
Abstract
Abstract
Background:
Physician counseling on lifestyle factors has been recommended as one way to help combat the obesity epidemic in the United States. The aim of this study was to examine the frequency of lifestyle counseling among healthy weight, overweight, and obese adolescents and determine the contributions of adolescent weight and physical activity.
Methods:
Self-reported surveys on dietary and physical activity counseling, along with measured height, weight, and physical activity data by accelerometry were collected on 76 adolescents ages 11–14 years. General linear models tested for associations of reported lifestyle counseling by weight category, adjusting for physical activity, age, gender, race/ethnicity, and parent education.
Results:
Half (47%) of the subjects were overweight or obese. Frequency of lifestyle counseling varied by weight category, with obese adolescents reporting greater amounts of lifestyle counseling across all topics than their peers. Obese adolescents received more dietary (β=0.88; standard error [SE]=0.25; p=0.001) and physical activity (β=0.80; SE=0.28; p=0.006) counseling than healthy weight youth, as well as being told to increase their physical activity more often (β=0.96; SE=0.29; p=0.001). There were no differences in lifestyle counseling between overweight and healthy weight subjects. Adolescents with greater daily moderate-to-vigorous physical activity reported less physical activity counseling (β=–0.02; SE=0.008; p=0.05).
Conclusions:
Despite universal recommendations to counsel adolescents on lifestyle, only obese adolescents consistently report receiving such counseling. Given known difficulties in reversing obesity after onset, efforts should ensure that all adolescents receive lifestyle counseling.
Introduction
The prevalence of pediatric obesity remains a major public health problem in the United States. 1 Obesity can lead to increases in blood pressure and blood lipids, two leading risk factors for cardiovascular disease (CVD). 2 Several established risk factors for CVD, including obesity, elevated blood lipids, and diabetes, have been shown to start as early as adolescence.3–5 Adolescence therefore represents a pivotal and actionable time period during which risk factors for adult morbidity and mortality, including obesity, can be measured and addressed, yet studies have shown low rates of physician- and parent-reported lifestyle counseling among providers caring for adolescents.
Healthcare providers, including physicians and nurse practitioners, would seem well positioned to play a role in obesity prevention and treatment counseling, because most US youth interact with a healthcare provider at least once during the year. 6 Moreover, lifestyle counseling on healthy eating and being physically active are part of well child care 7 and are especially important for prevention of overweight and obesity. Despite recommendations from the American Academy of Pediatrics, the American Medical Association, the CDC, and the US Department of Health and Human Services that clinicians should screen and counsel youth at least annually for overweight and obesity,8,9 providers report that lifestyle counseling for obesity often occurs infrequently as a result of a host of reasons, including visit time constraints, poor reimbursement, and low provider self-efficacy. 10
Previous studies have sought to identify patterns of physician counseling in the areas of diet and physical activity. Though these studies have tended to adjust for weight status,11–13 few studies have investigated the role of physical activity. Physical activity is known to have beneficial health effects independent of weight status. 14 Adolescent physical activity levels may play an important role in determining which patients receive lifestyle counseling, even after adjusting for weight status. For example, adolescents who report participating in sports or frequent forms of daily physical activity (e.g., walking to school) during annual well child care visits may prompt providers to not counsel on physical activity in the belief that this topic has already been covered or that current physical activity recommendations are being met, regardless of weight status. Using direct adolescent report of diet and physical activity counseling and behaviors, along with objective and self-reported measures of physical activity, this study sought to determine whether weight status was associated with different rates of counseling. It was hypothesized that overweight and obese youth would receive more counseling on both diet and physical activity than their healthy weight peers, 13 after adjusting for BMI and physical activity, and that youth with greater physical activity levels would be less likely to report physician counseling on physical activity.
Methods
This study used survey data collected as part of CUBES (Children's Use of the Built Environment Study), a longitudinal study of physical activity and the built environment to assess adolescents' report of receiving physician counseling on diet and physical activity. The data used for this study are cross-sectional.
