
Abstract
Abstract
Background:
Passive smoke exposure (PSE) may be a risk factor for childhood overweight and obesity and is associated with worse neurocognitive development, cognition, and sleep in children. The purpose of the study is to examine the effects of PSE on adiposity, cognition, and sleep in overweight and obese children using an objective measure of PSE.
Methods:
Overweight or obese children (n = 222) aged 7–11 (9.4 ± 1.1 years; 58% black; 58% female; 85% obese) were recruited from schools near Augusta, Georgia, over the course of the school year from 2003–2006 for a clinical trial, with data analyzed in 2009–2010. Passive smoke exposure was measured with plasma cotinine. Health, cognitive, and sleep measures and parent report of smoke exposure were obtained.
Results:
Overweight and obese children with PSE had greater overall and central adiposity than nonexposed overweight and obese children (p < 0.03). However, PSE was unrelated to prediabetes, insulin resistance, or visceral fat. PSE was linked to poorer cognitive scores (p < 0.04) independent of adiposity, but was not related to sleep-disordered breathing.
Conclusions:
PSE is associated with fatness and poorer cognition in children. Tailored interventions that target multiple health risk factors including nutrition, physical activity, and tobacco use in children and families are needed to prevent adverse health outcomes related to tobacco use and obesity.
Introduction
Tobacco use remains the leading cause of premature and preventable deaths worldwide, and there is no safe level of exposure to tobacco smoke.1,2 Of the nearly six million premature deaths caused by tobacco use annually worldwide, more than 480,000 occurred in the US alone, with nearly 42,000 of those deaths in nonsmokers due to passive smoke exposure (PSE). 1 Over 40% of children have at least one parent who smokes and, therefore, suffer from PSE. 2
Overweight and obesity is another major health concern worldwide, in both adults and children. Obesity rates in US children have reached epidemic proportions.3,4 Childhood obesity is associated with numerous potential adverse health outcomes, such as type 2 diabetes and cardiovascular disease risk. 5 Visceral fat has been shown to be more indicative of cardiometabolic risk in obese children than subcutaneous fat. 6
Weitzman and colleagues 7 demonstrated that PSE may be a risk factor for overweight and obesity, and metabolic syndrome among adolescents (12–19 years). Some research that examined the relationship between PSE and obesity has reported inconclusive results, 8 while other researchers have found a relationship between PSE and obesity, primarily by using maternal self-report measures.9–11 Studies conducted using cotinine measures for smoke exposure in children have found associations of PSE with worse cognition and sleep.12–14 Another study, which measured PSE through maternal self-report, found an association between PSE and neuropsychological deficits in adolescents. 15 Yet another study using parent report had inconclusive results on postnatal PSE and neurodevelopment. 16
The differences in findings between cotinine-measure PSE and self-report measures may be due to different measurements. 17 Thus, to clarify these relationships, we examined associations between both an objective measure of the child's PSE (cotinine) and parent reports of smokers in the home, with precise measurements of adiposity and related health risks, cognitive tests, and a measure of sleep habits to assess the relationship between PSE and children's health.
Methods
Participants
Overweight or obese children (n = 222) aged 7–11 (9.4 ± 1.1 years; 58% black; 58% female; 85% obese) were recruited from public schools near Augusta, Georgia, for a clinical trial between 2003–2006. 17 The study was advertised via presentations and flyers distributed at 15 elementary schools in Richmond and Columbia counties in Georgia and Aiken county in South Carolina. Inclusion criteria were white or black race, aged 7–11 years, overweight or obese (≥85th percentile BMI; calculated as weight in kg divided by height in m2), 18 sedentary (no regular physical activity program >1 hour per week), no medical condition or medications that would affect study results or limit physical activity, and ability to provide a fasting blood sample at baseline. Specific details regarding recruitment and procedures were previously reported. 17
Recruitment efforts resulted in 840 children being assessed for eligibility in the trial, with 222 children randomized and included in analyses. Baseline measures from the trial are reported here, and were analyzed from 2009–2010. The parent (i.e., primary caregiver) reported their own level of education (1 = less than 7th grade, 2 = 8th or 9th, 3 = 10th or 11th, 4 = high school graduate, 5 = some college, 6 = college graduate, 7 = postgraduate) and their child's demographic characteristics. The study was approved by the institutional review board of the Medical College of Georgia, and free and informed consent and assent were obtained orally and in writing from parents or guardians and from children.
