
Abstract
Abstract
Background:
The Healthy Homes/Healthy Kids Preschool (HHHK-Preschool) pilot program is an obesity prevention intervention integrating pediatric care provider counseling and a phone-based program to prevent unhealthy weight gain among 2- to 4-year-old children at risk for obesity (BMI percentile between the 50th and 85th percentile and at least one overweight parent) or currently overweight (85th percentile ≤ BMI < 95th percentile). The aim of this randomized, controlled pilot study was to evaluate the feasibility, acceptability, and potential efficacy of the HHHK-Preschool intervention.
Methods:
Sixty parent-child dyads recruited from pediatric primary care clinics were randomized to: (1) the Busy Bodies/Better Bites Obesity Prevention Arm or the (2) Healthy Tots/Safe Spots safety/injury prevention Contact Control Arm. Baseline and 6-month data were collected, including measured height and weight, accelerometry, previous day dietary recalls, and parent surveys. Intervention process data (e.g., call completion) were also collected.
Results:
High intervention completion and satisfaction rates were observed. Although a statistically significant time by treatment interaction was not observed for BMI percentile or BMI z-score, post-hoc examination of baseline weight status as a moderator of treatment outcome showed that the Busy Bodies/Better Bites obesity prevention intervention appeared to be effective among children who were in the overweight category at baseline relative to those who were categorized as at risk for obesity (p = 0.04).
Conclusions:
HHHK-Preschool pilot study results support the feasibility, acceptability, and potential efficacy in already overweight children of a pediatric primary care–based obesity prevention intervention integrating brief provider counseling and parent-targeted phone coaching.
What's New:
Implementing pediatric primary care–based obesity interventions is challenging. Previous interventions have primarily involved in-person sessions, a barrier to sustained parent involvement. HHHK-preschool pilot study results suggest that integrating brief provider counseling and parent-targeted phone coaching is a promising approach.
Introduction
Obesity remains a significant public health problem given that one third of adults and 17% of youth in the United States are obese and rates do not appear to be declining. 1 Obesity prevention interventions that target young children and their families are a public health priority. As early as the preschool age years, excess body weight and adiposity predict overweight and obesity in adolescence and adulthood.2,3 The health consequences of obesity can emerge in childhood, and childhood adiposity is associated with poor health outcomes in adulthood. 4
Pediatric primary care is an important place to address obesity prevention given the influential role of pediatric primary care providers (PCPs) and their regular contact with families during well-child visits, particularly during the preschool years when annual visits are the standard of care.5,6 Universal obesity risk assessment and a staged approach to pediatric obesity intervention are recommended by the American Academy of Pediatrics (AAP). 6 Barriers such as time limitations,7,8 provider confidence and training, 9 and perceptions of parent resistance,7,10 however, make medical care settings a uniquely challenging environment in which to address obesity. Increased attention has been devoted to developing and evaluating pediatric primary care–based obesity interventions that address these barriers.11–23
A recent systematic review of pediatric primary care–based obesity prevention and treatment identified 31 completed trials, including four focused on preschool-age children. 24 Only one of the four trials, a randomized trial of a brief post-well-child visit behavioral counseling intervention, 25 focused on prevention and found no treatment group differences in BMI at 1 year follow-up. Two of the three treatment trials targeting preschool-age children were successful in impacting child weight outcomes. Quattrin and colleagues 16 evaluated the efficacy of a 6-month family-based program that involved clinic-based group meetings and phone calls. Intervention group children had greater BMI percentile and z-score differences at 3 and 6 months, compared to children in the informational control group. Stark and colleagues 23 evaluated the efficacy of a 6-month clinic-based group intervention accompanied by home visits. Intervention group children showed a significantly lower BMI z-score and percentile at 6- and 12-month follow-up relative to comparison group children. These findings, along with results from trials focused on older children, suggest that more-intensive interventions are more effective. 24 However, interventions that augment well-child visits with additional office visits may pose a barrier to sustained involvement. 13 Exploring alternative modalities, such as phone-based coaching, is warranted. Phone coaching has been used as a viable option in the context of adult weight management26,27 and as an adjunct to in-person visits in childhood obesity interventions, 16 but has not been extensively evaluated as an option for pediatric primary care–based obesity prevention. Phone coaching may be particularly useful and convenient for parents of young children who may be dealing with child care issues and other logistical challenges associated with family and work schedules. 28
The Healthy Homes/Healthy Kids Preschool (HHHK-Preschool) pilot evaluated the feasibility, acceptability, and potential efficacy of a primary care–based obesity prevention intervention integrating pediatric care provider counseling and phone coaching to prevent unhealthy weight gain among preschool-age children at risk for obesity or currently overweight. The pilot study aim was to recruit and randomize 60 parent-child dyads to: (1) the Busy Bodies/Better Bites Obesity Prevention Arm or the (2) Healthy Tots/Safe Spots safety/injury prevention Contact Control Arm. Intervention feasibility, acceptability, and exploratory impact on BMI percentile and z-score, dietary intake, physical activity (PA), and screen time are presented here.
