
Abstract
Abstract
Background:
Urban elementary schools in minority communities with high obesity prevalence may have limited resources for physical education (PE) to achieve daily activity recommendations. Little is known whether integrating physical activity (PA) into classrooms can increase activity levels of students attending such schools.
Methods:
We conducted a cluster randomized, controlled trial among kindergarten and first-grade students from four Bronx, New York, schools to determine feasibility and impact of a classroom-based intervention on students' PA levels. Students in two intervention schools received the
Results:
A total of 988 students participated (intervention group, n=500; control group, n=488). There was no significant difference at baseline between the two groups on mean number of steps (2581 [standard deviation (SD), 1284] vs. 2476 [SD, 1180]; P=0.71). Eight weeks post–CHAM JAM, intervention group students took significantly greater mean number of steps than controls (2839 [SD, 1262] vs. 2545 [SD, 1153]; P=0.0048) after adjusting for baseline number of steps and other covariates (grade, gender, recess, and PE class). CHAM JAM was equally effective in gender, grade level, and BMI subgroups.
Conclusions:
CHAM JAM significantly increased school-based PA among kindergarten and first-grade students in inner-city schools. This approach holds promise as a cost-effective means to integrate the physical and cognitive benefits of PA into high-risk schools.
Introduction
The prevalence of obesity in the United States' (US) elementary school children ages 6–11 years has nearly tripled in the past 30 years, with 18% of children being obese. 1 Urban minority children have been disproportionately affected by the obesity epidemic, with prevalence rates reaching 26% in some low-income minority communities, such as the Bronx, New York. 2 Obese children tend to become obese adults and are at high risk of obesity-related adverse outcomes.3,4 Physical activity (PA) can lower the risk of becoming overweight and developing related diseases.5,6 However, PA is, on average, low in US children.7,8 Moreover, low-income and minority children have lower levels of PA, fitness, and sports participation than their high-income or white peers.8,9 Previous studies have also observed lower PA enjoyment and reduced PA levels in overweight/obese children and adolescents.10,11
Medical and public health authorities recommend daily school physical education (PE) as a way to combat childhood obesity.12,13 However, many schools in low-income communities, such as the Bronx, New York, do not have facilities (e.g., physical space) for PE, PE teachers, or trained classroom teachers to provide daily PE for all students.14,15 Even the schools with gymnasiums and play spaces often use them as classrooms to ease overcrowding.
14
In addition to these obstacles, urban school staff have a historical resistance to PE, believing that PE will reduce instruction time for core academic subjects.16,17 Despite multiple studies of school-based PA programs in the United States and other countries aimed at promoting PA and fitness in children,18–26
limited research is available on effectiveness of such programs in urban minority young children attending low-resource public schools. The
Methods
Study Design and Randomization
We conducted a cluster randomized, controlled trial (RCT) at four elementary schools in the Bronx, New York, with school as the unit of randomization. Two schools were randomized to the intervention (schools 1 and 3) and two (schools 2 and 4) to control groups. This random allocation took place after Time 1 (baseline) data collection was completed. Intervention schools received CHAM JAM in addition to their regular PE classes. Control schools continued to provide PE class to their students as usual. A cluster design was chosen because the intervention was implemented at the school level to avoid contamination between intervention and control students. Given the nature of the intervention, blinding of schools, students, and research staff was not possible after random assignment and during Time 2 (at 8-week follow-up) measurements. Our primary outcome measure was PA levels during the school day, measured objectively with pedometers, at Time 1 and Time 2. The study was approved by both the New York City Department of Education and Montefiore Medical Center Institutional Review Board Committees. Passive consent was obtained using parental opt-out.
Participants
Four public elementary schools located in low-income neighborhoods of the Bronx, New York, were recruited in spring 2007. School selection was on the basis of the following criteria: (1) >80% of students qualified for the free/reduced lunch (a marker of family poverty) and (2) school leadership's commitment to accommodate the study. Participating schools were representative of Bronx elementary schools with regard to sociodemographic characteristics and available resources. Study schools had the following student sociodemographic characteristics: 89–99% of students were eligible for free/reduced lunch; 48–53% male; 62–78% Hispanic; and 20–38% African American. 27 Inclusion criteria for child participants included enrollment in the kindergarten or first grade and having no health limitations restricting participation in routine PE class.