Measures
Smoke exposure
Passive smoke exposure was measured with plasma cotinine assay and defined as exposed if the subject had a cotinine level ≥0.05 ng/mL, and not exposed if the subject had a cotinine level <0.05 ng/mL. 19 No subject had a cotinine level that would indicate that they were a smoker (≥ 15 ng/mL). Parent report of the number of smokers in the household was also obtained.
Health measures
Anthropometrics were measured at least twice until consistent measures were obtained. Waist circumference was measured using a Gulick fiberglass tape with tension gauge (M-22C, Creative Health Products, Plymouth, MI). BMI percentile and z scores were determined from body weight (in shorts and t-shirt; Detecto) and height (without shoes; HR100; Tanita). BMI z-score ≥1.04 indicates overweight status (≥85th percentile), and a score ≥1.65 indicates obesity (≥ 95th percentile). Dual-energy x-ray absorptiometry (Hologic QDR- 4500W) of the whole body was used to measure percent body fat. Abdominal visceral and subcutaneous fat content was measured with magnetic resonance imaging. The oral glucose tolerance test was used to measure diabetes risk [area under the curve (AUC) and fasting levels of insulin and glucose]. Prediabetes status was determined by impaired fasting glucose (100–125 mg/dL) and/or impaired glucose tolerance (two-hour postchallenge glucose 140–199 mg/dL).
Cognitive assessment
A standardized cognitive assessment, the Cognitive Assessment System 20 was used as previously described. 21 The Cognitive Assessment System yields smaller race and ethnic differences than traditional intelligence tests, making it more appropriate for the assessment of disadvantaged groups. 22 It provides four scales each comprised of three subtests. The Planning scale measures executive function (i.e., strategy generation and application, self-regulation, intentionality, and utilization of knowledge). The Attention scale measures focused, selective cognitive activity and resistance to distraction. The Simultaneous scale includes spatial and logical questions with nonverbal and verbal content. The Successive scale requires analysis or recall of stimuli arranged in sequence, and formation of sounds in order. An overall measure of cognitive function, or Full Scale score, is derived from the scores on these four scales. Standard scores are reported (normative mean = 100, SD = 15).
Sleep-disordered breathing symptoms
Parent reports of participant sleep behaviors were obtained using the Pediatric Sleep Questionnaire, which has been validated against polysomnography in children, 23 as previously described. 24 Scores are the proportion of items answered “yes” and range 0–1. Higher scores indicate more symptoms endorsed, with a score ≥0.33 on Sleep-Related Disordered Breathing, a summary scale, considered clinically significant. Subscales include Snoring, Sleepiness, Behavior, and Other.
Lifestyle variables
Participants answered questions about the frequency of moderate and vigorous exercise over the course of one week.25,26 Moderate physical activity (days per week) was assessed by the question, “On how many of the past 7 days did you participate in physical activity for at least 30 minutes that did not make you sweat or breathe hard, such as fast walking, slow bicycling, skating, pushing a lawn mower, or mopping floors?” Vigorous physical activity (days per week) was assessed by the question, “On how many of the past 7 days did you exercise or participate in physical activity for at least 20 minutes that made you sweat or breathe hard, such as bicycling, fast dancing, or similar aerobic activities?” Dietary energy intake was assessed through three 24-hour diet recalls with food records that provided mean daily energy intake (kilocalories per day; Nutrition Data System for Research software, version 2006). Prior to recall, children and parents were shown how to maintain a diet record using food models, portion booklets, and containers for estimating serving size.
