
Abstract
Abstract
Background:
Research has provided evidence that obesity is associated with peer victimization and low levels of self-concept. No study has examined the relationship between BMI z-score, self-concept in multiple domains, and peer victimization.
Methods:
The aim of the research was to investigate the interplay between BMI z-score, self-concept in multiple domains (physical, athletic, social), and peer victimization, testing direct, mediated, and moderated associations. Eighty hundred fifteen outpatient children and adolescents were consecutively recruited in 14 hospitals distributed over the Italian country. The sample consisted of 419 males and 396 females; mean age 10.91 ± 1.97 years (range 6–14 years) and mean BMI z-score 1.85 ± 0.74 (range −0.97 ± 3.27). Peer victimization and self-concept were assessed with a revised Olweus Bully/Victim Questionnaire and with the Self-Perception Profile for Children. A structural equation model approach was used to determine the associations among variables, testing two competing models.
Results:
In both models, path analysis revealed that BMI z-score was directly associated with peer victimization and self-concept in multiple domains. In the first model, peer victimization mediated the relationship between BMI-score and self-concept, whereas in the alternative model, self-concept mediated the relationship between BMI z-score and peer victimization. Interaction analyses revealed that social competence moderated the relationship between BMI z-score and peer victimization and that peer victimization moderated the relationship between BMI z-score and physical appearance.
Conclusions:
Higher levels of BMI z-score are a risk factor for peer victimization and poor self-concept. When high levels of BMI z-score are associated with a negative self-concept, the risk of victimization increases. Preventive and supportive interventions are needed to avoid negative consequences on quality of life in children and adolescents with obesity.
Introduction
In recent years, a growing body of research has provided evidence that being overweight or obese is one of the most common reasons that children and adolescents are victimized by peers.1–5 Weight-based victimization occurs at school more often than victimization due to race, religion, or disability2,6 contributing to negative emotional consequences,4,7 academic failure, 8 and peer rejection. 2 A meta-analysis 9 carried out on 30 published articles concluded that both overweight and obese youths, without distinction by gender, were more likely to be victims of bullying. Most studies concluded that negative peer relationships among obese individuals, and in particular among those who are severely obese, 10 are due to the negative stigma toward obese children. 11
Despite the evidence of the association between BMI and peer victimization, the psychological mechanisms that mediate and moderate this relationship need to be further investigated. Therefore, the focus of the present study is on investigating the complex interplay among BMI, peer victimization, and self-concept in childhood and adolescence. Overweight and obese children often suffer from a negative self-concept more than their normal-weight peers do12–14 as a consequence of the related social stigma 11 and the lack of adequate coping strategies. 4 However, not all studies have found a negative association between BMI and self-concept. 15 It is worthy of consideration that in the literature there are many declinations of self-concept (e.g., self-esteem vs. self-image vs. self-efficacy) and that self-concept can be considered either as a unidimensional (e.g., global self-esteem) or a multidimensional and multifaceted construct. 16 In this light, obesity was found to affect self-perception in physical and social domains but not in academic domains. 14 Moreover, gender seems to moderate this association because obese boys were found to have lower levels of perceived physical and athletic competence than their normal-weight peers,12,17 whereas obese girls showed lower levels of perceived social competence. 12
In addition, peer victimization is generally associated with lower self-concept 18 in a vicious circle where the variables are reciprocally influenced. Several studies found that a weak sense of self-worth makes a child more vulnerable to attacks from bullies within a peer group19,20 because victims of bullying are usually perceived as vulnerable, submissive, or different by peers in dominant roles. At the same time, it is unquestionable that repeated experiences of peer victimization have a subsequent detrimental effect on self-esteem. 21
The few studies that have examined the interplay between BMI, self-concept, and peer victimization did not reach conclusive findings. Global self-esteem 22 and physical self-esteem 23 were found to mediate the relationship between BMI and peer victimization. Conversely, peer victimization was found to mediate the relationship between BMI and self-esteem 24 in Taiwanese adolescents, and to mediate the relationship between body dissatisfatction and self-worth in a US sample. 25 A moderating role of self-concept was also found26,27 as peer victimization was higher in overweight subjects who experienced higher levels of negative perception of their body image.
The purpose of the present study was to investigate the interplay among BMI, multiple dimensions of self-concept (i.e., physical appearance, athletic, and social competence), and peer victimization in a sample of normal-weight, overweight, and obese pediatric outpatients. In the light of theoretical assumptions based on the literature,22–25 we compared two plausible and alternative models (A and B) of relationships among variables. Common to both models, BMI was expected to be positively associated with peer victimization and negatively associated with multiple dimensions of self-concept. In model A, we also hypothesized that the relationship between BMI and peer victimization was mediated and moderated by self-concept. In model B, we hypothesized that the relationship between BMI and multiple domains of self-concept was mediated and moderated by peer victimization. The two theoretical models are shown in Supplementary Figure S1 (Supplementary Data are available online at www.liebertpub.com/chi). Since we are aware that BMI, self-concept, and peer victimization might be influenced by factors such as age, gender, parents' education level, and ethnicity,2,3,6 we accounted for these confounding variables in our hypotheses.
