
Abstract
Abstract
Background:
Accurate early assessment and targeted intervention with problematic parent/child feeding dynamics is critical for the prevention and treatment of child obesity. The division of responsibility in feeding (sDOR), articulated by the Satter Feeding Dynamics Model (fdSatter), has been demonstrated clinically as an effective approach to reduce child feeding problems, including those leading to obesity. Lack of a tested instrument to examine adherence to fdSatter stimulated initial construction of the Satter Feeding Dynamics Inventory (fdSI). The aim of this project was to refine the item pool to establish translational validity, making the fdSI suitable for advanced psychometric analysis.
Methods:
Cognitive interviews (n=80) with caregivers of varied socioeconomic strata informed revisions that demonstrated face and content validity. fdSI responses were mapped to interviews using an iterative, multi-phase thematic approach to provide an instrument ready for construct validation.
Results:
fdSI development required five interview phases over 32 months: Foundational; Refinement; Transitional; Assurance; and Launching. Each phase was associated with item reduction and revision. Thirteen items were removed from the 38-item Foundational phase and seven were revised in the Refinement phase. Revisions, deletions, and additions prompted by Transitional and Assurance phase interviews resulted in the 15-item Launching phase fdSI. Only one Foundational phase item was carried through all development phases, emphasizing the need to test for item comprehension and interpretation before psychometric analyses.
Conclusions:
Psychometric studies of item pools without encrypted meanings will facilitate progress toward a tool that accurately detects adherence to sDOR. Ability to measure sDOR will facilitate focus on feeding behaviors associated with reduced risk of childhood obesity.
Introduction
Accurate assessment and targeted intervention of early problems with parent feeding behaviors is critical for prevention and treatment of child obesity. Qualitative, longitudinal, cross-sectional, and literature review studies support links among parental feeding behaviors, child eating behaviors, and child weight status.1–4 Negative child behavioral patterns, including disruptive mealtime behavior and extreme food selectivity, contribute to child obesity.5,6 In a longitudinal study, increased parental concern about childhood obesity and increased incidence of toddler feeding problems correlated with obesity at age 9 years. 7 In a 1-year study of 323 parent-child dyads, feeding the child to assuage emotional arousal, overt food restriction, and fat restriction were prospectively associated with obesigenic child behaviors. 3 A cross-sectional study of almost 5000 4 year olds revealed that higher mean child BMI was associated with more child food responsiveness, enjoyment of food, and parental restriction. 2 A literature review of 31 articles from high-income countries revealed that during infancy, high maternal control and low sensitivity correlated with higher weight gain. 4 Conversely, controlling and indulgent feeding patterns were associated with lower weight gain. With respect to toddlers and preschoolers, 15 of 20 studies found positive relationships between feeding (controlling, restrictive, and indulgent) and child weight status, and five found negative associations between parental pressuring and child BMI. Five of seven articles from the preschool/early elementary period found positive correlations between feeding (restrictive or indulgent) and child weight status and two found negative relationships between pressuring during feeding and child BMI. 4 These child feeding problems correlate with parental eating problems. 8
The Satter Feeding Dynamics Model (fdSatter) has been offered as a model to prevent or correct obesigenic parental (primary caregiver) feeding practices. 9 fdSatter defines and addresses parental feeding practices that support the child's competence with respect to eating attitudes and behaviors. fdSatter systematizes research-based evidence and conceptualizes the feeding of young children as a relational, multi-systemic process with parents as the architects of feeding.10,11
fdSatter provides the theoretical framework for Satter's Division of Responsibility in Feeding (sDOR) between caregivers and children: Parents do the what, when, and where of feeding and children do the how much and whether of eating. 12 According to Satter, “Children have a powerful and resilient ability to maintain energy balance and grow in a predictable fashion. However, for the child to maintain appropriate energy intake, the feeding relationship must be responsive and supportive.” 11 sDOR posits that optimal feeding depends on caregivers who both provide leadership with feeding and give the child autonomy with eating. That is, parents take responsibility for food management and provide the structure and social context for feeding and thereby ensure a positive feeding environment. At the same time, parents are trusting of, and responsive to, the child's capabilities with respect to food acceptance, food regulation, and growth.9,11–13 The priority with sDOR is consistent feeding, with parents keeping control of the family food supply and of the menus for meals and snacks. 13 At the same time, parents do not attempt to impose control on what or how much the child eats, either overtly or covertly. 14 Once the food and the context are provided by the parent for the meal or snack, the parent trusts the child to manage his or her own food consumption.9–13
