweight children presenting to the ED to their normal weight counterparts with respect to billed charges, clinical presentation, admission rates, and ED lengths of stay.
Methods
Study Design, Population, and Setting
We conducted a retrospective study of all visits for children 2 to <18 years of age who presented in 2007 to the ED at St. Louis Children's Hospital. St. Louis Children's Hospital is a free-standing, academic children's hospital with level-one trauma capabilities.
Study Sample
Visits for children with missing, estimated, or implausible weight data were excluded. We determined weights to be estimated if the weight was noted to be per parents report or if units other than kilograms were recorded. Implausible weights were defined as greater than 275 kilograms; this was physiologically improbable and likely represented a typographical error in the medical record. Visits were excluded for children with weight-for-age less than the 3rd percentile; these children were likely malnourished and/or chronically ill children. Pregnancy test results were obtained from the hospital laboratory, and, if a positive result was obtained for that visit, the patient visit was excluded. Visits were also excluded for hospital charges of $0 and those greater than $1 million, which represent care for a truly catastrophic event. Finally, visits were excluded if the child's disposition data were missing and thus it was unknown if the patient was admitted to the hospital or discharged home.
Comparison Groups
Given the lack of retrospective height data, overweight was defined as greater than the 95th percentile sex-specific weight-for-age. 13 Normal weight was defined as less than or equal to the 95th percentile sex-specific weight-for-age.8,9,14
Data Sources
Data were extracted from four electronic databases: The electronic medical record for the ED visit; the electronic medical record for the hospital admission; the billing database for charges, discharge diagnosis, and insurance status; and the laboratory database for pregnancy test results. We used patient account number, a unique identifier for each patient visit, to match data. The Human Resource Protection Office at Washington University approved this study, and a waiver of informed consent was obtained for the study.
Data Collection
To validate our study definitions for normal weight and overweight children, a subsample of 400 normal weight children and 100 overweight children as defined by the study definition were randomly selected from children who were admitted to the hospital. Admitted children had a height and weight recorded on arrival to the inpatient unit, which was obtained from their electronic hospital medical record. Patients were excluded from this subset if they did not have both a height and weight recorded. A BMI was calculated for each of these patients, which was then classified as normal weight by BMI-for-age below the 85th percentile, or overweight by BMI-for-age at or above the 85th percentile. 15 Percentiles for BMI-for-age were obtained using the CDC SAS program. 13 Patients with biologically implausible values were excluded. 13 Percent agreement between the study definition and the CDC definition for normal weight and overweight was calculated for the subsample.
To characterize visits by overweight and normal weight children within our cohort, we collected demographic data, including age, race, insurance status, mode of arrival, identifiable primary care physician, and internal triage acuity. Race was classified into white, black, or other. Insurance information was obtained from the medical billing database. The billing database contained the insurance company's financial class, which was further classified into public, private, or uninsured by consensus agreement between two of the authors (K.F.D., J.L.). Mode of arrival was classified into arrival by emergency medical service (EMS) or not by EMS. Patients were listed as having an identifiable primary care physician if they identified one during their visit. Triage level for the St. Louis Children's ED is assigned on an internally validated five-point scale with 1 as the highest acuity level and 5 as the lowest acuity level.
The primary outcome was billed charges for the child's visit, as a proxy for cost. 10 ED charges were rolled into hospital charges; thus, billed charges as well as other outcomes were reported separately for patients discharged from the ED and those admitted to the hospital. Secondary outcomes were hospitalization rate and ED length of stay in hours. Length of stay was determined by computerized time stamps from triage to discharge or transfer to the inpatient unit. Patients with negative lengths of stay or lengths of stay greater than 24 hours were excluded from the length of stay analysis, because these values are improbable and likely represent errors in the medical record.
