
Abstract
Abstract
Background:
While authoritative parenting, which includes high levels of warmth and behavioral control, has been associated with lower risk of obesity, little is known about how general parenting impacts child weight loss during treatment. Our goal was to examine the relationship between several general parenting dimensions and ‘decreasing /stable’ child BMI during a 16-week family-based behavioral weight control program.
Methods:
Forty-four overweight parent-child dyads (child age 8 to 12 years) enrolled in the program. Families were videotaped at baseline eating dinner in their home. Using the General Parenting Observational Scale (GPOS), meals were coded for several general parenting dimensions. Primary outcome was percent of children whose BMI ‘decreased or stayed the same.’ Multivariable logistic regression was used to determine the relationship between general parenting and decreasing/stable child BMI.
Results:
Forty families (91%) completed the program. Children had a mean BMI change of −0.40 (SD 1.57), which corresponds to a −0.15 (SD 0.20) change in BMI z-score (BMI-Z); 75% of children had decreasing/stable BMI. In the unadjusted models, lower parent BMI, higher parent education, and higher levels of parental warmth were significantly associated with decreasing/stable child BMI. In the multivariable model, only higher level of warmth was associated with increased odds of decreasing/stable child BMI (OR = 1.28; 95% CI, 1.01, 1.62).
Conclusions:
Baseline parental warmth may influence a child's ability to lower/maintain BMI during a standard family-based behavioral weight control program. Efforts to increase parent displays of warmth and emotional support towards their overweight child may help to increase the likelihood of treatment success.
Introduction
Currently, 33.2% of children age 6 to 19 years are overweight or obese (BMI ≥85th percentile). 1 Obesity in childhood is highly correlated with adult obesity, 2 and leads to higher risk of obesity-related comorbidities such as cardiovascular disease, 3 diabetes mellitus, 4 and cancer. 5 The current gold standard treatment for childhood obesity is family-based behavioral therapy (FBT), 6 which includes nutrition and physical activity education for parents and children, along with behavior therapy skills such as monitoring, goal setting, problem solving, stimulus control, and modeling.7–9 Despite its overall success, not all children respond to FBT. Studies demonstrate large variability in short-term outcomes,10–12 with only a third of children being able to maintain their weight status and another third increasing 20% or more from their baseline percent overweight at 10-year follow-up. 13
Since parents are responsible for structuring the home eating and physical activity environment, parent involvement in FBT is crucial.14,15 Studies comparing parent-focused interventions to child-focused interventions (for children age 6 to 11 years) show greater reduction in child percent overweight when parents are targeted as the agent of change (14.6% vs. 8.4%).16,17 Furthermore, parent-only programs that require parents to master weight control strategies and deliver it to their children (ranging in age from 8 to 14 years), without their child attending the treatment program, are equally effective as programs that involve both parent and child.18,19
Despite the importance of parents, little is known about how parents are contributing to their child's ability to decrease weight status during weight loss treatment. At a broader level, studies have shown that social risk factors like parent education and employment status are associated with a child's ability to lose weight; families with higher social risk are less likely to have children who lose weight. 20 On a behavioral level, parents who successfully lose weight are more likely to have children (age 8 to 12 years) who can decrease their BMI or BMI z-score (BMI-Z).10,21 These results suggest that parents may be modeling healthy behaviors or successfully making behavior changes to their own and their child's daily eating and activity habits. This idea was supported in another study that found that parent modeling of healthy eating and activity behaviors significantly predicted change in child percent overweight. 12 Furthermore, greater parent self-monitoring of their own behaviors significantly predicted adolescent weight loss. 22
Parents may also influence child outcomes via their general parenting style. General parenting style, or general parenting, can influence the emotional environment in the home and provide a context for the parent-child interaction that is potentially collaborative and supportive, or antagonistic and harmful. 23 The authoritative parenting style, characterized by high levels of warmth and support as well as maintenance of clear behavioral boundaries and expectations (behavioral control), has been associated with lower BMI and normal weight status,24–26 greater consumption of fruits and vegetables,27–30 and more frequent physical activity behavior27,28,31 in children. This emotionally and behaviorally supportive parenting style has also been associated with increased frequency of family meals, 32 a factor that has been linked with lower weight status for some, particularly whites and younger female teens in middle school.33,34 On the other hand, more negative parenting styles characterized by psychological control—a coercive and emotionally laden parenting style associated with authoritarian parenting that uses guilt induction, love withdrawal, possessiveness, and shame to manage a child's behaviors 35 —have been associated with higher child BMI-Z. 36 Despite these associations, few studies have examined how general parenting affects a child's ability to decrease weight status during a weight control intervention.