Participants/Sample
A convenience sample of 11- to 14-year-old non-Hispanic white, non-Hispanic black, and Hispanic adolescents being observed at a local community health center and attending a community recreation center and residing in three middle- and low-income communities (Lynn, Winthrop, and Revere) in the greater Boston area were recruited to participate in a study of physical activity and the built environment. Recruitment took place from April 2011 to April 2012. Signed parental informed consent, along with signed child assent, was obtained from each family. The Partners HealthCare Institutional Review Board approved the study. A total of 96 participants were recruited, with 76 providing accelerometer and survey data necessary for inclusion in this study.
Data Collection and Measures
Physician counseling on diet and physical activity
Adolescent participants completed a questionnaire at study entry assessing their views on health, weight status, diet, physical activity, and physician counseling. The study included three questions assessing lifestyle counseling for diet and exercise: (1) “When you go to the doctor, how often does the doctor talk to you about physical activity?”; 2) “When you go to the doctor, how often does the doctor talk to you about eating well?”; and (3) “When you go to the doctor, does the doctor ever tell you that you should do more physical activity?” Possible answers for each item were: every time; sometimes; rarely; or never.
Measured physical activity
Physical activity was measured with accelerometers (GT3X; ActiGraph LLC, Pensacola, FL) worn on a belt around the hip, set to record at 30-second intervals. Subjects were instructed to wear the belt at all times during waking nonwater activity hours for at least 5 weekdays and 2 weekend days. Accelerometer data were cleaned and validated using ActiLife software (ActiGraph LLC). Periods of 60 minutes or longer of consecutive zeros were considered nonwear time and were removed from analysis. To be included in analyses, subjects were required to provide a minimum of 8 valid hours of data per day for at least 3 days.15,16 Data collected between the hours of 12:00 am and 5:00 am were considered sleep time and were excluded from analyses. Accelerometer data were classified into age-specific intensity categories, with total minutes at or above the moderate-to-vigorous physical activity (MVPA) threshold (≥2296 counts per minute) 17 divided by the number of valid days to obtain minutes of MVPA per day.
Self-reported physical activity
Self-reported physical activity was assessed using the Physical Activity Questionnaire–Children/Adolescents (PAQ-C and PAQ-A), as age appropriate, a validated self-report instrument for assessing physical activity.18,19 The PAQ is a nine-item instrument, with each item scored on a 5-point scale, with a mean score of the items derived to produce a final PAQ activity summary score.
Anthropometrics
Height and weight were measured using a stadiometer (SECA, Hanover, MD) and a digital scale (LifeSource MD; A&D Engineering, Inc., San Jose, CA) by trained research staff, with participants wearing indoor clothing, pockets emptied, and shoes removed. Measurements were taken in duplicate and then averaged, from which BMI was calculated using age- and gender-specific CDC growth curves and classified into weight status categories: healthy weight (BMI ≥5th–<85th percentile); overweight (BMI ≥85th–<95th percentile); and obese (BMI ≥95th percentile). 20
Demographics
Self-reported age (date of birth), sex, and race/ethnicity categorized as non-Hispanic white, non-Hispanic black, and Hispanic/Latino were obtained at baseline, along with parent-reported highest reported level of parental education.
Statistical Analysis
Study sample characteristics were reported using descriptive statistics. Bivariate analyses with Kruskal-Wallis tested whether frequency of counseling differed by weight category. General linear models were run to identify potential predictors of physician counseling, with counseling on diet and physical activity on 4-point Likert scales as dependent variables and BMI category, age, gender, race/ethnicity, and parental education as independent variables. Mean daily minutes of MPVA and mean PAQ score were also included as independent variables in the models predicting physical activity counseling.
Results
A description of the 76 subjects is provided in Table 1. The study sample was reasonably distributed, with 42% age 11 years at enrollment, 40.8% male, 43.4% white, and 47.4% overweight or obese. Nearly all (90%; 68 of 76) adolescents reported having received physical activity counseling from a doctor, with 30% (23 of 76) reporting counseling at every visit. Similarly, 92% (70 of 76) of respondents reported receiving healthy eating counseling, with 37% (28 of 76) reporting such counseling at every visit. Sixty-six percent (50 of 76) of adolescents reported having received recommendations from a doctor to be more physically active. Subjects provided, on average, 6.2 days (range, 3–10) of validated activity data. Mean daily MVPA was 31.2 (standard deviation [SD], 16.8) minutes. Boys had greater mean daily MVPA levels than girls (47.7 vs. 32.2 minutes; p=0.004), with no differences observed by race or weight category. Mean PAQ score for self-reported physical activity was 2.54 (SD, 0.76), comparable to the original reported score of 2.31 (SD, 0.63) among adolescents who validated the original instrument. 19 There were no differences in mean PAQ score by race or weight category, but, similar to national studies of physical activity patterns, 21 boys reported higher physical activity levels than girls (mean PAQ score, 2.78 vs. 2.38; p=0.02).