The primary and secondary outcomes were analyzed for the entire cohort and for four disease specific subgroups. Discharge diagnosis was obtained from International Classification of Disease, 9th Revision (ICD-9), codes in billing data, because these codes are assigned by professional coders in response to the physician's diagnosis. ICD-9 codes were grouped into related diagnostic groups and subgroups using the Diagnosis Grouping System (DGS). 16 Four DGS subgroups were chosen that were prevalent in both discharged and admitted patients and represented common pediatric problems. The four subgroups were compared for mean charges per visit, length of stay, and admission rate.
Sample Size
Using an estimated mean cost of $750 and standard deviation of $250 in obese children, the sample size of 176 for each group was calculated to achieve 80% power to detect a 10% difference in charges between obese children and normal weight children with a significance level of 0.05 and a two-tailed t-test.
Data Analysis
Ninety-five percent confidence intervals (CI) were determined for subsample validation by the exact binomial proportion test. The chi-squared, Student t-test, and Wilcoxon test were used to detect the cohort characteristics' significance. Multivariate regression modeling was used to detect confounders for the primary and secondary outcomes. Race, age, sex, insurance, and acuity were identified as potential confounders and were controlled in the multivariate regression model that was used to compare the primary outcome. For the secondary outcomes, generalized linear modeling was used for the length of stay comparison with confounders controlled. Adjusting for the same confounders, logistic regression modeling was used to estimate the admission rate between the obese and normal weight group. Medians and ranges of charges, length of stay, and percentages of admission rates were reported, and descriptive analysis was used for the discharge diagnoses. Mean charges were also reported as a reflection of the total cost to society. Log transformation was performed for nonnormally distributed data. SAS versions 9.1 and 9.2 (SAS Institute Inc., Cary NC) were used for the analysis. The significance was considered at two-sided values, p<0.05.
Results
Study Sample
Of 55,352 patient visits to the ED in 2007, 32,996 were included in our study; exclusion criteria are shown in Figure 1. Of these, 6333 (19.2%) were for overweight children as classified by the study definition.
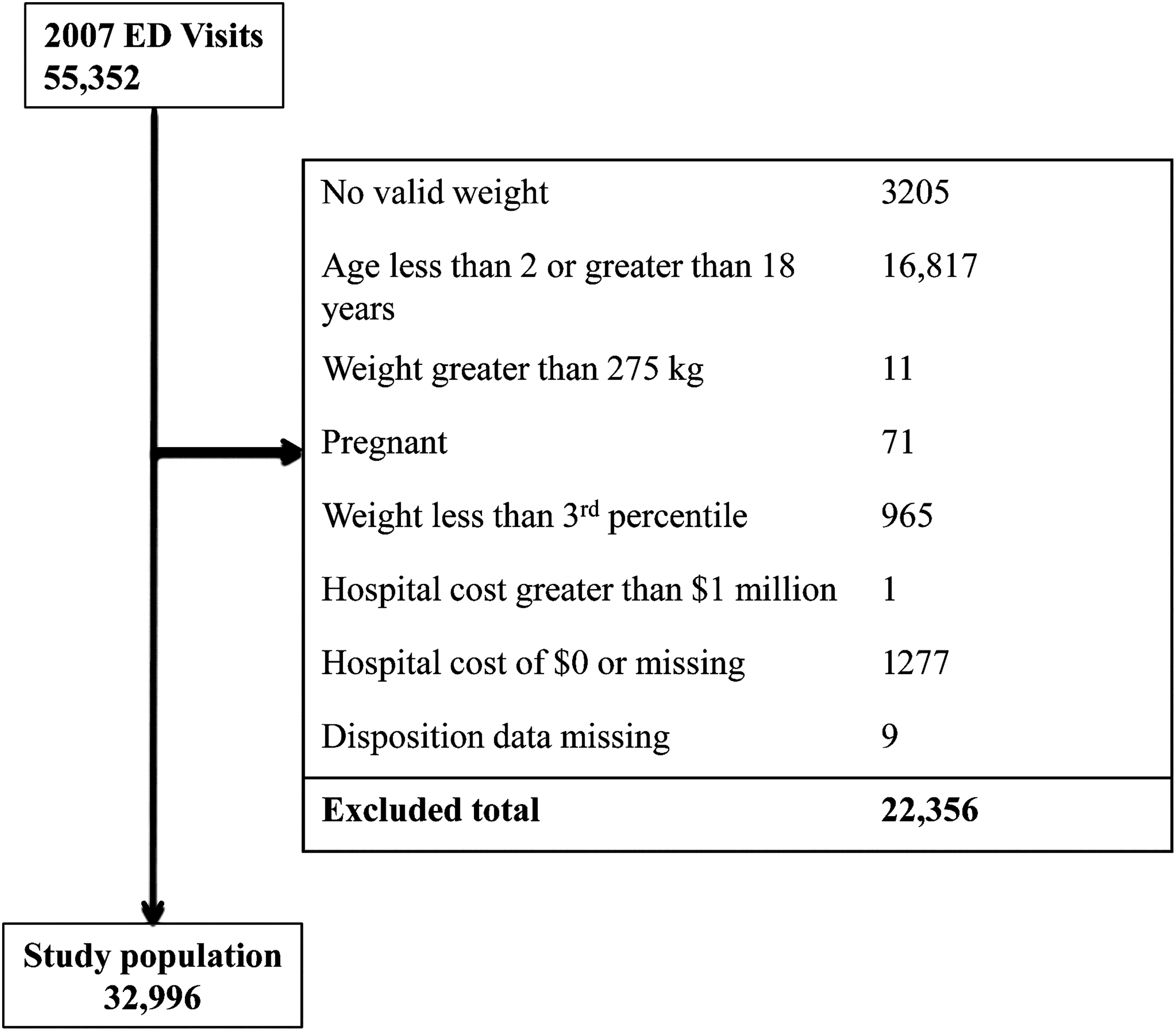
Exclusion criteria.
Subsample Validation