As such, sDOR is an authoritative approach to feeding: Parents taking leadership with feeding embodies parental expectations for the child's self-mastery; and parents' giving the child autonomy with eating enacts parental sensitivity. 11 That is, parents who give autonomy let the child be independent and self-directing within the context that they provide and, at the same time, remain warm and attentive to the child. Leadership without autonomy is authoritarian feeding, and autonomy without leadership is indulgent feeding; neither feeding style is congruent with sDOR. The principles of sDOR are recognized as the best practice childhood feeding model and incorporated in recommendations by the Academy of Nutrition and Dietetics,15,16 the American Academy of Pediatrics,17,18 and child obesity guidelines. 19 Feeding in Head Start is conducted in accordance with sDOR principles. 20 The principles of sDOR form the basis for Special Supplemental Nutrition Program for Women, Infants, and Children (WIC) certification based on inappropriate feeding practices 21 and provide the foundation for related core messages developed by the USDA Food and Nutrition Service. 22
Despite its wide availability and application, a validated tool to measure adherence to sDOR has not been developed. A variety of tools with varying levels of reliability and validity are available 23 ; however, those tools are based on varied theoretical constructs and protocols for intervention. These tools, for instance, address parents' perceptions of children's eating attitudes and behaviors, 24 parental concerns about the child's eating and other behavioral issues, 25 the child's neophobia, 26 or fdSatter-inconsistent definitions of parent demandingness and responsiveness in feeding. 27 Framing a test that can examine the theoretical underpinnings and application of sDOR is not meant to displace the aforementioned constructs and protocols, but rather to contribute to the parent feeding behavior dialog in the language of fdSatter. Given the cross-disciplinary usage of sDOR, such a tool needs to be sufficiently accessible to be used in a variety of practice settings (e.g., Head Start and doctors' offices) and sufficiently robust for rigorous psychometric testing. To address the need for a validated, objective assessment of sDOR, 13 Satter drew from clinical observations and professional literature to generate the Satter Feeding Dynamics Inventory (fdSI) as a self-report questionnaire to be completed by parents of children ages 2 through 5 years.
A shared understanding of meaning, especially among diverse audiences, is essential for development of weight-related interventions. 28 Likewise, a major challenge for development and construct validation of instruments is to develop items that elicit a shared understanding of meaning. That is, the test must have translational validity (i.e., that operationalization of items is a good reflection of the construct), especially among more diverse audiences. Mismatch in item meaning between what is intended and what is comprehended can contribute to ambiguous relationships between maternal feeding practices and changes in child overweight. 29 Dissonance between a construct (i.e., developer-held belief or perspective) and test item interpretation can be detected with cognitive interviews during survey development. 30 Respondents score an item, then are asked to explain responses, paraphrase items, discuss thoughts, feelings, and ideas, or suggest other wording. Items that show consonance can stand as written; those that show dissonance must be discarded or revised. Iterative mapping of item responses to interview verbalizations aligns construction of a survey qualified for construct validation.
The aim of this project was to rigorously examine the fdSI item pool using an iterative response mapping process to refine the initial items and assure face and content validity (i.e., parents and testers mutually understand and interpret all items) preceding further studies to establish construct validity.
Methods
Study Design
This formative assessment stage of fdSI construction examined face and content validity in five researcher defined and labeled phases: Foundational; Refinement; Transitional; Assurance; and Launching. Each phase utilized a mixed-method approach with similar data collection and analyses procedures that resulted in item revision, deletion, and/or addition (see Figs. 1 and 2). A description of procedures common to all phases is followed by phase-specific details.