Intervention
The CHAM JAM intervention is an audio CD consisting of 10-minute, education-focused aerobic activities that teachers can implement by playing the CD in their classrooms. CHAM JAM was based on the TAKE 10! program concept of engaging students in PA while reinforcing learning objectives. 28 Unlike TAKE 10!, which is a curriculum guide that teachers are trained to lead, CHAM JAM requires no previous teacher training. CHAM JAM was developed as modules that teachers could implement by playing a CD mixed in a recording studio by a professional disc jockey, who set the lessons to contemporary music. Professional actors read the lesson scripts that provide instructions to the students. The CHAM JAM intervention was based on an interval training approach, more characteristic of spontaneous PA in children, 29 with periods of more-intense exercise alternating with less-intense activity.
Twenty-five CHAM JAM lessons in both English (n=20) and Spanish (n=5; on mathematics, phonics, grammar, geography, time, and money concepts) were used in the study. Each lesson track has a standard 2-minute warmup, a variable 6-minute aerobic activity section, and a standard 2-minute cool down. Each middle section has a different type of music and academic skill. The academic skill in CHAM JAM was based on the material from the educational curriculum pertinent to each grade level and was developed in partnership with teaching experts. Intervention school teachers were instructed to play the lesson of choice (of 25 lessons) three times a day using a CD player that was provided by the study (for classes that did not have one), and students followed the recorded instructions. The teachers were free to either repeat the same lesson or choose a lesson that best suits the material being taught in the classroom. See http://chc.montefiore.org/physical-activity/show-kids-that-exercise-is-fun for more information on CHAM JAM.
Outcome Measures
Physical activity assessment
Number of steps per school day was measured with a pedometer (Yamax Digi-Walker SW-200; New-LifeStyles, Inc. Lees Summit, MO) using a validated methodology.30–32 Before the study, 10% of the pedometers were randomly selected to undergo shake and walking tests.33,34 We collected pedometer data for 5 consecutive school days during Time 1 and Time 2. We collected Time 1 pedometer data in all four schools before random assignment and over a 4-week period in November–December 2007. Schools 1, 2, and 3 had data collection during 3 weeks in December 2007 and school 4 during the last week of November 2007. Intervention was implemented immediately after Time 1 data collection. Time 2 pedometer measurements occurred 8 weeks postrandomization over a 3-week period in March–April 2008. Data during Time 2 was collected over a 3-week period owing to scheduling logistics. Details about procedures used for pedometer data collection have been reported on previously. 2
Anthropometric assessment
Research staff followed a standardized protocol 2 and measured each participant's standing height and weight at Time 1 using a digital scale with a stadiometer (Tanita electronic physician scale, WB-300; Tanita, Tokyo, Japan).
Physical education class, trip, and recess frequency assessment
We asked classroom teachers from all study schools to record whether the students had a PE class, trip, or outdoor recess on each day of PA monitoring at Time 1 and Time 2. In general, depending on the schedule, students from different classrooms at the study schools with gymnasium and PE teacher(s) had 0–2 PE classes per school week. 2
Intervention Implementation and Process Measures
We used the five dimensions of the RE-AIM framework of reach, effectiveness, adoption, implementation, and maintenance 35 to guide the identification of barriers and facilitators for participating schools in adopting, implementing, and maintaining the CHAM JAM intervention. Before Time 1 data collection, we met with all kindergarten and first-grade teachers to describe the study and their role. After Time 1 data collection, schools were informed of their group assignment. Immediately thereafter, in January 2008, CHAM JAM was implemented by the research staff, who demonstrated and led one CHAM JAM lesson for each intervention kindergarten and first-grade class. Intervention school teachers were asked to continue using CHAM JAM three times a day and record the number of times their class participated in the activity using the provided calendar. We conducted unannounced random direct observations of intervention and control classrooms during the 2 months of intervention delivery to assess levels of teacher adherence and student CHAM JAM participation in intervention classes as well as ensure that control schools had no PA program implemented during the course of the study. Individual teacher interviews were conducted at the end of the study to identify barriers and facilitators to implementation using open-ended questions. Comments were recorded by research staff at the time of the interview. Several teachers, who were absent on the days of the interview or who were not able to meet for the interview, provided written comments to these questions.