Table 1 displays the results of the subsample of admitted patients that were used to compare our study definition to the BMI-based definition of overweight and obese. Of the 400 children in the subsample who were normal weight by the study definition, 356 were eligible for analysis; and of the 100 children in the subsample who were overweight by study definition, 85 were eligible for analysis. Among those classified as normal weight by the CDC definition, 280 (98.3%) of 285 (CI 96.0–99.4%) met the study definition of normal weight. For those classified as overweight or obese by the CDC definition 80 (51.3%) of 156 (CI 43.1–59.3%) met the study definition of overweight. The overall percent agreement between the study definitions and the CDC definitions was 360 (81.6%) of 441 (CI 77.7–85.1%).
Comparison of Study and BMI-Based Definitions of Overweight
40 were excluded for missing data, 4 were excluded as outliers.
13 were excluded for missing data; 2 were excluded as outliers.
Exact binomial proportion.
CI, confidence interval.
Cohort Characteristics
Table 2 shows the characteristics of our study cohort stratified by disposition after their ED visit, admitted to the hospital versus discharged home. Compared to normal weight children, higher proportions of overweight children were older, black, and publicly insured in both the admitted and discharged groups. However, there were no differences in arrival by EMS or identification of a primary care physician among normal weight and overweight children in either admitted or discharged groups. Discharged patients who were overweight were more likely to be female, but this was not true of admitted patients. Admitted patients who were overweight had a lower mean acuity on presentation.
Characteristics of the Cohort at Presentation by Weight and Admission Status
p<0.001.
p=0.002.
p=0.04.
Acuity was missing for one normal weight, discharged patient visit.
CI, confidence interval; EMS, emergency medical service; PMD, primary medical doctor.
Table 3 presents the admission rates for normal weight and overweight children. Overweight and normal weight children did not have different rates of admission to the hospital after controlling for potential confounders. The four high-frequency DGS subgroups chosen were: Abdominal pain; asthma; fractures and dislocations of extremities; and infectious skin, dermatologic, and soft tissue diseases. These subgroups represent the four most common diagnosis groupings shared between the comparison groups. No significant differences in admission rates between overweight and normal weight visits were found for these subgroups.