Methods
Participants
Parent-child dyads were recruited through 20 clinics in the greater Minneapolis–St. Paul area. Candidates included children identified through electronic medical records who: (1) had a 2- to 4-year-old well-child visit scheduled and (2) a previous BMI or weight-for-height percentile between 50th and 95th for age and sex. 29 Figure 1 depicts a modified CONSORT diagram. PCPs of identified children were consulted by secure electronic medical record (EMR) messaging. Then, unless the provider indicated a reason why the child should not be included, a study invitation letter was sent to parents. A subsequent phone call assessed interest and preliminary eligibility, confirmed in a home visit. Eligibility criteria included: (1) child at risk for obesity (BMI percentile between 50th and 85th with one overweight parent) or overweight (85th percentile ≤ BMI < 95th percentile); (2) English-speaking parent; and (3) child not using a steroid medication for more than 1 month. Consent forms were reviewed with and signed by the parent. This study was approved by the HealthPartners Institutional Review Board and registered on ClinicalTrials.Gov before recruitment (NCT01080885).
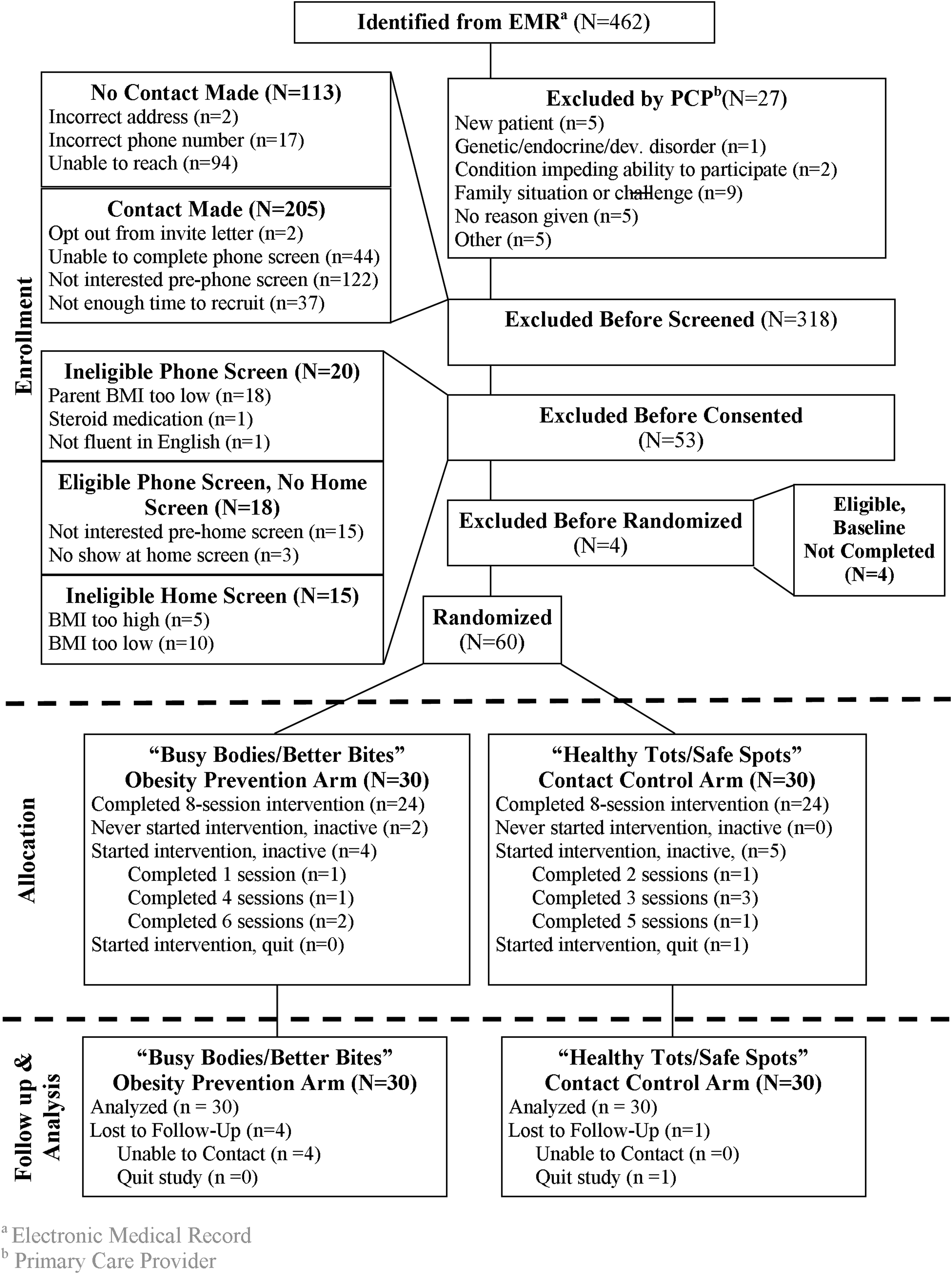
Healthy Homes/Healthy Kids—Preschool modified CONSORT diagram.
A total of 462 children were identified and 435 were sent an invitation letter (Fig. 1). One quarter of invited candidates could not be reached and another 45% did not complete eligibility screening. Phone screen eligibility was assessed in 117 dyads; 20 were ineligible. An additional 15 candidates were ineligible based on home screen–measured BMI; four consented families did not complete baseline measurement. Sixty parent-child dyads were randomized equally to the Busy Bodies/Better Bites Obesity Prevention and the Healthy Tots/Safe Spots Contact Control arms.
Interventions
The pilot intervention programs included a brief pediatric primary care component and eight phone coaching sessions. Participants received pediatric PCP counseling during their well-child visit to raise parental awareness of their child's obesity risk and provide messaging regarding obesity and injury prevention behaviors. Providers used the HHHK-Preschool flip chart that highlighted study messages, and parents received a pamphlet with their child's BMI percentile and obesity and injury prevention tips. Pediatric PCPs attended a 1-hour study training during which the study and provider intervention component was reviewed and questions were addressed. A more-intensive training component was not feasible given provider time constraints.