Statistical Analyses
Definitions and computations
BMI percentile was calculated by using each child's weight, height, age, and gender. In accord with national guidelines, we defined healthy weight as a BMI between 5th and less than the sex-specific 85th percentile, underweight as a BMI below 5th percentile, overweight as a BMI at or above the 85th percentile, but less than the 95th percentile, and obese as a BMI at or above the 95th percentile on the CDC's 2000 BMI-for-age growth charts. 36
Power analysis
The power for this cluster randomized trial was assessed assuming a sample size of two schools per intervention arm, 10 classrooms per school, and 25 students per classroom, for a total of 500 students per intervention arm. We further assumed based on previous studies that the standard deviation (SD) of the number of steps was approximately 1000 steps, the intraclass correlations in measures among students from the same classroom was 0.03, and among students from different classrooms within the same school was 0.01. Under these assumptions and using the method of Heo and Leon, 37 the study protocol as designed had 80% power with a two-sided type I error rate of 5% to detect a difference between intervention and control groups of 350 steps at the end of follow-up.
Data analysis
All data analyses were preceded by extensive data checking and verification to identify and resolve the reasons for missing values, inconsistencies, and out-of-range values. Extreme outliers, defined as days with step count <500 and >10,000, were just 1% of the total data and were excluded, as previously described. 2 We also excluded days when students went on school trips owing to the fact that these do not represent routine school-day activity. Descriptive statistics were computed to summarize demographic characteristics of the study population. PA levels were compared between intervention and control students by grade level, gender, and weight status. In separate subgroup analyses, the effect of the intervention was evaluated in the combined group of underweight and healthy weight students (BMI<85th percentile) and in overweight and obese students (BMI≥85th percentile).
To adjust for the within-cluster correlations at three different levels (student, classroom, and school), generalized linear mixed models (also termed hierarchical or multilevel models) were fit to evaluate differences in the number of steps between the intervention and control groups. The model included random effects for school, classroom, and subject, as well as fixed effects for grade, gender, outdoor recess, and PE class. The rationale for including the fixed effects in the model was to adjust for any imbalances in these variables across intervention groups; these imbalances can occur because of the small number of clusters (i.e., four schools), which were randomized to the two groups. A p value <0.05 was considered statistically significant. Data were analyzed using SAS software (Version 9.1; SAS Institute Inc., SAS 9.1, Cary, NC: SAS Institute Inc., 2000–2004). All analyses were based on the intent-to-treat approach, except where noted.
Results
The principals of all four selected schools agreed to have their schools participate in the study. Figure 1 illustrates enrollment and retention based on the CONSORT (Consolidated Standards of Reporting Trials) criteria. 38 Thirteen parents opted out of having their child participate in the baseline (Time 1) data collection, but subsequently opted in at the request of their children to have them participate in the follow-up (Time 2) data collection.