Statistical Analyses
All statistical analyses were performed using SAS (SAS version 9.1.3; SAS Institute Inc., Cary, NC). Statistical significance was assessed using an alpha level of 0.05 unless otherwise noted. The associations of passive smoke exposure with health measures were tested, controlling for recruitment cohort, race, sex, age, and parent education. Cohort, race, and sex were included because they were design variables in the trial, and parent education was included as a proxy to avoid confounding by socioeconomic status. Age was included as a covariate for all models except BMI z-score and cognitive measures, which adjust for age. Lifestyle variables were included as covariates if they were related to the cotinine measure, or adiposity measures. ANCOVA models were used on continuous outcomes (waist circumference, BMI, BMI z-score, visceral fat, subcutaneous fat, percent body fat, fasting glucose, AUC glucose, fasting insulin, AUC insulin, cognitive and sleep measures) and logistic regression on prediabetes status (i.e., impaired fasting glucose, impaired glucose tolerance, and both conditions). Results of covariates in the models where PSE was significant were reported for comparison of effect size with PSE results. Where models for nonadiposity outcomes showed a significant association with PSE, percent body fat was further adjusted to evaluate independence of these effects.
Results
Characteristics of the sample are presented in Table 1 by PSE status, with univariate comparisons by this condition. As expected, cotinine levels and parent reports of smokers in the household were different between exposure groups (p < 0.001). Most measures of adiposity were higher in the smoke-exposed group, but no differences were apparent for lifestyle, sleep, or insulin-glucose measures, with the exception of the number of children with prediabetes. The insulin-glucose measures were slightly lower in the smoke-exposed group. No significant correlations were observed for lifestyle variables with cotinine level, anthropometrics, or percent body fat.
Participant Characteristics a
Total n = 222 from Augusta, Georgia, 2003–2006; mean ± SD or %.
Differences for PSE from t-test and chi-square analyses shown.
Parent education: parent report of educational attainment: 1 = 7 or fewer years of school; 2 = 8–9 years of school; 3 = 10–11 years of school; 4 = 12 years of school; 5 = partial college; 6 = college graduate; 7 = postgraduate.
p < 0.05.
p < 0.01.
p < 0.001.
ANCOVA models revealed that controlling for covariates, overweight and obese children who had been exposed to passive smoke, as measured by plasma cotinine levels, had greater overall and central adiposity (waist circumference, p = 0.02; BMI z-score, p = 0.002; percent body fat, p = 0.02) than their nonexposed peers (see Fig. 1A-C). However, no significant differences were found for PSE on BMI, visceral or subcutaneous fat, glucose and insulin measures, or physical activity and diet. PSE was also linked to poorer cognitive scores, as shown in Figure 2, with increased cotinine levels showing lower scores (4–6 points) in the children's Planning (p = 0.04), Attention (p = 0.02), Simultaneous (p = 0.001), and Successive (p = 0.01) cognitive skills, while no differences were shown for any of the sleep measures. Logistic regression analyses revealed no significant associations between PSE and prediabetes status. Sex was a significant covariate for percent body fat (p < 0.0001) and Attention (p = 0.003). Race was a significant covariate for BMI z-score (p = 0.002). Parent education was a significant covariate only for Planning (p = 0.02). Further adjusting the cognitive models for percent body fat did not substantially alter findings; it very slightly weakened the association of PSE with Planning (p = 0.07).