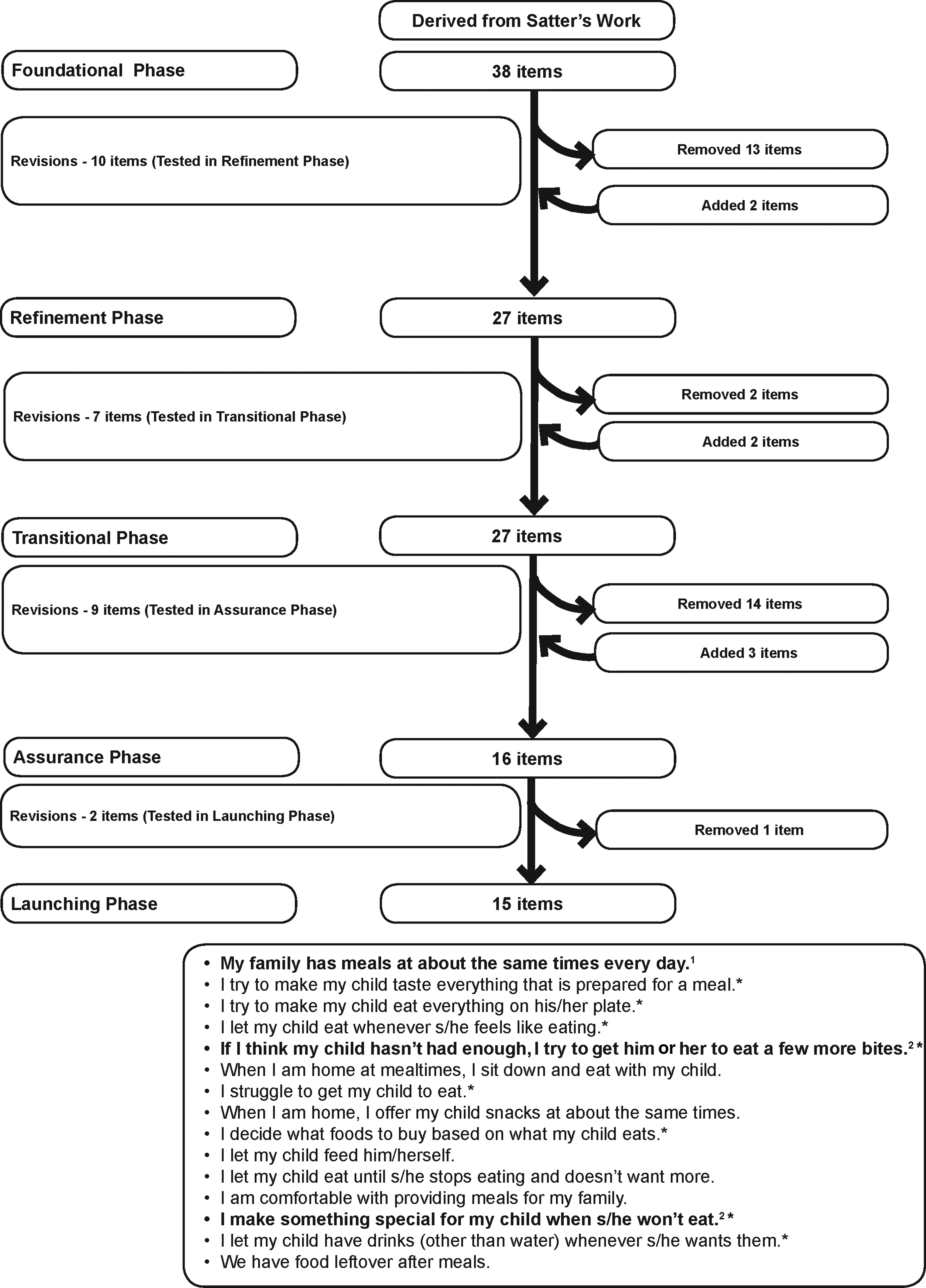
Evolution of survey items. This figure shows the evolution of survey items throughout the five developmental phases. Items from the Launching phase are listed in the order that they appear on the survey. 1Item was carried through from the Foundational phase. 2Item was carried through from the Refinement phase. *Item is reverse scored.

Phases of Satter Feeding Dynamics Inventory item development.
Each phase measured eating competence with the validated31,32 and reliability-tested 33 ecSatter Inventory for Low-Income audiences (ecSI/LI). Response options for the 16 items included always, often, sometimes, rarely, and never; scored as 3, 2, 1, 0, and 0, respectively. Responses are summed so that scores can range from 0 to 48. Based on researcher clinical expertise, confirmed by subsequent validation studies, eating competence was defined as a score greater than or equal to 32.31,32 For all fdSI item development phases, item response options were always, often, sometimes, rarely, and never. Additional survey items captured participant age, child age, race/ethnicity, federal assistance program usage, and educational level. Items were written at a fourth-grade reading level or less.