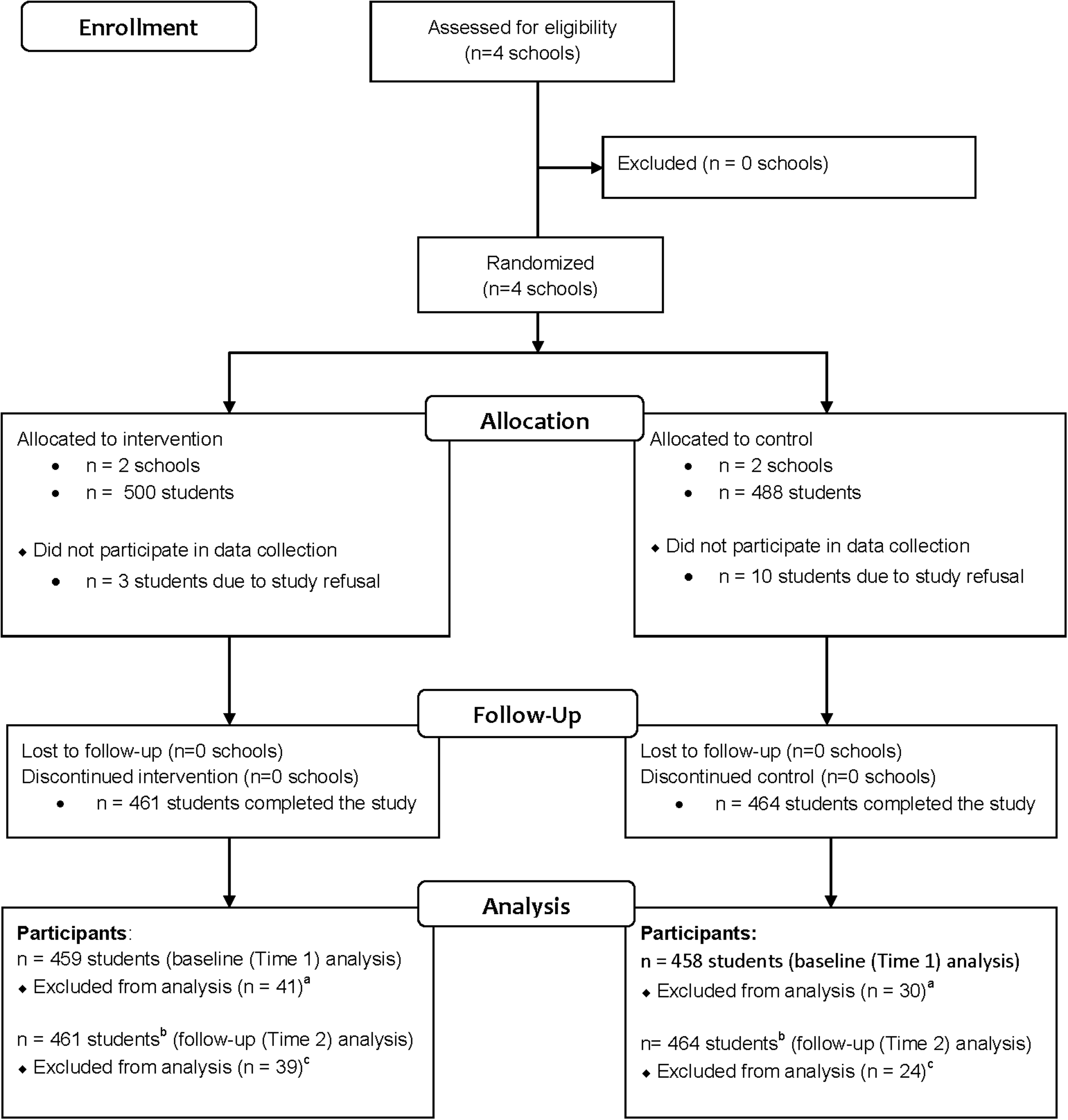
CONSORT (Consolidated Standards of Reporting Trials) 2010 flow diagram. aOwing to opting out or student absence during data collection. bNumbers differ at follow-up as a result of students transferring in/out of school and parents who opted out at baseline then opted in at follow-up. cStudents transferred or absent during data collection.
Sample Demographics
Overall, 988 kindergarten and first-grade students (n=500 intervention, n=488 control) from 45 classrooms (range, 8–13 classrooms per school; average class size=22 students; range, 10–28 students per class) in four schools were enrolled. A total of 459 (92% of enrolled) students in the intervention group and 458 (94% of enrolled) in the control group were included in baseline (Time 1) data analyses, and 461 (92% of enrolled) students in the intervention group and 464 (95% of those enrolled) in the control group were included in follow-up (Time 2) data analyses.