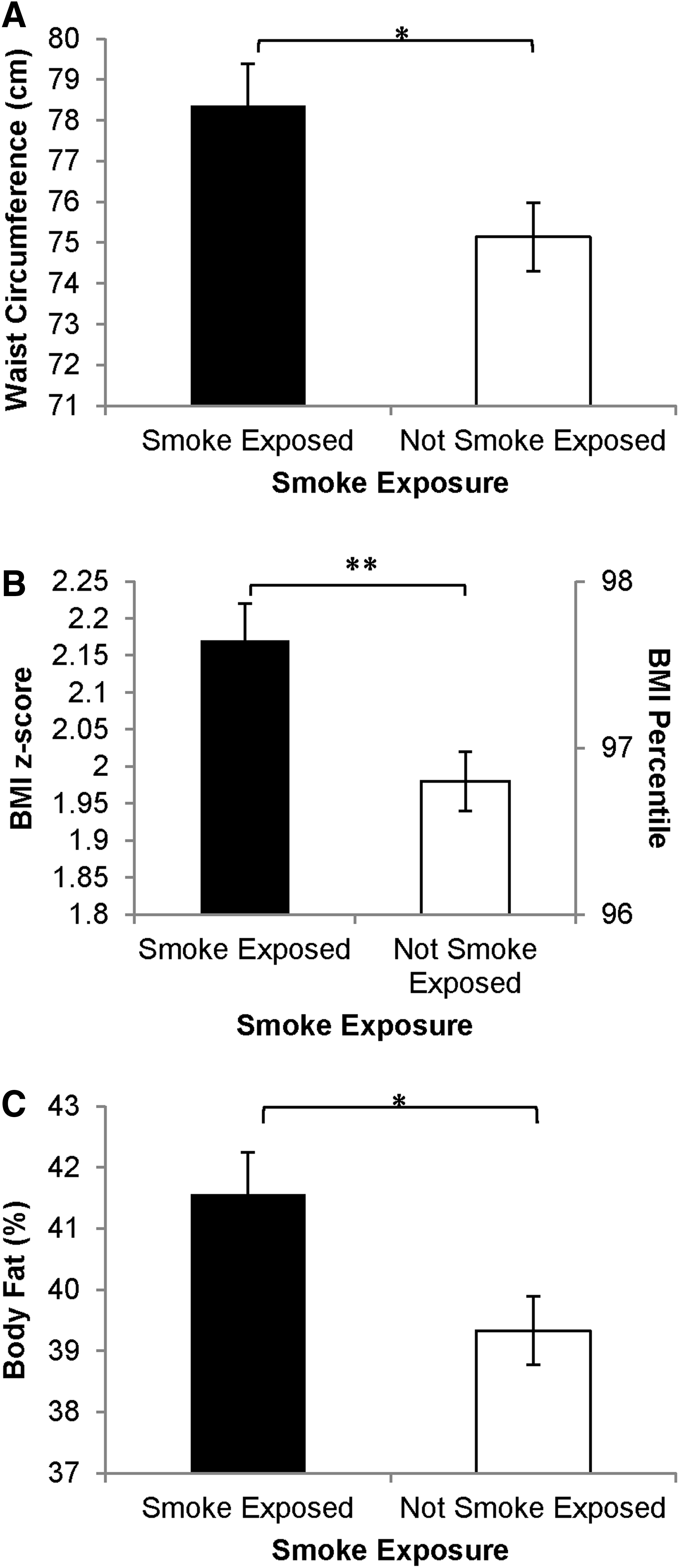
Smoke exposure and obesity measures. Means and standard error bars are shown. Panel A shows waist circumference, Panel B shows BMI z-score, and Panel C shows percent body fat via dual-energy x-ray absorptiometry. Asterisks indicate that children exposed to tobacco smoke were more obese compared to those that were not exposed. *p < 0.05. **p < 0.01.