Cognitive interviews were conducted by trained interviewers in each phase to identify and revise items that did not convey their intended meaning.34,35 Cognitive interviews were used because the one-on-one interview for at least 30 minutes enables development of a rich data set quite distinct from a quantitative survey. Each phase utilized the version based on findings from the preceding formative phase. Cognitive interviews followed procedures outlined by Willis 34 and Shafer and Lohse 30 and used retrospective verbal probing techniques. Subjects read each of the fdSI items aloud (in the same order), verbalized their chosen response (always, often, sometimes, rarely, or never), and described their rationale for choosing the response option. Interviewer probes, designed by an expert panel, elicited more-specific information to clarify response choice for each item and enabled the interviewer to determine whether the subject interpreted the item as intended or was triggered to provide a tangential response. The Pennsylvania State University Institutional Review Board (University Park, PA) approved this study, and verbal informed consent was obtained from all participants.
Statistical Analyses
Cognitive interviews were analyzed iteratively using a thematic approach. 34 Interview notes and audio recordings were reviewed by the interviewer and fdSatter-oriented researchers not present during the interview. Patterns in respondent interpretation and processing of each fdSI item were identified using a constant comparative method. 36 Interview responses for each item across respondents were mapped to fdSI responses to examine consistency and comprehension. This response mapping technique enabled calibration of discrepancies and congruencies for each fdSI item. Items consistently comprehended as intended remained the same; items interpreted as not intended were revised or removed. At each item development phase, the overall content of fdSI was evaluated to assure that the questionnaire examined key elements of fdSatter and preserved a balance between items addressing parent leadership and those addressing child autonomy. fdSI face validity was assessed through rigorous review of cognitive interview transcripts.
Subsequent to, and including, the Transitional phase, fdSI item responses were arithmetically summed; scores for each of the items ranged from 0 to 4; total possible scores differed, depending on survey development phase. Scores ranged from 0 to 108, 0 to 64, and 0 to 60 for the Transitional, Assurance, and Launching phases, respectively. Internal consistency of responses from the 27-item surveys completed in the Transitional phase was assessed with Cronbach's alpha. Data were analyzed using SPSS statistical software (version 19; IBM, Armonk, NY).
Results
Foundational Phase
fdSI originated as a 14-item clinical tool titled, Feeding Your Child (FYC). FYC was used for clinical assessment of parent-child feeding dynamics in conjunction with parental interviews and observations. In addition, it was used for awareness training and education with respect to parent-child feeding interactions. FYC was refined through repeated usage and revision by clinicians expert with feeding dynamics and proved useful with respect to identifying specific distortions in feeding dynamics and targeting interventions. However, unpublished reliability testing revealed FYC to have a single factor and suboptimal internal reliability. These psychometric concerns prompted transformation of FYC to fdSI, a 38-item instrument with 20 parent leadership and 18 child autonomy items; items were classified based on the operational definitions of parent leadership and child autonomy. Parent leadership was defined as parent attitudes/behaviors related to their taking responsibility for the what, when, and where of feeding. Child autonomy was defined as parent attitudes/behaviors that support or interfere with the child's prerogative with respect to determining how much or whether to eat. Item generation was driven by an evidence- and experience-based conceptualization of optimal, developmental stage-appropriate parental feeding dynamics, as defined by fdSatter.9–13 Content validity was established by item review by a panel of experts in feeding dynamics and human development. Response options to the 38-item survey were almost always, often, sometimes, rarely, and almost never.
Subsequent to survey completion, two rounds of cognitive interviews were completed with low-income caregivers in Pennsylvania. Round 1 consisted of 4 low-income women completing both the fdSI and a cognitive interview. Each participant responded to half of the survey: questions 1–19 or 20–38. Participants voiced confusion distinguishing between almost always and often, as well as almost never and rarely. In addition, some participants noted not knowing how to respond when they “always” or “never” did some behaviors. Therefore, almost always and almost never were revised to always and never, respectively. As a result, fdSI response options became always, often, sometimes, rarely, and never. Some items were revised slightly to present negative behaviors in the affirmative to encourage parents to accurately report socially undesirable behaviors.