Table 1 shows baseline characteristics of the study sample by intervention assignment. There were more boys in the intervention group, as compared to control (57% vs. 49%; p=0.01). There were more students in first grade in the intervention group, as compared to the control (61% vs. 49%). The proportion of overweight (BMI ≥85th percentile) students was also slightly higher in the control group, compared to the intervention group (48% vs. 42%; p=0.07). We attributed the differences in baseline characteristics across groups to the small number of clusters randomized in the trial.
Baseline Characteristics of the Study Participants by Group Allocation
SD, standard deviation.
Pedometer-Determined Physical Activity
There was no significant difference between the intervention and control group students in the mean number of steps (SD) taken at Time 1 (2581 [1284] intervention vs. 2476 [1180] control; p=0.71). However, at Time 2, intervention group students took significantly greater mean number of steps (SD) than controls (2839 [1262] vs. 2545 [1153]; p=0.0048) after adjusting for baseline activity level, grade, gender, recess, and PE class.
Subgroup analyses revealed that, at Time 1, intervention and control students did not differ significantly with respect to mean number of steps (SD) taken among students with BMI <85th percentile (2449 [957] vs. 2465 [894]; p=0.72) and students with BMI ≥85th percentile (2504 [1024] vs. 2534 [982]; p=0.92). At Time 2, intervention students took a greater mean number of steps than the control students in the BMI <85th percentile subgroup (2833 [984] vs. 2536 [819], respectively; p=0.019) and in the BMI ≥85th percentile subgroup (2911 [1004] vs. 2540 [903], respectively; p=0.0029) after adjusting for baseline activity level, grade, gender, recess, and PE.
Similar trends of increased step counts in the intervention group at Time 2 were observed in subgroups defined by gender and grade level (results not shown).
Process Measures
RE-AIM was used to describe the intervention's reach, effectiveness, adoption, implementation, and maintenance (Table 2). The quantitative aspects of
RE-AIM Dimensions, Definitions, and Applicability to the CHAM JAM Study
RE-AIM, framework of reach, effectiveness, adoption, implementation, and maintenance; CHAM JAM, the
Teacher Feedback About the CHAM JAM Intervention
RE-AIM, framework of reach, effectiveness, adoption, implementation, and maintenance; CHAM JAM, the
Discussion
We evaluated the effectiveness of CHAM JAM in a population-based feasibility study using a natural school environment with all kindergarten and first-grade classrooms participating. In this cluster RCT, we found that a classroom-based PA intervention, CHAM JAM, significantly increased PA levels in students attending intervention schools. The CHAM JAM intervention was equally effective across gender, grade level, and weight status.
We have previously reported low PA levels in urban minority kindergarten and first-grade students attending Bronx elementary schools. 2 The CHAM JAM intervention was developed to address increasing levels of obesity in minority children and low levels of PA in this population with an innovative approach to promote PA as an integral academic component. Few programs have been developed that target academic curriculum as a means to increase PA in US school children.22,23,39 Take 10! 39 and Physical Activity Across the Curriculum (PAAC), 23 which is based on Take 10!, are two such programs. Whereas these programs used an innovative approach by integrating PA into classroom academic lessons, they require hours of teacher in-services training and preparation to deliver interventions.23,39 The CHAM JAM lessons are self-explanatory and required no teacher training or preparation and are offered at a minimal cost of CD players and CDs.
Previously published studies describing effectiveness of the school-based interventions were prone to selection bias given that the evaluation took place in selected classrooms of teachers who agreed to participate22,23 and involved a convenience small sample of students.22,39 The studies enrolled students in grades 2 and above, and the majority of students were Caucasian.22–24,40 Although one study evaluated the Take 10! program in one predominantly Hispanic Chicago elementary school, it did not include a control group and did not measure program's impact on PA levels. 20 Another study evaluated the effects of a classroom-based PA program on fitness, classroom behavior, academic performance, and health outcomes, but not on PA levels. 24 Our study enrolled all kindergarten and first-grade classrooms from four study schools to assess impact of CHAM JAM on PA levels in a real-life setting using a rigorous cluster RCT design.