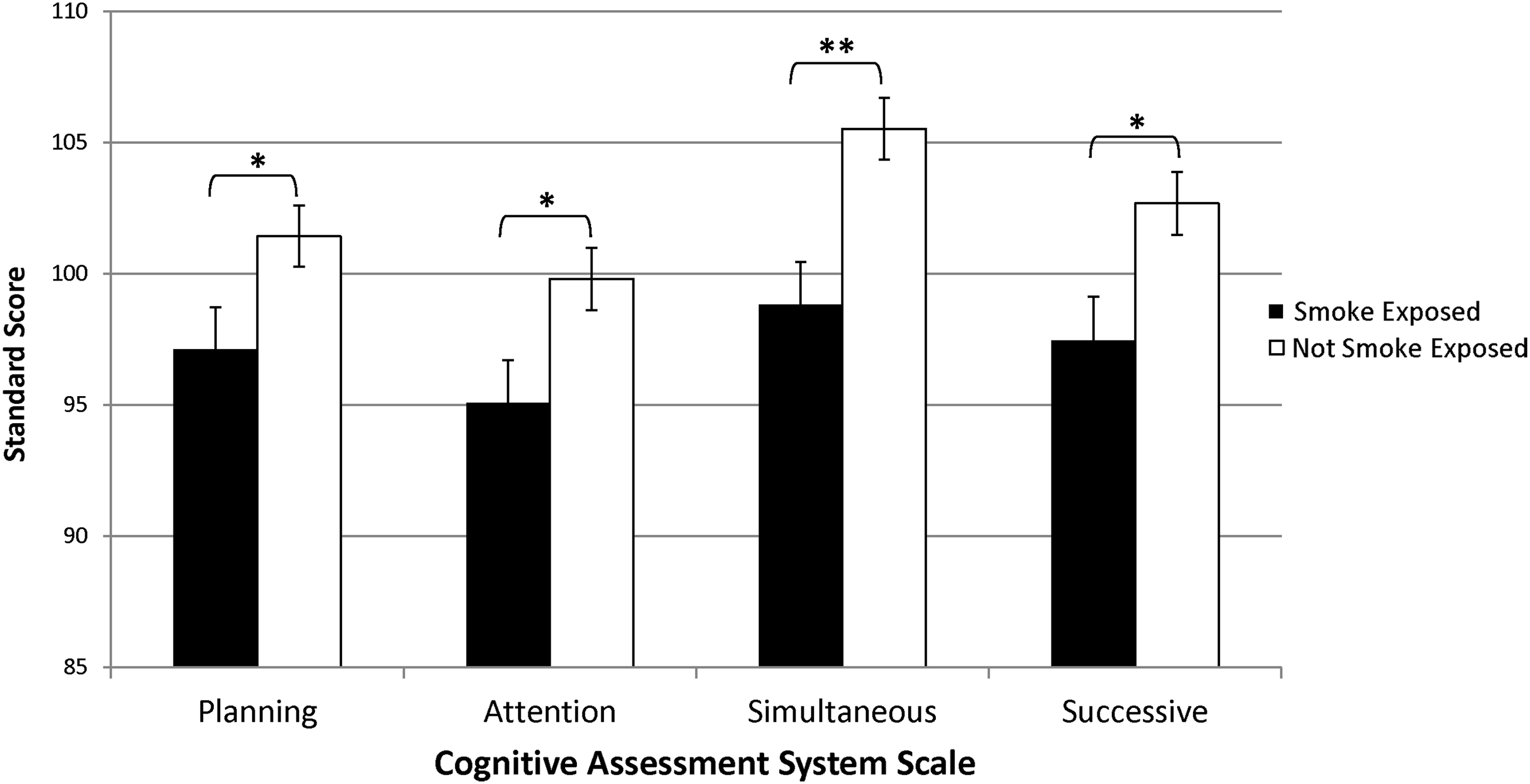
Smoke exposure and cognitive performance. Means and standard error bars are shown. Asterisks indicate that children exposed to tobacco smoke scored poorly on cognitive tests compared to those that were not exposed. *p < 0.05. **p < 0.01.