Demographic Characteristics of Study Participantsa
n=76.
Healthy weight, BMI ≥5th–<85th percentile; overweight, BMI ≥85th–<95th percentile; obese, BMI ≥95th percentile (adjusted for age and sex).
Range, 1 (low physical activity) to 5 (high physical activity).
PAQ, Physical Activity Questionnaire; MVPA, moderate-to-vigorous physical activity.
Table 2 reports the frequency of physician counseling on diet and physical activity by weight category. Notable differences in frequency of counseling by weight category were present for every lifestyle counseling topic. Among healthy weight adolescents, 13% reported never having discussed either diet or physical activity when they were observed by doctors, with one third reporting having rarely discussed physical activity and one quarter reporting having rarely discussed diet. Among overweight adolescents, nearly one quarter (24%) reported only rarely receiving physical activity or dietary counseling. In contrast, over half (56%) of obese adolescents reported receiving physical activity counseling at every visit; two thirds reported receiving dietary counseling at every visit. One third of obese adolescents reported being told to increase their physical activity at every visit.
Adolescent Reported Frequency of Physician Counseling on Diet and Physical Activity by Weight Category
In adjusted models, weight category remained significantly associated with every lifestyle counseling question (Table 3). Compared to healthy weight adolescents, obese adolescents reported more physical activity (β=0.80; standard error [SE]=0.28; p=0.006) and dietary counseling (β=0.88; SE=0.25; p=0.001). Obese adolescents also reported a higher frequency of being told by a physician to be more physically active, compared to their healthy weight peers (β=0.96; SE=0.29; p=0.001). There were no differences in counseling frequency on any topic between overweight and normal weight subjects. Among the covariates, mean daily MVPA was borderline inversely associated with being told by a physician to increase physical activity (β=−0.02; SE=0.008; p=0.05). No other covariates were significantly associated with receipt of physical activity or dietary counseling. Figure 1 represents the adjusted estimated marginal means and SEs for receiving lifestyle counseling by weight category, illustrating increased frequencies of counseling for all topics among obese adolescents, compared to their overweight and healthy weight peers (Fig. 1).
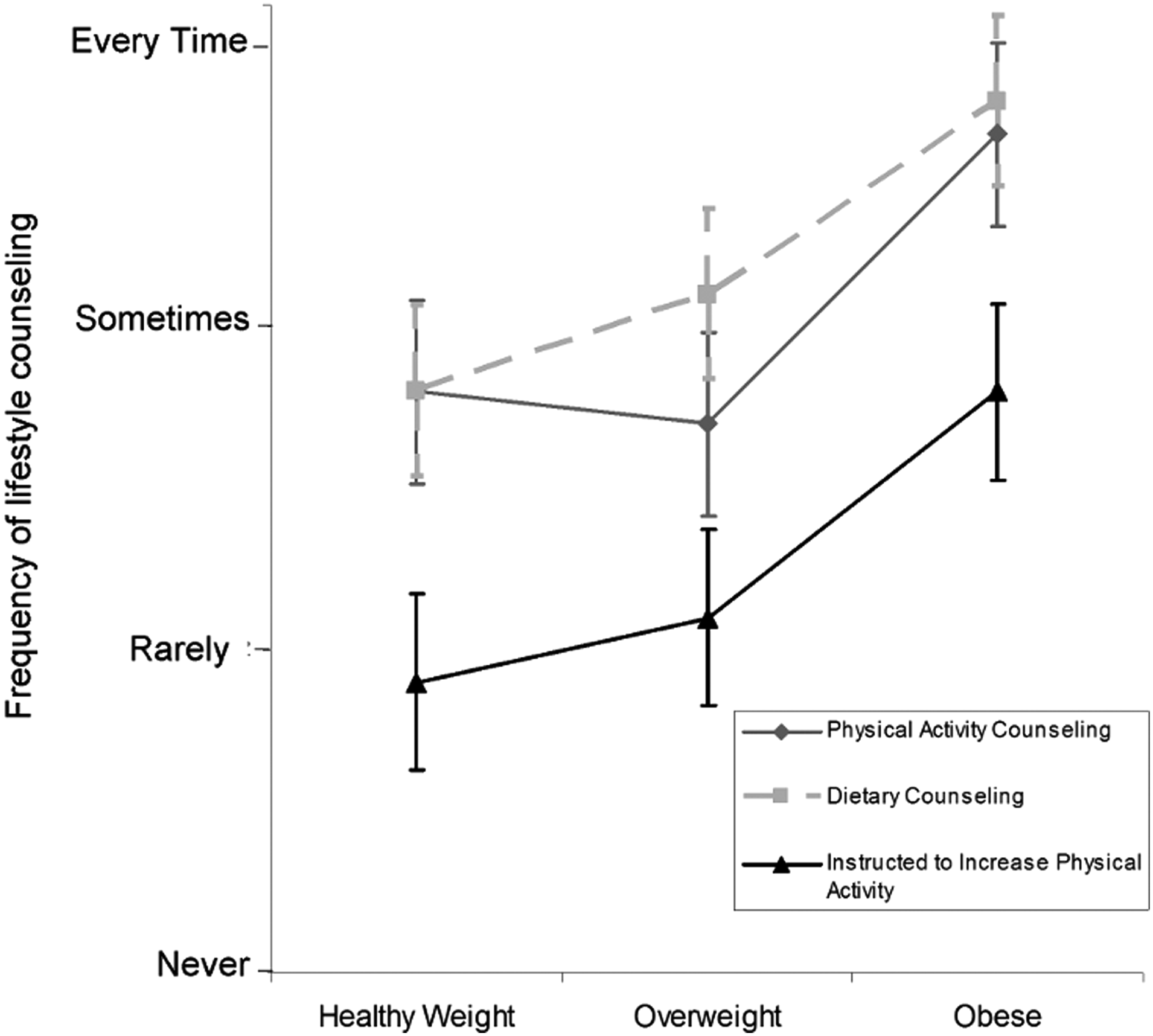
Mean levels of lifestyle counseling by weight category.