Round 2 procedures mirrored round 1 with 163 low-income women each completing one half of the fdSI items. In addition, 9 women recruited from low-income venues completed the entire 38-item survey and participated in a cognitive interview. Testing prompted revision of 10 items to better convey elusive concepts, removal of 13 questions, and addition of 2 items because they either triggered responses inconsistent with the intended meaning or produced redundant responses. Fifteen questions were unchanged because respondent interpretation was consistent with the meaning intended by the expert panel.
Refinement Phase
Cognitive interviews for all 27 items were held subsequent to fdSI completion with 23 low-income women from Pennsylvania. Mapping survey responses to cognitive interview remarks prompted slight revision to seven items to enhance face validity (i.e., congruence between intended item meaning and respondent comprehension).
Transitional Phase
fdSI generalizability to women from middle-income venues was confirmed by administering the 27-item fdSI to parents with children ages 2 through 5 years who attend preschools (n=7) with admission fees incompatible with low-income status. Collaborating with preschool administration, study materials (letter to caregivers, informed consent, survey with instructions, and envelope for returning completed forms to preschool), was sent home with each child in the targeted age range. Survey distribution was staggered among preschools until achieving the targeted sample size of 120 participants. Caregivers completed and returned surveys at their convenience. Participation was incentivized with a book on child feeding.
Of 132 participants who returned surveys, 111 (84%) indicated interest in further participation and provided contact information. Selection of cognitive interview participants considered parent and child ages, as well as survey responses to facilitate breadth of interview findings. Cognitive interviews (n=20), which were held approximately 2–3 weeks after survey completion, were conducted in private with a trained observer taking hand-written notes. A $20 discount store gift card was handed out upon survey completion.
Participant characteristics are shown in Table 1. For slightly more than half (54%), the child of focus was a firstborn. fdSI scores ranged from 53 to 95, and the mean score was 76.2±7.6. Internal consistency of the 27-item instrument was apparent with an acceptable Cronbach's alpha of 0.71. Parent leadership scores tended to correlate with child autonomy scores (r=0.16; p=0.07). Cognitive interviews and response mapping results supported concerns about instrument ability to identify and define child autonomy and parent leadership practices. Discrepancies between participant's survey response and verbal response were identified. Of the 27 items on the survey, 15 evoked discrepant responses. Twenty-five discrepancies were identified among the 15 items. As a result of discrepant response analyses, 14 items were discarded because they were not understood as intended and did not fully capture or measure parent leadership or child autonomy. Nine items were revised to improve item comprehension and three new items were added, producing a test with 16 items; eight addressing parent leadership and eight child autonomy.
Characteristics of Participants from Last Three Phases of Survey Development
ecSatter Inventory for Low-Income (ecSI/LI); possible range, 0–48.
Eating competence is defined by an ecSI/LI score ≥32.
Federal Special Supplemental Nutrition Program for Women, Infants, and Children (WIC).
Supplemental Nutrition Assistance Program (SNAP).
Current or previous use of either SNAP or WIC programs.
SD, standard deviation.
Assurance Phase
Findings from examination of the 16-item fdSI by two participant groups assured researchers that items approached their intended purpose. Both groups were English literate with children ages 2 through 5 years, but one was low income, being recruited in a WIC clinic to participate in an interview immediately after their appointment (n=9). The other group consisted of 5 participants from the Transitional phase who were not low income, had indicated an interest in additional participation, and had also provided discrepant survey and interview responses to the Transitional phase fdSI. For both groups, surveys were administered in person (following verbal informed consent) and completed by hand. Cognitive interviews were conducted in a private room immediately after survey completion, with findings captured by audio recording and hand-written notes by an experienced observer. As in previous phases, participants received a $20 gift card to a discount store upon interview completion.
All participants were white/non-Hispanic and mean eating competence (EC) scores or proportion defined as EC paralleled those of earlier studies (see Table 1).37–43 More participants in the low-income group were Supplemental Nutrition Assistance Program (SNAP) participants, (63% vs. 0%) and worried about having enough money for food (33% sometimes vs. 0%). They were also younger (28.25±5.39 vs. 35.00±3.74), and less educated (33% with a two- or four-year college degree vs. 100%).