Parent-report PSE data were also examined to permit comparison of the results of the current study to those found in previous research. A cross-tabulation of PSE status on these measures is shown in Table 2. Cohen's κ showed fair agreement between cotinine-measured and parent-reported PSE (κ = 0.346, p < 0.001; parent report was 69% sensitive, 71% specific). 27 Parent-report data in similar ANCOVA models showed differences in waist circumference (p = 0.02) and a trend for greater percent body fat and sleepiness (p's = 0.05), as well as differences in cognitive scores for Attention (p = 0.02), and for sleep-disordered breathing (p = 0.01) and behavior (p = 0.001) problems. No differences were found for other health, cognitive, or sleep measures.
Cotinine Level versus Parent-Reported Smoke Exposure in the Home
Discussion
This study examined the association of PSE, as measured by cotinine levels, with obesity, related health measures, and cognition in a community sample of black and white overweight and obese children. It was found that overweight and obese children who had been exposed to passive smoke had greater overall and central adiposity than nonexposed peers. Our study used definitive measures and found an association between PSE and several measures of adiposity, including waist circumference, which is a clinical indicator of risk for obesity-related diseases.28–34 However, no association was detected in this multiethnic sample with MRI-measured subcutaneous or visceral fat depots, nor with detailed measures of prediabetes and insulin resistance. PSE was also linked to poorer cognitive scores, independent of socioeconomic status and adiposity, yet not to sleep-disordered breathing. These associations with PSE were more robust and consistent than the effects of demographics in those models.
Although we confirmed the link between PSE and adiposity,9–11 no significant relationships were found for PSE with prediabetes status (impaired fasting glucose and/or impaired glucose tolerance), fasting or postchallenge (data not shown) glucose or insulin levels, dyslipidemia (data not shown), or visceral or subcutaneous abdominal fat in the children in the current study. This stands in contrast to the Weitzman et al. findings (who also used cotinine to measure PSE) who showed that PSE may be a risk factor for not only obesity, but also metabolic syndrome in adolescents, particularly dyslipidemia (high triglycerides, low high-density lipoprotein levels); however, similar to our findings, that report did not find a link with impaired fasting glucose. 7 Together, these findings suggest that PSE may have more effect on the amount of body fat than metabolic dysfunction at this age. The current study focused on younger, overweight and obese children, and had a larger percentage of children with prediabetes (32%), as well as more detailed measures of overall adiposity (DEXA), visceral and subcutaneous abdominal fat (MRI), and oral glucose tolerance testing than the Weitzman study. 7 The current study included a larger proportion of black children, who are less prone to dyslipidemia than white or Hispanic children. 35
In this study there was only fair agreement between cotinine-measured and parent-reported smoke exposure. As shown in Table 2, PSE status based on cotinine levels can be quite different from parental reports of smoke exposure, indicating a lower sensitivity and specificity of self-report data versus biological measurements of exposure. This may explain inconsistent results in studies with different measures of PSE. For example, in terms of adiposity, parent-reported PSE showed fewer differences than those shown by cotinine-measured PSE in this study, with the only association based on parent report being with waist circumference. In this case, the cotinine-measured PSE status was more sensitive to the associations with adiposity. Similarly, fewer differences were found on measures of cognition, with parent-report data showing differences only for Attention, while cotinine-measured PSE showed associations with all four cognitive measures. However, our parent-report data generated a false positive finding for sleep disturbances. Parent-report data showed significant differences for sleep-disordered breathing and behavior problems, whereas cotinine-measured PSE data showed no significant differences on the sleep variables. Perhaps in some of those homes where there was a smoker in the household, precautions to avoid exposing the child to the smoke were effective. However, more likely, the PSE is unrelated to sleep problems in this population, which displays it as a very common malady (nearly a third of children screened positive for sleep-disordered breathing), perhaps due more to obesity than allergen or toxin exposure.
One study, which measured height and weight and used a maternal questionnaire to determine smoke exposure, did not find an association between PSE and obesity in very young children. 8 However, passive smoke exposure was not the focus of the study; its effects were only examined in terms of the strength of its influence on the relationship between asthma and obesity. The current study in an older cohort of overweight and obese children focused on PSE as a risk factor for obesity and related disorders.