General Linear Models of Associations between Adolescent-Reported Lifestyle Counseling with Weight Category
Also adjusted for age and mean Physical Activity Questionnaire score.
Also adjusted for age.
p<0.05.
SE, standard error; MVPA, moderate-to-vigorous physical activity (mean daily minutes).
Discussion
This study sought to better understand and identify patterns in physician counseling on lifestyle modifications as reported by adolescents themselves. This study found that the only consistent predictor associated with physician counseling was adolescents' weight status, with obese youth reporting more counseling on lifestyle factors than their healthy and overweight peers. This was after accounting for the adolescent's actual and reported physical activity level, as well as sociodemographic characteristics. A marginal association was also found between adolescent physical activity and specific recommendations to increase physical activity, such that less-active adolescents reported receiving advice to do more physical activity more often from their doctors, even after adjustment for weight status.
The findings in this study that obese youth report being more likely to receive lifestyle counseling than their overweight and healthy weight peers could be explained several ways. The findings could represent real counseling trends: When doctors encounter an obese patient, perhaps they are more primed to counsel on diet and physical activity than if the patient is of healthy weight or overweight. This would represent an acknowledgment that physicians recognize obesity to be a problem and are attempting to do something about it. Despite these efforts to treat, such a pattern is problematic because it suggests that healthcare providers may be missing an opportunity for prevention. The alarmingly high prevalence of obesity and the difficulty in reversing obesity call for greater prevention efforts. Moreover, studies have shown adolescents to be receptive and interested in receiving dietary and exercise counseling, 22 making the shortcomings in counseling a lost opportunity. These data could represent recall bias, whereby obese children recall having a doctor discuss diet and exercise more frequently with them than their healthy weight peers. Regardless of the underlying mechanism, the finding that obese youth consistently reported higher rates of counseling than overweight and healthy weight adolescents on all lifestyle topics suggests an important opportunity for intervention. In addition, because recall is likely an important factor in affecting behavior, whether these data reflect true patterns or merely recall may be less important.