Table 2 shows survey responses to fdSI items, including 13 items with varying degrees of change (i.e., no change, slight change, or substantial change), for the 5 participants who completed both Transitional and Assurance phase fdSI versions. For the four unchanged items, 90% of the surveyed responses were either the same or differed by only one response option (e.g., sometimes vs. often or always vs. often). Of the five items with slight (i.e., one- to two-word or addition of phrase) revisions, 92% of responses to the Transitional phase fdSI and the Assurance phase fdSI were either the same or similar. For the four items that were substantially changed (i.e., item was completely reworded to better capture intended construct), only 55% of responses were either the same or similar. For example, the Transitional phase item, If I think my child has eaten enough, I try to get him or her to stop, is presented in a negative manner, but the Assurance phase item, I let my child eat until s/he gets full, is worded in the affirmative. As a consequence, responses for this item switched directionality (i.e., never to always; see Table 2).
Comparison of Survey Responses from the 5 Participants Completing Both the Transitional and Assurance Phase Instruments
Only the 13 items that were unchanged or revised between the Transitional and Assurance phases are included. Differences between items are bolded.
Response options include: A (Always); O (Often); S (Sometimes); R (Rarely); and N (Never).
As illustrated by Table 2, cognitive interviews in the Assurance phase confirmed improved understanding of changes to the Transitional phase items. Items evoking discrepant responses in the Transitional phase did not evoke discrepant responses as revised for the Assurance phase. For example, in the Transitional phase, two participants provided survey responses that were discrepant from their cognitive interviews to the item, Between meals I offer my child snacks at about the same times every day. For the Assurance phase item, When I am home, I offer my child snacks at about the same times, both participants provided congruent survey and cognitive interview responses.
Interview responses for all 14 Assurance phase participants were congruent, with survey responses indicating that participants comprehended most items as intended. Discrepant responses (listed in Table 3) were provided for 5 of the 16 items. Of the original 16 items, 13 were retained without revisions because interview responses matched the survey response option selected. In the Assurance phase, parental pressure to eat (i.e., not providing for child autonomy) was assessed with two statements: I have to do something to get my child to eat new foods and I struggle to get my child to eat. For the first statement, response mapping identified three response options with interview and survey discrepancies; for the second statement, discrepancies were not apparent. Because lack of discrepancies indicated that the “I struggle …” item more accurately reflected the participant's use of pressure on the child to eat, this item was retained and the “I have to do something …” item was discarded.
Items in the Assurance Phase with Discrepant Responses between Cognitive Interview Responses and Survey Completion
Seven participants in the Assurance phase did not provide a discrepant response—these participants provided congruent responses for all 16 items.
First letter represents participant's response on survey; letter in parentheses represents the mapped response from the cognitive interview.
Response options include: A (Always); O (Often); S (Sometimes); R (Rarely); and N (Never).
In the Assurance phase, interview responses to the item, I let my child eat until s/he gets full, indicated the item was not capturing child autonomy because participants conferred varying meanings to being full. Three parents reported that they decided when their child was full, 6 said their child would tell them when s/he was full, and 4 said the child's behavior (i.e., pushing plate away, getting down from the table) indicated that they were finished. This latter response reflected application of sDOR. To better capture child autonomy in the feeding situation, the item was reworded to, I let my child eat until s/he stops eating and doesn't want more.
The item, We have leftovers after meals, was developed to address having or preparing enough food. Three participants expressed confusion with the term leftovers. Some thought this item meant that they ate leftovers after they were finished with the meal, which was not the intended meaning of this item. To improve clarity of understanding, the item was reworded using participants' phrasing to, We have food leftover after meals. Details and rationale of item modifications are shown in Table 4. Assurance phase findings resulted in a 15-item fdSI for the Launching phase (see Table 4).
Outcomes from the Assurance Phase: Rationale of Changes and Item Modifications
(L) indicates parent leadership item; (A) indicates child autonomy item.
Responses include: A (Always); O (Often); S (Sometimes); R (Rarely); and N (Never).