Admission Rate by Weight, for Patients Admitted and Discharged by Diagnosis
Median and Mean Charges
Median charges and ranges are shown for all visits and by DGS subgroup in Table 4. Charge data was nonnormally distributed. Comparing original and log transformation, parametrics of skewness and kurtosis were close and the p value of the normality test before and after log transformation was the same; therefore, the original data are presented in the table for ease of interpretation. Among all children admitted to the hospital or those discharged from the ED, there was no difference in charges between normal weight and overweight after controlling for potential confounders. In children admitted for asthma, there was a significant difference in charges; overweight children had significantly higher charges compared to their normal weight counterparts, median $4617, range 2065–375,669 (mean $9016) versus, median $4177, range 1980–37,432 (mean $5320), p=0.01. There was no difference by weight among discharged children with asthma. A similar trend was seen in fractures and dislocations; visits resulting in admission for overweight children had median charges of $9855, range 6681–58,546 (mean $13,250) compared to normal weight children who had median charges of $8137, range 1461–52,557 (mean $9952), p=0.01. Again, there was no difference between normal weight and overweight children with fractures and dislocations who were discharged from the ED. In children with abdominal pain and with soft tissue infections, there were no differences in charges between overweight and normal weight children.
Median Charges for Admitted and Discharged Patients, by Diagnosis
p<0.05 in multivariate regression modeling.
Sex and race were not potential confounders in the multivariate regression modeling.
ED Length of Stay
ED lengths of stay are shown for all visits and by DGS subgroup in Table 5. Overweight and normal weight children had no difference in ED length of stay, after controlling for potential confounders, whether admitted or discharged. In the DGS subgroups, there were no differences in ED length of stay for overweight versus normal weight children.
Emergency Department Length of Stay in Hours for Admitted and Discharged Patients by Diagnosis
No potential confounders identified in the multivariate regression modeling.
Sex and race were not potential confounders in multivariate regression modeling.
Subjects with negative lengths of stay or length of stay greater than 24 hours excluded.
Discussion
In this study, we found no measurable difference in overall acute care charges for overweight children discharged from the ED or admitted to the hospital. However, there were important disease-specific increases in cost of care for overweight children that were admitted to the hospital after ED evaluation. In particular, overweight children admitted to the hospital for asthma and fractures or dislocations had substantially higher costs of care. Additionally, in this study, overweight children were more likely to be older, black, and publicly insured.
Weight-for-age greater than the 95th percentile has been used as a proxy definition for overweight in settings where height was not routinely collected.8,9,14,17 Unlike these prior studies, we used a subsample validation scheme to compare weight-for-age to the gold standard definition in this cohort. Our study definition of overweight correctly identified most normal weight children (98.3%), but had a comparatively lower correct identification of overweight and obese children (51.3%). A comparatively higher rate of misclassifying overweight and obese children as normal weight will likely bias the study toward accepting the null hypothesis, i.e., the effects of overweight and obesity in the study may be underestimated. Future investigators who use weight-for-age to define weight status need to take into account the underestimation of the effect of obesity.
The cohort in this study was not representative of national demographics, with a higher proportion of publicly insured patients (59% in this cohort vs. 30% of children nationally), and a higher proportion of black patients (65% in this cohort vs. 15% nationally). 18 However, our sample is similar to that of other urban, academic pediatric institutions. 10 In this study, overweight children on presentation to the ED are more likely to be older, black, and publicly insured. Other studies have shown that black children are more likely to be overweight or obese,1,3,10,14 and at least one study had a higher proportion of children with Medicaid (public insurance) who were overweight. 10 These findings suggest that it may be necessary to intervene at a young age to prevent obesity and to develop obesity prevention programs that target particular sociodemographic groups.