The eight-session phone coaching program focused on healthy eating and PA (Busy Bodies/Better Bites) or safety and injury prevention (Healthy Tots/Safe Spots). After the well-child visit, parents received a randomized group assignment notification letter, the associated workbook, and Busy Bag or Safety Tote. The Busy Bag included: a child-focused book on television (TV) habits, activity and dinner table conversation idea cards, portion placement and plate, a kid-friendly, healthy recipe pamphlet, small plastic cones, sidewalk chalk, stickers, a child-focused dance music CD, and an inflatable beach ball. The Safety Tote included a similar number of items relevant to the safety and injury prevention topics (e.g., travel-size sunscreen or fire safety book).
The first phone coaching session was scheduled and 15- to 30-minute calls informed by social ecological models, 30 social cognitive theory, 31 and motivational interviewing 32 were held biweekly. Biweekly sessions were chosen to provide an opportunity for parents to work on goals set during the phone session and to minimize the time burden of participating. Busy Bodies/Better Bites goals 6 included home-based strategies to: (1) reduce screen time; (2) decrease sweetened beverage availability; (3) increase PA; and (4) increase availability of lower-fat, lower-calorie meals and snacks. Healthy Tots/Safe Spots goals included: (1) distracted driving reduction; (2) fall prevention; (3) fire safety; (4) poison control; and (5) sun protection. During the first session, parents described how their family was currently doing in each area and identified desired changes. Coaches worked with parents to address behavior change areas in order of parent preference, setting goals and discussing challenges and successes at subsequent sessions. An overview of behavior change techniques and strategies was also given during the first session and behavioral adherence strategies adapted from Levy33,34 were utilized to facilitate goal attainment.