Given recent evidence that specific parent behaviors may influence child weight loss efforts, our goal was to examine whether the broader parenting dimensions of parental warmth and behavioral control were also associated with child success in decreasing weight status during a weight control intervention. Using an observational tool, the General Parenting Observational Scale (GPOS), 37 we examined whether these baseline parenting dimensions were associated with changes in child BMI during a 16-week family-based weight control program. Our primary hypothesis was that warm parenting and firm behavioral control would be associated with decreasing child BMI, while negative parenting (e.g., psychological control) would be associated with increasing child BMI.
Methods
Subjects
Children between the ages of 8 and 12 years and their parents were recruited to participate in a family-based weight control program via physician referrals, direct mailing, and advertisements in the community and schools in Providence, Rhode Island and San Diego, California. Eligible children had a BMI greater than the 85th percentile but were less than 100% overweight, and had parents who were willing to participate in the 16-week program. Families were excluded if the child was taking any medications that affected his or her weight or growth, was severely developmentally delayed, had a major psychiatric illness that prevented him or her from participating in the group sessions, or the family was moving out of the area within the next year. Children who were 100% overweight or higher were also excluded because of the significant medical comorbidities often associated with children at this weight status and the need for more intensive treatment. 38 Human subjects' approval was obtained from the institutional review board at the Miriam Hospital in Providence, Rhode Island and the University of California, San Diego in California.
Procedure
Families were initially screened via a brief phone interview. Those who were interested and met eligibility criteria were invited to the research center for an hour-long orientation session conducted by the principal investigator where additional information regarding the program was discussed. The informed consent process and child assent process was conducted at that time. Details regarding study enrollment are presented in Figure 1. In the end, 44 parent-child dyads entered the study; 21 families were from Rhode Island and 23 families were from California. There were no statistical differences between groups regarding demographic characteristics. P-values for parent demographics were sex, 0.86; age, 0.29; education, 0.45; marital status, 0.69; race/ethnicity, 0.94; and BMI, 0.53. P-values for child demographics were sex, 0.30; age, 0.12; and BMI-Z, 0.79.