Eating competence relates to feeding
Interview responses of participants who were not EC (i.e., ecSI/LI <32) indicated being hesitant to provide their child autonomy in the feeding situation (i.e., they did not trust their child to decide how much or whether to eat). For the item, If I think my child hasn't had enough, I try to get him or her to eat a few more bites, one participant stated, “I make him eat everything, so I will try to get him to eat more. I bribe him with treats to get him to eat the food.” Others indicated they decided when their child was full, based upon the amount they thought their child should eat. Non-EC participants were more likely to perceive their child's eating negatively. One participant described her son to be “really picky” and also stated on two occasions that “he doesn't try new foods well.” Another participant mentioned that her son would eat brownies all day if she let him. In contrast, competent eaters perceived their child to be “good eaters.” Examination of verbal responses revealed limited use of coercion or pressure because their children were competent with eating. Another respondent said, “I never have to do something to get him to try new foods, because he is a really good eater.” Another participant stated, “He's good with eating, so I never have to make him eat new foods. He likes most foods.” All three participants with ecSI/LI scores above 40 mentioned, on multiple occasions, that their child was a good eater. The small sample size limited conferring internal consistency, but the 15-item fdSI was suggested as potentially reliable with a Cronbach's alpha of 0.60.
Launching Phase
Parents of children 2 through 5 years of age were recruited from local WIC program sites to participate after their scheduled appointment. As shown in Table 1, participants (n=10) were mostly white/non-Hispanic, SNAP participants, and not EC. Participants were more racially diverse than in other phases, but other demographic characteristics were similar. Comparison of the summed 14 items common to the Assurance and Launching phase fdSI versions supported fdSI readiness for further testing, including construct validation. Mean scores were 32.4±4.9 and 31.7±3.9 for the Assurance and Launching phases, respectively. Very few survey and interview discrepancies were noted, and responses to the two revised items (I let my child eat until s/he stops eating and doesn't want more and We have food leftover after meals) were congruent with only one discrepant response. In addition, unlike earlier phases, participants did not ask for item clarification during survey completion.
Progression of item generation, revision, and deletion aligned with sDOR tenets about parent leadership and child autonomy is shown in Table 5 and underscores the value of a constant comparative approach with attention to face and content validity in fdSI development. In addition, this display demonstrated that the number of items to reach conceptual understanding is asymmetrical, varying for each concept. sDOR Parent Leadership and Child Autonomy are each described by three fdSatter concepts, and in the Foundational phase, each concept was represented by as many as 10 or as few as two items. By the Launching phase, a concept could be represented by nearly the same number of items (i.e., going from six to five) or the concept abandoned (i.e., going from eight to zero items) because none of the concept's items were comprehended. The latter was the case when testing the concept of the parents' positive feelings about the child's eating and weight. Stressing item comprehension, rather than adherence, to an a priori item pool size or balance mitigated symmetry-driven decisions.
Thematic Progression in Phases of Item Generation and Revision for the Satter Feeding Dynamics Inventory
Indicates item is reverse scored.
Change in wording transformed the item from a parent leadership to a child autonomy item.
Discussion
sDOR has been used widely in parent education and clinical intervention relative to child obesity with parents of preschoolers. The sDOR elements of parents taking leadership with feeding and giving children autonomy with eating are subjective, contextual, and potentially amorphous and thereby difficult to measure. This project is a first step in preparing an instrument to objectively measure those elements by establishing translational validity of an item pool. Only an instrument with documented shared understanding can be tested using advanced psychometric analysis. To develop the fdSI to be a tool with shared understanding this project nurtured five distinct phases utilizing several rounds of survey completion and cognitive interviews. Fifteen face and content valid items to examine adherence to sDOR were generated, readying the fdSI for studies to establish construct integrity. Participant responses indicated that items captured parent ability to take leadership with feeding and give the child autonomy with eating. Inclusion of participants in both the Transitional and Assurance phases who were not low income demonstrated generalizability of survey items from a low-income population.
Findings supported evaluating EC when examining parent feeding practices. Participants with higher ecSI/LI scores provided comments more compatible with sDOR, indicating that parent EC may relate to fdSatter. Perceptions of child eating behaviors tended to differ between EC and non-EC participants. Participants with the highest ecSI/LI scores referred to their children as “good eaters,” whereas non-EC participants frequently described their child's eating negatively. EC adults, as defined by ecSatter, experience a positive affect about eating, consistently provide themselves with adequate amounts of rewarding food, attend to internal cues of hunger, appetite, and satiety to regulate food intake, take an interest in unfamiliar food and routinely develop comfort with eating it, and eat in a structured, attentive fashion. 44
fdSatter, the same as ecSatter, is predicated on the utility and effectiveness of biopsychosocial processes: hunger and the drive to survive; appetite and the need for pleasure; the social reward of sharing food; and the biological propensity to maintain preferred and stable body weight. 44 Thus, parents who are themselves EC are positioned to maintain an appropriate balance of responsibility with their child and avoid the use of coercive feeding strategies, such as food restriction and pressure to eat. 45 If further examination reveals that EC aligns with fdSatter, then enhancing EC may be a means to improving feeding dynamics 46 and preventing child obesity.