Childhood obesity clearly leads to long-term consequences that increase healthcare costs.4–6 Cost–benefit analyses suggest that spending $2 billion per year in obesity prevention would be cost effective if it reduced obesity among 12 year olds by one percentage point. 19 The question remains, however, who should be responsible for funding childhood obesity programs. Motivating health insurers to willingly invest in obesity prevention requires evidence of more immediate cost savings. There is some evidence that childhood obesity increases short-term healthcare costs. Previous investigators used the Medical Expenditure Panel Survey to show excess annual-per-child attributable healthcare costs for overweight and obese children with particular increases in annual costs for prescription drugs, outpatient visits, and ED visits.6,20 Similarly, a study among Medicaid patients found that overweight children had higher outpatient and acute care expenditures, whereas a study among children who received primary care at an urban children's hospital found overall annual charges for all types of healthcare services were increased for overweight children.10,21 In contrast, analysis of the National Health and Nutrition Examination Survey and Medical Expenditure Panel Survey data found that while overweight children have increased dyslipidemia, hyperglycemia, and hypertension, overall they do not have increased healthcare expenditures. 22 Our study did not find a difference in overall acute care resources for overweight children when discharged from the ED or when admitted to the hospital. However, caution should be taken when interpreting this finding, because our study was biased to the null hypothesis.
Our study supports prior research that indicates increased disease-specific resource use among overweight children.8,9,14,17,23–28 Asthma symptoms and exacerbations have an association with obesity, but the mechanism is unclear.23,25 In our study, overweight children with asthma who were admitted to the hospital had significantly higher billed charges than their normal weight peers; however, there was no difference in billed charges for children discharged from the ED. Prior studies are conflicting as to whether obesity leads to longer lengths of stay or increased admission rates for asthma.8,9,27 There were no differences in ED length of stay or admission rate for overweight children with asthma in our cohort.
The same pattern emerged for children with fractures and dislocations of extremities. Overweight children admitted for long bone injuries had significantly higher charges, but there were no differences in our outcomes among discharged patients. Prior studies indicate that obese children appear to have different patterns of injury than nonobese children and more complicated hospital courses after injuries, which may account for the disparate charges.14,24,26 Examining disease-specific and severity-dependent differences in healthcare use and expenditures between overweight or obese children and normal weight children is a very important method of comparison for acute care. Overall cost comparisons in hospital and ED settings may be confounded by children with chronic illnesses, such as cancer or neurologic conditions, who are more likely to be underweight or normal weight than overweight. In addition, evaluating patients admitted to the hospital from the ED separately from those that are discharged home demonstrates that the cost differences may be related to severity of illness. In other words, for those children with less severe asthma exacerbations and long-bone injuries, overweight and normal patients receive similar levels of care. However, for more severe disease, those that require admission, overweight patients have higher costs and perhaps more complicated courses. Furthermore, this study does not assess the important question of whether or not overweight children utilize the emergency department more frequently.
Our study had several limitations. The study definition of overweight used weight-for-age instead of BMI; this resulted in a number of overweight children being classified as normal weight, thus biasing our results to the null hypothesis. Also, by excluding patients with weight not obtained at the study facility, we may have excluded higher-acuity patients. Nonetheless, our study was able to demonstrate a significant difference in disease-specific acute care costs. We used billed charges as a proxy for cost. Billed charges are standardized for patients with a variety of different payer sources whereas collected fees can be very different, depending on third-party payers. There is precedence for using billed charges as a proxy for economic burden, but they overestimate burden as third-party payers often reimburse at discounted rates. 10 The study was overpowered, but we used an entire year of patient visits to obtain a broad, representative sample, to eliminate bias due to seasonal variation in pediatrics, and to allow us to investigate disease-specific subpopulations. Finally, this cohort comes from a single institution and may not be generalizable.
Conclusion
Although our study was unable to demonstrate an overall difference in acute care costs for overweight children, we were able to demonstrate a substantial increase in hospital charges for overweight children who are admitted through the ED with certain diagnoses, notably asthma and fractures and dislocations. Our findings support the growing body of literature demonstrating the economic burden of obesity. While the long-term health care savings incurred by preventing obesity are the most persuasive economic argument for prevention, our findings support the argument that immediate health care savings can be achieved by addressing obesity in childhood.
Footnotes
Acknowledgments
No external funding was required for this study.
Author Disclosure Statement
The authors have no conflicts of interest to disclose.