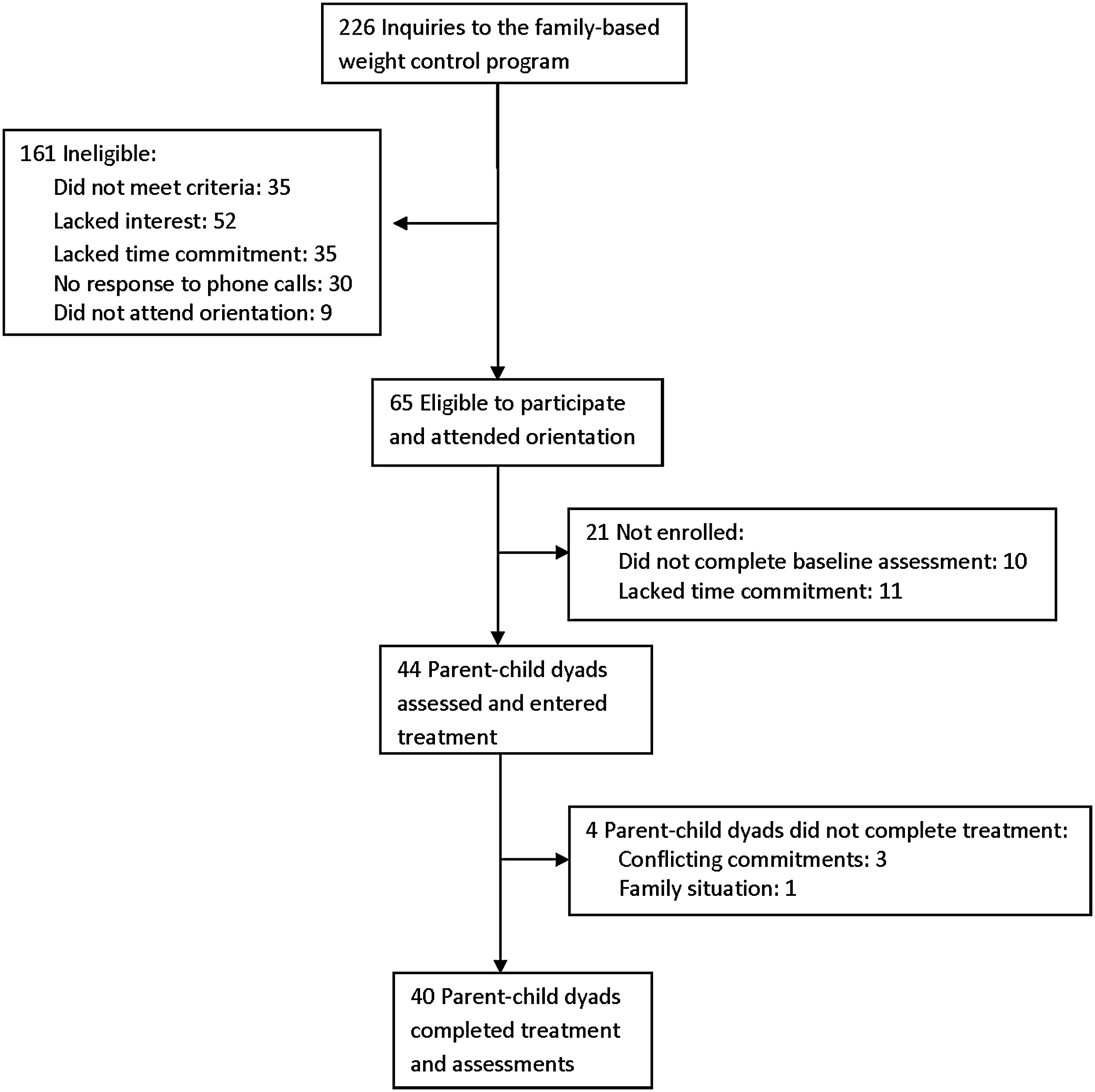
Flow diagram for study enrollment and retention.
The weight control intervention consisted of a 16-week family-based behavioral treatment program that included nutrition and physical activity recommendations, behavior therapy techniques, and parent management training.8,9 Children and parents met separately in one-hour group sessions for 16 weeks and learned about behavioral strategies that targeted improved eating and physical activity behaviors. To reduce caloric intake, parents and children received information regarding energy balance and the traffic light diet, a system that classifies foods into red, yellow, and green categories based on sugar and fat content as well as energy density.8,9 Families were encouraged to increase their intake of “green” foods and decrease their intake of “red” foods. Parents and children were also encouraged to engage in at least 60 minutes of physical activity per day and decrease sedentary behaviors. Families practiced how to set goals, self-monitor their eating and activity behaviors, plan ahead for difficult situations, and problem solve. Parents learned additional skills, such as how to limit portion sizes, change feeding behaviors, and modify the home environment to promote healthy behaviors. Parents were also encouraged to use praise, positive reinforcement, and a reward system to reinforce behaviors.
Pre- and postintervention assessments were completed by both children and parents. They included measured height and weight as well as surveys. Additionally, families were videotaped eating a family meal in their home before and after the intervention. In this analysis, however, only baseline video data was used. Research assistants (RAs) scheduled the taping to occur during the family's regular dinner hours (times ranged from 3:30 pm to 7:30 pm). Only index children and immediate family members were included in these meals. The RA set up a video camera in their dining area (kitchen, dining room, or living room) and turned the camera on when the family was ready to eat. She then left the house and returned in 30 minutes. Prior studies have indicated that parent-child behaviors during a meal are similar across three different tapings.39–41 As such, only one taping was performed for each family.