Evaluation of the Take 10!, program from which CHAM JAM was adapted, revealed that intervention students took only 142 more steps than controls during the school day, 41 as compared to 294 more steps found in our study. These results are comparable with the findings of the PAAC study (also based on Take 10!) that reported a 12% increase in PA.23,42 Evaluation of the Promoting Lifestyle Activity for Youth program using the treatment-control, postmeasure design revealed a mean difference of 1418 steps between the intervention and control groups of fourth-grade Arizona students. 40 However, this study evaluated PA over 23 hours and not during the school day. Thus, attributing the increase in steps to the program effectiveness, and not to another activity that children may have participated after school hours, is difficult.
Some research suggests that boys, older children, and those with lower BMI may be more physically active,43–45 but findings are inconsistent.2,44,46 To address baseline differences between the two groups with respect to age, gender, and BMI, we adjusted for these differences in data analyses. Other studies reported lower PA levels in obese/overweight children.10,11 We found no difference in PA levels between the two groups by weight status. Further research to evaluate the relationship between gender, age, and BMI on PA levels is needed.
New York City schools have been facing challenges meeting the New York State Education Department's (NYSED) Physical Education Regulations for students in elementary schools. 47 Bronx schools located in low-income communities have barriers related to lack of physical space and trained staff to meet the NYSED's PE requirements. In addition to the above-mentioned structural barriers, there is also a real barrier of school closing or phasing out owing to poor student academic performance. 48 To overcome these barriers, an intervention, such as CHAM JAM, that complements classroom curricula is needed. Finally, classroom PA programs may help meet state requirements for daily school-based PA given that many inner-city children are only physically active during school hours. 49
We found several barriers to intervention implementation that might have affected the size of the intervention effect. These barriers included time pressures to use the program three times a day, other competing demands, such as testing and academic assessments, days with PE, and class trips. Previous studies similarly found that lack of time was a main barrier to program implementation, 50 as well as other barriers related to varied school policies and procedures 51 and low retention rate. 52 Despite identified barriers, CHAM JAM was easy to implement because it requires no previous teaching training and both students and teachers enjoyed the program.
Our study had several limitations. The study was conducted in urban low-income public elementary schools in the Bronx, New York. The conclusions may not be generalizable to other schools in different communities. Pedometers, valid, reliable, and objective measures of children's PA in large, population-based studies,30–32 do not capture the intensity of PA or upper-body motion. Therefore, we cannot make conclusions about students' time spent in moderate-to-vigorous PA or upper-body activity during CHAM JAM. CHAM JAM involved upper-body activity, and the observed increase in PA may have been an underestimation of the true rise in PA. Pedometers captured only 1 school week of data at each point, which may not represent PA at other times; however, we conducted random unannounced direct observations of the classrooms and confirmed teachers' self-report of CHAM JAM use. We did not measure PA during individual CHAM JAM sessions. Finally, BMI was not assessed at 2 months postintervention because we did not expect to observe BMI changes at this time point. Future research assessing long-term impact on BMI z-scores will be conducted.
Conclusions
CHAM JAM is a promising program that increased PA among young elementary school students by combining academic concepts with PA components. It was well received by both teachers and students. Future research needs to address the effects of CHAM JAM on academic performance, health measures, and cost benefits. School-based PA interventions such as CHAM JAM may be effective in promoting PA outside of the classroom that may then translate into obesity prevention and reduced risk for other chronic diseases.
Footnotes
Acknowledgments
This research was funded by the Bauman Foundation. The funding agency had no role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; or preparation, review, or approval of the manuscript. The authors acknowledge the support from the NIH Eunice Kennedy Shriver National Institute of Child Health and Human Development (RC1 HD063607) for resources to expand the scope of evaluation. The authors also acknowledge the Diabetes Research and Training Center (P60DK20541) for salary support of Judith Wylie-Rosett for her work on this manuscript. The authors thank the Montefiore School Health Program for developing 25 classroom-based PA lessons used in this study and helping with data collection. (Clinical Trial Registration: ![]() Identifier: NCT00556569)
Identifier: NCT00556569)
Author Disclosure Statement
No competing financial interests exist.