The phone coaching was conducted by experienced interventionists with bachelor's or master's degrees in health behavior, nutrition, or exercise science. Phone coaches received study protocol and behavioral adherence strategy training and ongoing supervision. Phone coaches completed a self-assessment of session fidelity (e.g., use of behavioral adherence strategies and time spent discussing specific target areas) after each session. Phone sessions were audio recorded, and recordings were utilized during supervision sessions and subsequently coded by independent raters to provide a more in-depth examination of fidelity. 35
Measures
Study data included intervention feasibility and acceptability measures and data collected at baseline and 6 months.
Intervention Feasibility and Acceptability
Provider adherence
Well-child visit protocol adherence was assessed by phone survey with parents 1–2 weeks post-well-child visit. Parents reported whether their provider talked about BMI percentile, whether they received the HHHK pamphlet, and whether the provider addressed specific PA, sedentary behavior, healthy eating, and safety/injury prevention issues.
Provider feedback
Feedback was obtained by survey after providers completed three HHHK well-child visits. The survey assessed comfort level, addressing BMI percentile and obesity and safety/injury prevention issues with parents, as well as study training and resource usefulness.
Parent participation and satisfaction
Call completion and intervention satisfaction were assessed on the 6-month survey.
Home Visit Data Collection
Child body mass index percentile, body mass index z-score, and parent body mass index
Child and parent height and weight were measured during home visits using a Seca 876 flat scale and Seca 217 stadiometer (Seca Corp., Hanover, MD). Weight and height were measured twice; if the first two measurements differed by more than 0.2 kg for weight or 1.0 cm for height, a third measurement was taken. Measurements were averaged and child BMI percentile, BMI z-score, and parent BMI (kg/m2) were computed.
Child dietary intake
A multipass 24-hour dietary recall was administered by staff trained and certified to use the Nutrition Data System for Research software versions 2009, 2010, and 2011 (NDSR; Nutrition Coordinating Center, University of Minnesota, Minneapolis, MN). Recalls were analyzed using NDSR version 2011 software to estimate total energy intake, percent calories from fat, servings of fruits, vegetables, and sugar-sweetened beverage intake.
Diet-Related Variables
Family meals
Parents reported the number of times all, or most, of the family living at home had dinner together during the past week. 36 Assessment of family meal frequency was included given the focus on household food environment change.
Fast food patterns
Parents reported the number of times during the past week their child ate something from a fast food restaurant. 37
Home food availability
Household food availability was assessed across five categories (fruits, vegetables, salty snacks, beverages, and sweet snacks). Items were adapted from the Food Frequency Questionnaire. 38 Participants selected the items available in their home within the last week. A count variable was created for each food and beverage category. 39
Physical Activity and Television Time
Accelerometry
Child PA was measured using ActiGraph GT3X accelerometers (ActiGraph LLC, Pensacola, FL). Children were asked to wear the accelerometers for 7 full days during waking hours, except during water activities. The devices were placed on elastic belts, fitted on the right hip, and initialized to record data in 5-second epochs. Children were included in PA data analyses if they had at least 4 valid monitoring days, defined as 6 or more hours of wear time. To estimate minutes spent in moderate-to-vigorous physical activity (MVPA) and total physical activity (Total PA), data were aggregated into 1-minute epochs; cut points were defined using the Pate and colleagues equations. 40
Television viewing
Parents reported the amount of time their child watches TV on an average weekday and weekend day 41 ; items were dichotomized to classify children as meeting (≤2 hours of TV per day) or exceeding (>2 hours per day) AAP guidelines. 42
Activity-Related Variables
Parent support for child physical activity
Parental support for child PA was assessed with four items adapted from Trost and colleagues. 43 Parents rated the frequency during the past week that they engaged in the supportive behaviors (e.g., engaged in PA or played sports with their child). Ratings were made on a 0–4 Likert scale (“none,” “once,” “sometimes,” “almost daily,” or “daily”). The Cronbach's alpha coefficient was 0.77.
Parent self-efficacy for limiting media use
Two items adapted from Taveras and colleagues 44 assessed parental confidence in their ability to limit their child's media viewing and remove TV from their child's bedroom.