Parents were asked to rate the meal on two aspects: (1) how similar the meal was to their typical meal and (2) how similar the parent-child interaction was to their typical interactions. Scores were rated on a scale of 1 (not very typical) to 4 (very typical). Parents who scored the meal or the interaction as a 1 or 2 were told that an additional meal would have to be taped to ensure the validity of the data being collected. Only two families required an additional taping. Meals averaged 18.1 minutes (SD 3.2 minutes) in length (median = 20 minutes, interquartile range = 4 minutes). Therefore, up to the first 20 minutes of each videotaped family meal were coded for parenting behaviors and used for analysis.
Measures
Outcome
Child height and weight were obtained in the lab by trained RAs to determine BMI, BMI percentile, and BMI-Z. A Tanita digital scale (model WB-110A, Tanita, Arlington Heights, IL) was used to weigh children. Weight was measured twice in kilograms to the nearest 0.1 kg, and the average of the values used for analysis. Height was measured using a portable Tanita stadiometer. Height was recorded to the nearest 0.1 cm for both trials, and the average of the values was used for analysis. BMI (kg/m2) was calculated and translated to BMI percentiles for age and sex using the CDC growth charts, 42 and to standardized BMI-Z. 43 Given that the goal of treatment as defined by the Expert Committee Recommendations on the prevention, assessment, and treatment of childhood obesity is to maintain weight or lose one pound per month, 44 those who decreased their BMI or had no change in BMI were categorized as “decreasing/stable BMI,” while those who increased their BMI were categorized as “increasing BMI.”
Predictors
Parenting dimensions were obtained from the General Parenting Observational Scale (GPOS). 37 This scale was based on the Home Observation Coding System 45 and used a five-point global rating scale to determine the prevalence of 10 general parenting dimensions observed during the videotaped family meal. The 10 dimensions in the scale were based on work by Baumrind, 46 Maccoby and Martin, 47 Barber, 35 and Slater and Power 48 and were categorized into the emotional (warmth/affection, support/sensitivity, negative affect, detachment) and behavioral (firm discipline/structure, demands for maturity, psychological control, physical control, permissiveness, and neglect) domains of parenting. Definitions for each dimension are included in Table 1. Videotapes were divided into two-minute segments and scored from 1 (not present at all) to 5 (present a great deal) on each of the 10 dimensions. Scores were summed for each dimension with a possible range of 10 to 50. Meals less than 20 minutes long were coded and summary scores standardized to fit a 20-minute coding period. Two coders reviewed all tapes. They were initially trained to at least 90% reliability and met with the trainer weekly thereafter to prevent observer drift. Intraclass correlations for each dimension were warmth/affection = 0.87, support/sensitivity = 0.89, negative affect = 0.91, detachment = 0.81, firm discipline/structure = 0.87, demands for maturity = 0.91, psychological control = 0.95, physical control = 0.96, permissiveness = 0.85, and neglect = 0.74. 37 Coders reached consensus on any discrepant scores and these scores were used for analysis.
Dimensions were based on classic parenting concepts introduced by Baumrind, Maccoby and Martin, Barber, and Slater and Power.
Videotapes are divided into two-minute time periods, and each dimension is scored on a scale from 1 (not at all present) to 5 (present a great deal). Composite scores are calculated for each dimension based on a 20-minute videotape of a family meal.
GPOS, Global Parenting Observational Scale.