This study's findings in adolescents are similar to those in a recent study by Kallem and colleagues, which found that obese children were more likely to report lifestyle counseling than overweight and healthy weight children. 23 Whereas the study by Kallem et al. assessed counseling categorically with a yes or no question, our study offers further insight by providing information on recalled frequency of counseling. This study also accounted for physical activity, a potential confounder of receiving exercise counseling. Adolescents were found to report low overall rates of lifestyle counseling by doctors caring for youth, similar to findings reported by Taveras and colleagues. 12 In a recent study looking at parent-reported doctor communication on weight status, Perrin and colleagues found that less than one quarter of parents of overweight children ages 2–15 years reported being told their child was overweight by a pediatric care provider, though, in a pattern similar to the weight-based counseling trends we found in our study, reports of being told the child was overweight improved with increasing weight status. 13 This study's data illustrate a similar pattern, whereby healthy and overweight youth are not universally discussing healthy lifestyle modifications with their doctors, and it is not until youth become obese that they consistently receive counseling.
The finding that a sizable proportion of overweight adolescents do not report receiving lifestyle modification counseling is concerning, given the known ill health effects of increased adiposity. National levels of physical activity in adolescents are known to be insufficient, 24 and, in our study, we found adolescents achieved, on average, less than half the daily recommended level of MVPA. Despite this, only two thirds of overweight participants report receiving regular counseling on physical activity, and only one third report being told to increase their physical activity levels at physician visits. Pediatricians face many well-described barriers to providing counseling, 10 which may impede appropriate care until patients are obese. Finding ways for healthcare providers to intervene earlier, even if after a patient has become overweight, may play a role in reducing the obesity burden. A full population health approach would be to offer high counseling rates to all children and adolescents, even those of healthy weight, in an effort to prevent overweight and obesity in later years.
This study has several limitations. Counseling rates are self-reported by adolescents and subject to recall bias, including the possibility that reported counseling may be based on the general feelings of adolescents, rather than in reference to specific physician encounters. This study did not audio- or videotape counseling and, therefore, was not able to verify adolescent reports, nor were parents included as respondents to verify the adolescent report. This study also does not have information to contextualize and better understand the reported counseling patterns, including possible physician barriers to counseling. Data were not collected on how often adolescents sought care, which may falsely increase the weight of reported values in adolescents who are counseled less frequently. Information was not available on when participants last saw a provider nor were subject charts reviewed for documentation of counseling to assess the accuracy of the adolescent self-reports. This study used the PAQ, a validated physical activity questionnaire for youth, but reliability and validity both remain a concern for all physical activity questionnaires. 25 The counseling survey items were based on previously published surveys and pilot tested by adolescents and experts in survey methods and pediatric obesity after being modified for our study aims, but were not validated using formal psychometric testing. The study was conducted in one greater metropolitan region with subjects primarily residing in middle- and low-income neighborhoods, which limits our ability to address socioeconomic determinants, and findings may not be generalizable to national counseling patterns.
However, this study also has several strengths. BMI data were measured and obtained at the time of questionnaire completion, thus eliminating the possibility of weight status misclassification. Physical activity data were collected to control for physical activity level to account for the possibility that adolescents reporting greater physical activity may consequently not receive physical activity counseling. This study also queried adolescents themselves, who are somewhat independent from parents with respect to physical activity and dietary patterns. Few studies have queried adolescents themselves about physician counseling, despite the recommendations that physicians have time with adolescents independent of their parents.
Conclusions
Weight status and physical activity level, but not other sociodemographic characteristics, were associated with receipt of physician counseling on lifestyle modifications among middle-school–aged youth. Although obese youth report more frequent counseling than nonobese peers, which may help in weight reduction efforts given the increasing prevalence of, and difficulty in treating, obesity, efforts should be placed on finding ways to facilitate healthcare provider counseling on lifestyle modifications for all patients, thus moving counseling more toward disease prevention, rather than response to an already apparent health problem.
Footnotes
Acknowledgments
All phases of this study were supported by the National Institutes of Health/National Heart, Lung, and Blood Institute (5K23HL103841; principal investigator, N.M.O.). The study was also funded by a grant to Dr. Oreskovic from the Boston Nutrition Obesity Research Center.
The authors thank Menghua L. Chen for her statistical assistance.
Author Disclosure Statement
No competing financial interests exist.