Utilization of an iterative approach to map cognitive interviews to survey responses was unique to fdSI item pool design. Cognitive interviews provided rich insight into meanings and interpretations of health and nutrition topics. 47 Iterative application allowed outcomes from each fdSI developmental phase to be applied in generating items that captured particular feeding constructs.
A few feeding tools that address parental feeding practices were subjected to cognitive testing, but not iterative application. Subsequent to instrument development, the Caregiver's Feeding Style Questionnaire underwent cognitive interviews with low-income African American and Hispanic participants, and changes were made based on interview feedback. 27 Jain and colleagues conducted semistructured interviews to assess validity of Parental Feeding Questionnaire items with African American participants, and interview responses revealed that three of the eight constructs were consistently misunderstood across research subjects. 29
Mapping survey responses to cognitive interview comments postured the capture of parent feeding behaviors as more than single-item revision or deletion, but rather a contextual integration of parents' ideas. For example, with respect to giving children autonomy with what they will eat, the descriptive, survey, and interview congruent Launching phase item, “I struggle to get my child to eat,” was commuted from three Foundational phase items describing specific parent actions. Also, with respect to child weight, continuous response mapping of six items denoting parent attitudes and feelings toward child eating and weight revealed significant dissonance between what a parent will note on a survey and what they really mean. Removal of weight-related items is a departure from current practice. However, our findings suggest that adhering to sDOR will correspond to appropriate concerns about weight and growth, that is, such questions are not needed and, because they are misinterpreted by parents, provide invalid information and confuse decisions about treatment and policy development.
fdSI items focus on meals because they are consistent with fdSatter and provide the most opportunity for exposing the themes of parent leadership and child autonomy. Meals are a metaphor for parent ability to plan and implement parenting skills. Planning and providing sit-down snacks at a set time in a particular place is also an important part of sDOR. However, this concept proved impossible to capture. Instead, three items relate to snacking: Drinks whenever he or she wants; Eats whenever he or she wants; and Offers snacks at about the same times. This parsing out of snacking behavior may adequately capture parent leadership with respect to not allowing the child unplanned access to food and drinks.
Strengths and limitations
A fundamental strength of this study was the administration of cognitive interviews in tandem with survey completion enabling verbalizations to be mapped to paper-pencil output. Observer bias was reduced because cognitive interviews were conducted by three researchers across phases. In addition, our sample was diverse in income and education levels. However, generalization of results is limited because of racial and ethnic homogeneity, and although usual recruitment venues and methods were followed, we cannot be certain that participants represent low-income women. Indeed, the proportion of EC persons and mean ecSI/LI scores were slightly higher than previously reported for low-income women.40,48 Item comprehension and feeding practices may differ by race or ethnicity, warranting further study with a racially/ethnically diverse sample. The small sample size, which is appropriate for qualitative studies involving cognitive interviews, requires a conservative interpretation of the findings.
Conclusions
Findings from this study offer a step closer to a valid tool to measure adherence to sDOR. A validated measure of parent-child interactions around feeding is critical to public health policy making, programming, and intervention assessment relevant to child obesity.
Thus, the presence of an instrument so rigorously tested in formative assessment and readied for construct validation, including confirmatory factor analyses and structural equation modeling, provides optimism for future research and treatment of parent-child interactions in feeding that are associated with child obesity.
Footnotes
Acknowledgments
This study was funded by the Food and Nutrition Service SNAP-Ed program of the USDA through a contract from the Pennsylvania Department of Public Welfare to The Pennsylvania Nutrition Education TRACKS of Pennsylvania State University. The authors thank Christine Least for her work with data collection in the early phases of survey development. The authors also thank Jodi Stotts Krall for her presubmission review of the manuscript.
Author Disclosure Statement
Ellyn Satter, MS, RD, LCSW, BCD, receives royalties from educational materials about child feeding.