Statistical Analysis
Study population descriptive characteristics and intervention feasibility and acceptability are presented. To address exploratory aims regarding Busy Bodies/Better Bites Obesity Prevention intervention efficacy, the treatment by time interaction was quantified using a general or generalized (for binary outcomes) linear mixed-model approach where treatment (Busy Bodies/Better Bites Obesity Prevention, Healthy Tots/Safe Spots Contact Control) was a fixed between-subjects effect and time was a fixed within-subjects effect. Separate mixed models that treated baseline BMI (50%–84%; ≥85%) or sex (male, female) as fixed between-subjects effects were estimated to assess whether the treatment by time effect was moderated by baseline BMI. Within each family of secondary outcomes, the generalized Holm procedure limited the family-wise error rate (FWER) to falsely reject one null hypothesis at α = 0.05. 45
Results
Baseline characteristics are reported in Table 1. Forty-five percent of children were female, and 92% of participating parents were female. The majority of participants were white and non-Hispanic. Average child BMI percentile was 80.1.
Baseline Characteristics by Treatment Arm
M, mean; SD, standard deviation.
Intervention Feasibility and Acceptability
Well-child visit intervention component
Parents reported that 78% of providers discussed BMI percentile. The majority of parents (87%) received the HHHK pamphlet, but less than half (44%) reported that their provider used the HHHK flipchart. The most frequently discussed obesity prevention topics included fruit and vegetable intake (27%), PA (24%), junk food, including sweetened beverages (11%), and media use (7%). Fewer parents reported that the provider discussed family meals (5%), eating breakfast (4%), and eating out at restaurants (0%). Approximately half (53%) of the parents reported that talking about healthy eating and PA made them think about changes they wanted to make at home.
The majority of providers reported that the study training was helpful (88%) and that they were comfortable addressing healthy eating/PA (96%) and BMI (93%). Approximately two thirds reported that the HHHK pamphlet (71%) and flipchart (68%) were useful for communicating with families, and the average amount of time spent on these topics during well-child visits reported by providers was 5.8 minutes.
Busy Bodies/Better Bites and Healthy Tots/Safe Spots phone coaching component
Figure 1 shows that 80% of participants in both arms completed the eight-session intervention. On average, sessions were 23 (standard deviation [SD] = 9) minutes in the Busy Bodies/Better Bites arm and 21 (SD = 9) minutes in the Healthy Tots/Safe Spots arm. Seventy-two percent of Busy Bodies/Better Bites parents reported that phone coaching helped their family improve or maintain healthy behaviors.
Body Mass Index Outcomes
Mean baseline and 6-month BMI percentiles and BMI z-scores are presented by treatment group in Table 2. There was no statistically significant treatment by time effect on BMI percentile (p = 0.64) or BMI z-score at 6 months (p = 0.89). However, as shown in Figure 2, baseline child weight status moderated the time by treatment effect on BMI percentile (p = 0.04). Overweight children randomized to the Busy Bodies/Better Bites Obesity Prevention arm showed marginally greater 6-month reductions in BMI percentile, compared to overweight children randomized to the Healthy Tots/Safe Spots Contact Control arm (p = 0.06), whereas change in BMI percentile from baseline to 6 months did not differ as a function of group assignment for children in the at risk for becoming overweight category (p = 0.15). Child weight status also moderated the time by treatment effect on BMI z-score (p = 0.02). Overweight children randomized to the Busy Bodies/Better Bites Obesity Prevention arm showed greater 6-month reductions in BMI z-score, compared to overweight children randomized to the Healthy Tots/Safe Spots Contact Control arm (p = 0.02). BMI z-score change from baseline to 6 months did not differ as a function of group assignment for children in the at risk for becoming overweight category (p = 0.09)

Treatment by time effect moderated by baseline weight status.
Baseline and 6-Month Characteristics by Treatment Arm
M, mean; SD, standard deviation; kcal, kilocalories; TV, television; MVPA, moderate-to-vigorous physical activity; PA, physical activity.
Dietary Intake and Diet-Related Outcomes
The treatment by time interaction for total energy intake was not significant (p = 0.84). There was a marginally significant effect on percent energy from fat, which decreased more among Busy Bodies/Better Bites children (31–27%) compared to Healthy Spots/Safe Spots children (30–29%).
Physical Activity, Television Time, and Activity-Related Outcomes
Accelerometer compliance was unequally distributed between treatment groups. Two thirds of Busy Bodies/Better Bites participants had valid baseline accelerometry data, compared to 87% of Healthy Spots/Safe Spots participants, and only 57% of Busy Bodies/Better Bites participants, compared to 73% of Healthy Spots/Safe Spots participants, had valid 6-month accelerometry data. Children with valid 6-month accelerometry data in the Busy Bodies/Better Bites Obesity Prevention arm (mean BMI percentile = 84; SD = 8.7) tended to be heavier, compared to Healthy Spots/Safe Spots children with valid accelerometry data (mean BMI percentile = 76; SD = 17; p < 0.11). As shown in Table 2, the treatment by time interaction for accelerometry-measured MVPA was significant, such that MVPA of Busy Bodies/Better Bites Obesity Prevention participants was stable from baseline to 6 months and MVPA among Healthy Spots/Safe Spots participants increased. A similar pattern approaching statistical significance was observed for total PA.