Several dimensions within the emotional parenting domain were highly correlated (r = 0.43 to 0.90) and exploratory factor analysis was conducted to determine the underlying factor structure of this domain. Similar analysis was not conducted with the behavioral dimensions of parenting, since these dimensions were conceptually different from each other and not as highly correlated. Factor analysis was conducted using Proc Factor in SAS version 9.3 (SAS Institute, Inc., Cary, NC), using the squared multiple correlations approach (PRIORS = SMC) and promax rotation. An item was said to load on a given factor if the factor loading was >0.30 for that component and <0.30 on the other component. However, only one factor emerged. Factor loadings were warmth/affection, 0.97; support/sensitivity, 0.92; negative affect, −0.34; detachment, −0.34. Eigenvalues were 20.45, 0.19, −0.02, and −0.18, respectively. Test of significance determined that one factor was sufficient (chi-square = 3.04, p = 0.22). Scores for negative affect and detachment were reverse coded, and scores from all four dimensions averaged to create a new “warmth” variable.
Covariates
Several sociodemographic variables were included in this study: parent and child age and gender, parent race/ethnicity, marital status, and educational level. In this sample the primary racial/ethnic groups were Caucasian, Hispanic, and other. Maternal education was dichotomized into those who had a “high school degree or less” or “some college or higher.” Marital status was dichotomized into “married or living with significant other” and “widowed, divorced, separated, or never married.”
Analysis
All statistics were completed using SAS software. Descriptive statistics were performed, and paired t-tests and Wilcoxon signed-rank sum test were used to determine significance regarding differences in weight status and parenting over time. Using baseline demographic variables and parenting dimensions, unadjusted logistic regression models were created to determine predictors of decreasing/stable child BMI. The parenting variable “warmth” was normally distributed and used as a continuous variable in all analyses. The behavioral parenting dimensions were skewed to the right. Log and square root transformation of these variables did not normalize the distribution. Therefore each variable was dichotomized into those who displayed none of the behavior (score = 10) and those who displayed some of the behavior (score >10). A multivariable logistic regression model was created using significant demographic and parenting variables to determine the odds of decreasing/stable child BMI during the intervention. Alpha level of 0.05 was used to determine significance.
Results
Children in the intervention had a mean BMI percentile of 98.2 (SD 1.3) and BMI-Z of 2.2 (SD 0.3) (Table 2). Two-thirds of the children were female with a mean age of 10.0 years (S.D. 1.3). Mothers were the primary participant in the intervention (95%), and 77% of parents were married or living with a significant other. Parents had a mean age of 41.4 years (SD 6.9) and were overweight (mean BMI = 30.1, SD 5.8).
Demographic Characteristics of Participating Children and Parents (n = 44 dyads)
There was a significant decrease in child BMI percentile (p < 0.01) and BMI-Z (p < 0.001) at the end of the intervention (Table 3). Children during the intervention had an average change of −0.40 (SD 1.57) BMI points which corresponded to a decrease of 1.03 (SD 1.99) BMI percentile points and a −0.15 (SD 0.20) change in BMI-Z. Overall, 75% of children had a decrease or no change in their BMI. One-third of these children lost weight, while two-thirds maintained their weight or gained a modest amount of weight (2.6 pounds or less) but also gained in height, thus maintaining a stable BMI. General parenting did not change significantly during the course of the intervention (Table 3).
Examining changes in child weight status and general parenting dimensions from baseline to posttreatment a
Posttreatment assessments occurred at the end of the 16-week family-based behavioral weight control intervention.
IQR, interquartile range.
In the unadjusted logistic models (Table 4), baseline parent BMI (OR = 0.85; 95% CI, 0.74, 0.99) and education (OR = 10.33; 95% CI, 1.86, 57.42) were significantly associated with decreasing/stable child BMI. Parental warmth was the only general parenting dimension that was significantly associated with decreasing/stable child BMI (OR = 1.31; 95% CI, 1.06, 1.60). All significant variables were entered into a multivariable logistic regression model. In the adjusted model, parental warmth was the only variable associated with change in child BMI such that higher levels of warmth were associated with an increased odds of decreasing/stable child BMI (OR = 1.28; 95% CI, 1.01, 1.62). The final model accounted for 18% of the variance, and parental warmth contributed to 5% of the variance, i.e., 18% of the variation in the decrease/stability in BMI was explained by this multivariable model.
Factors associated with decreasing/stable child BMI during the course of a family-based behavioral weight control program
Model 1 represents unadjusted odds ratios and 95% CI.