In the current study, cotinine-verified PSE was linked to poorer cognitive scores across the board (4–6 Standard Score points, or one-third of the population standard deviation on each of four scales), and participants with parent-reported smoke exposure in this study had lower scores on one measure of cognition. Other studies that analyzed serum or urine cotinine levels to determine PSE found similar associations between PSE and other standardized measures of cognition in children and adolescents, such as the Wide Range Achievement Test and the Wechsler Intelligence Scale for Children-III.12,13 This is also consistent with other studies using parent report.14–16 However, these studies did not adjust for the child's current adiposity. Our results confirm that PSE is linked with poorer cognitive performance in children, independent of adiposity.
As mentioned above, the cotinine-verified PSE measure did not corroborate the link with sleep problems in this study. Previous researchers found associations between cotinine-assessed PSE and sleep-disordered breathing in asthmatic children (56% black, 61% male, aged 6–12). 14 It appears that, because the children in the previously mentioned study had asthma, they were already predisposed to atopic respiratory disturbances that were compounded by PSE. The children in our study, being overweight and obese but otherwise healthy, may have sleep-disordered breathing more due to overweight than exposure to allergies.
Parent-reported PSE has been linked with lower adiponectin, higher leptin, adverse lipid profile, and a low-grade inflammatory response in German school children. 36 Additionally, in a meta-analysis relevant to the current study, PSE has been linked with increased risk of type 2 diabetes in adults, though mechanisms to explain this remain unclear. 37 Mechanisms linking PSE with adverse effects on cognition include hypoxia or increased carbon monoxide exposure from PSE. 38 PSE may worsen respiratory conditions that affect sleep quality, which could in turn hamper cognition. 14 Additionally, prenatal exposure to nicotine is linked with overweight and obesity as well as affecting the dopaminergic, adrenergic, and serotonergic centers of the brain, producing long-term neurocognitive deficits.10,12 It has been suggested that neurotransmitter imbalances and behavioral differences in smoking mothers (e.g., breastfeeding) may affect a child's weight status later in life.9,10 However, we did not have prenatal exposure measures in this study.
The current study has several limitations. The study is cross-sectional in nature, and we did not control for multiple testing. Furthermore, all children participants were either overweight or obese based on established BMI measurements. However, results are consistent with studies including normal weight children, thus findings of this study may be generalizable to normal weight children.9–11,39
The current study also has several strengths. It uniquely combines the use of biological measures of cotinine, adiposity, and related health risks with a standardized test of cognitive performance to examine possible relationships with PSE and found associations with overall and central adiposity as well as cognitive performance to the detriment of overweight and obese children. We compared findings between PSE based on the children's cotinine level and the parent's/caregiver's self-report of smoking status. Another unique aspect of this study was the comparison of adiposity, cognitive performance, and sleep disturbance in a healthy community sample of predominantly black overweight and obese American children that are afflicted with health disparities in these factors.
In this study, childhood PSE was associated with increased adiposity and decreased cognitive performance, independent of its association with adiposity, which has also been shown to confer a cognitive disadvantage.40,41 Thus, the study confirms that PSE endangers overall health and cognitive functioning in exposed children. These associations should spur intervention research, as both obesity and cognitive development have far-reaching effects on child outcomes. Tailored behavioral interventions that target multiple health and cognitive risk factors, including supports for nutrition, physical activity, neurocognitive development, and tobacco cessation and prevention in families with children, may have the largest impact to prevent adverse health and cognitive outcomes in children related to tobacco exposure.
Footnotes
Acknowledgments
This work was supported by grants R01 DK 60692, R01 DK 70922, and R01 HL087923 from the NIH and by the East Georgia Cancer Coalition. The content is solely the responsibility of the authors and does not necessarily represent the views of the NIH or the Georgia Cancer Coalition.
Author Disclosure Statement
No competing financial interests exist.
Ethical Statement Concerning the Conduct of Human Subjects Research
The procedures followed in the current study were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2008.