The trend toward improvement in efficacy for removing the TV from their child's room among parents in the Busy Bodies/Better Bites arm (p = 0.04) falls short of significance (FWER pcrit = 0.017).
Discussion
The HHHK-Preschool pilot study primary aims were to evaluate the feasibility and acceptability of an obesity prevention intervention integrating parent-targeted pediatric PCP counseling and phone coaching. Pediatric primary care recruitment is challenging 13 ; however, by using a proactive outreach system that minimized clinician burden, we successfully recruited 60 parent-child dyads. Pediatric primary care well-child visit implementation was also successful. The majority of parents reported that they received the HHHK pamphlet and that their provider discussed BMI percentile and associated issues. Moreover, parent-targeted phone coaching was well received, as indicated by call completion rates and satisfaction measures.
Given the small sample size and short pilot study duration, we did not anticipate and did not find a statistically significant time by treatment effect on BMI. However, post-hoc examination of baseline weight status as a treatment outcome moderator showed that the Busy Bodies/Better Bites intervention was effective among children who were in the overweight category at baseline relative to those who were at risk for obesity. Previous pediatric primary care–based obesity intervention studies conducted in this age group to date have only focused on children who are already overweight or obese.16,19,23 Of interest, Quattrin and colleagues 16 reported that intervention group children had greater BMI percentile and z-BMI decreases at 3 and 6 months, compared to information control condition children (p < 0.0021), and that children with greater baseline BMI percentile had a greater BMI percentile decrease over time (p = 0.02). Preschool-age children who are already overweight or obese appear to benefit the most from parent-targeted obesity interventions. Further intervention strategy development to prevent at-risk children from becoming overweight or obese is warranted. Parents of preschool-age children misclassify their child's weight status,46,47 and obesity prevention may not be a salient issue. Strategies emphasizing the connections between obesity prevention behaviors and broader child developmental outcomes may be a promising approach. 48
The HHHK-Preschool pilot study offers insights to strengthen pediatric primary care–based interventions. Phone coaching call content was parent driven, with coaches guiding parents to identify their priority behavioral targets. Behavioral targets chosen by parents, however, may not necessarily have been the areas that would substantively impact healthy child energy balance. Additionally, parent-reported data indicated that although many pediatric care providers used the HHHK-Preschool intervention tools and discussed relevant content information, there is room for improvement given the small percent of parents reporting provider discussion of key obesity prevention behavior targets. These results, however, should be interpreted with caution in light of the fact that provider adherence was parent-reported 1–2 weeks post-well-child visit, rather than objectively measured during the well-child visit, and may be subject to response bias.
Study findings should be interpreted considering several limitations, including the relatively homogeneous sample with respect to race/ethnicity and socioeconomic status, use of a single 24-hour diet recall to estimate dietary intake, and suboptimal accelerometry compliance rates, which varied by treatment group. Moreover, multiple statistical comparisons performed increased the likelihood of type 1 error.
Conclusions
Despite these limitations, the study findings support the feasibility and potential efficacy of pediatric primary care–based interventions to promote healthy growth in preschool-age children, who are already overweight. The HHHK-Preschool pilot study highlights next steps for optimizing and broadening the reach of obesity prevention interventions, including: (1) developing strategies to engage parents who may not view obesity prevention as a salient issue; (2) supporting pediatric care providers in their efforts to address obesity prevention; and (3) systematically examining the optimal modality and timing of intervention delivery, including how this may vary as a function of child and family characteristics, such as child weight status.
Footnotes
Acknowledgments
The project described was supported by grant numbers A1R21DK078239 (principal investigator [PI]: Sherwood), P30DK050456 (PI: Levine), and P30DK092924 (PI: Schmittdiel) from the National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK). The content is solely the responsibility of the authors and does not necessarily represent the official views of the NIDDK or the NIH.
Author Disclosure Statement
No competing financial interests exist.