Model 2 represents the multivariable logistic regression model including all significant demographic and parenting variables from the unadjusted models. R2 for model 2 = 0.18. Warmth contributed to 5% of the variance.
Warmth was normally distributed and used as a continuous variable. Higher scores indicated higher levels of warmth. The remaining parenting variables were dichotomized into those that did not display any of the noted behavior (0) and those that did (1).
Discussion
Over the past several years there has been growing interest in the role of parents in the development and treatment of obesity. 49 The purpose of this analysis was to examine the association between general parenting and decreasing/stable child BMI during a family-based weight control intervention. We found that general parenting defined by greater levels of warmth and support was significantly associated with decreasing or maintaining child BMI during the course of a 16-week intervention. Other studies have shown that specific parent behaviors like the use of praise during FBT are associated with a decrease in child percent overweight.12,50 When examining the broader dimension of parenting style, only one other study by Stein and colleagues found that an authoritative parenting style among fathers was associated with greater decreases in child percent overweight during the course of their weight loss intervention. 51 Of note, they found that fathers increased their use of acceptance-based parenting during the intervention and this change in parenting was associated with decreases in child percent overweight. While we did not see a change in parenting during the course of the intervention, we did find that baseline levels of parenting were associated with decreasing or stable child BMI. The results of these studies highlight the potential importance of general parenting in weight loss efforts.
The fact that warmth and support was associated with decreasing or stable child BMI suggests that parents who were emotionally supportive of their child's weight control efforts created an environment that encouraged healthy behaviors. Parents who have an authoritative parenting style (that is characterized by high levels of warmth and support as well as behavioral control) have also been found to have children who engage in their own self-care behaviors around diabetes management 52 and have greater psychosocial functioning. 53 Fewer criticisms may (1) help children feel they can successfully make the required behavioral changes for weight loss and (2) promote continued adoption of these new behaviors. While we did not specifically quantify the use of praise statements, the positive reinforcement created by warm parenting may be contributing to children feeling supported in their efforts and lead to a greater likelihood of success in weight loss programs.
While the study results are strengthened by the use of observational data that corroborates the results from other studies that used self-report data, there are some limitations to consider. First, the sample was relatively small and there was little variability in the behavioral dimensions of parenting. This may have limited our ability to detect significant relationships between the harsher behavioral dimensions of parenting, like psychological control or physical control, and changes in child BMI. We also did not assess father's and mother's general parenting separately and cannot comment on the impact of each parent's parenting style on this relationship. Future analyses should continue to tease apart the unique impact each parent has on the child and his or her development. In addition, we did not code for specific feeding behaviors that have previously been shown to relate to weight status.54,55 Finally, our sample was primarily white and we had limited ability to determine if parenting behaviors differed among the racial/ethnic groups or had varying impact on child outcomes. Larger studies with more diverse populations are needed to examine cultural variability in parenting and its impact on child weight-related behaviors and outcomes.
Conclusions
The results of this study begin to highlight the potential impact of parenting style in weight loss interventions. Previous reports have demonstrated that specific parenting practices, like modeling eating healthy foods or monitoring child activities,12,22 are important in childhood obesity interventions. We found that general parenting dimensions are also associated with changes in child weight status during a weight control intervention. Future interventions may need to place additional emphasis on promoting general parenting styles that display warmth and support for their child's efforts in order to improve pediatric weight loss outcomes.
Footnotes
Acknowledgments
We are grateful to the staff at the Weight Control and Diabetes Research Center (Rhode Island) and the Center for Healthy Eating and Activity Research (California) who participated in data collection and the families who participated in the study. This research was supported by grant number K23HD057299 from the Eunice Kennedy Shriver National Institute of Child Health and Human Development awarded to KR.
Clinical Trials Registry Name and Number
The role of parenting skills, style, and family functioning in pediatric weight loss. NCT01004341.
Author Disclosure Statement
The authors have no competing financial interests. The content is solely the responsibility of the authors and does not necessarily represent the official views of the Eunice Kennedy Shriver National Institute of Child Health and Human Development or the NIH.