Materials and Methods
Participants
Participants were recruited in 14 hospitals distributed across northern (4 sites), central (6 sites), and southern (4 sites) Italy. Participants were consecutively enrolled in numbers weighted to each pediatric service population. In each hospital, a first setting of recruitment was constituted by outpatient clinics for the treatment of childhood overweight and obesity; a second setting was constituted by hospital ambulatories attended by children for preventive healthcare or minor complaints (recovery after infectious acute illness, minor medical procedures, dental services, and dermatology services).
In the first setting, we recruited 714 overweight and obese individuals (BMI z-scores >1), aged from 6 to 14 years, not affected by other independent pathology associated with weight status, and regularly attending school (from first to eighth grade). In the second setting, we recruited 101 normal-weight individuals (BMI z-scores >−1 and <1), aged from 6 to 14 years, without active or chronic pathology at the time of the interview, and regularly attending school. Underweight children were not enrolled in the study because they represent a specific at-risk population, whose distinctive psychological and sociorelational mechanisms leading to victimization and negative self-concept fall outside the scope of this article. All participants were consecutively recruited between November 2011 and May 2012.
The final sample consisted of 815 individuals, 419 males and 396 females, mean age 10.91 years ±1.97, BMI z-score ranged from −0.97 to 3.27, mean 1.85 ± 0.74.
The study was approved by the Ethics Committee of the Department of Psychology of the Second University of Naples and by the Childhood Obesity Group Board of the Italian Society of Pediatric Endocrinology and Diabetology. Written informed consent was obtained from all participants and/or their parents or legal guardians in accordance with the revised version of the Helsinki Declaration regarding research involving human subjects.
Measures
Anthropometric measures
Body weight was determined to the nearest 0.1 kg on accurate and properly calibrated standard beam scales, with the children in minimal underclothes and no shoes. Height was measured to the nearest 0.5 cm on standardized, wall-mounted height boards according to standardized procedures. The BMI was calculated as weight divided by square of height (kg/m2). The BMI z-score was calculated using the CDC standards. 28
Sociodemographic measures
Information about ethnic group (Italians vs. other ethnic groups) and parents' educational level was also collected. Mothers and fathers reported their attained educational levels on a five-point scale, where 0 = illiterate and 4 = finished university education or higher. A combined value of mother's and father's levels was computed.
Peer victimization
We administered a modified version of the “revised Olweus Bully/Victim Questionnaire” 29 administering 10 items concerning different types of school victimization (verbal, physical, and relational). Two items aimed to specifically detect weight-based victimization 4 were inserted ad hoc: “How often have you ever been teased/have you been excluded from sports activities by your peers because of your weight?” For each item, participants were asked to respond “How often have you been bullied at school in the past couple of months?” using a five-point scale (“never involved,” “only once or twice,” “2 or 3 times a month,” “about once a week,” “several times a week”). A trained assistant administered the questionnaires in a separate room following an administration protocol shared among the participating centers. The assistant had a briefing with the participants to ensure that the key concepts included in the standard definition of bullying, such as the intention to harm the victim, the repetitive nature of bullying, and the imbalance in power between the victim and the perpetrator(s), were clearly understood. The questionnaire was self-administered but the assistant remained in the room to provide support if the participants requested such. The assistant only read the items aloud if the participants had limited reading skills (e.g., younger children). No protocol deviations were registered during the data collection. The scale showed good internal consistency (alpha = 0.75). The two weight-based victimization items showed moderate–good correlations with the other items of the scale (from 0.21 to 0.48).
Self-concept
The Self-Perception Profile for Children 30 is a domain-specific self-report questionnaire that assesses children's perceived self-competence in a number of domains. We investigated three domains: (1) social competence; (2) athletic competence; and (3) physical appearance. Each subscale consisted of six items. The response to each item was scored from 1 to 4, where participants indicated which statement was most like them and to what degree the statement was true or not true of them. Higher scores indicate more positive self-evaluations. Cronbach's alpha coefficients were, respectively, social acceptance (0.73), athletic competence (0.70), and physical appearance (0.79).
Data Analysis
For each scale, a mean value was calculated by summing the scores divided by the number of items (10 for the victimization scale and 6 for each subscale of self-concept).
Descriptive analyses were executed to investigate variable distributions. Pearson's correlation for continuous variables and biserial correlation for dichotomic variables coefficients were computed to investigate bivariate relationships among the variables used. To examine pairwise correlation relationships among variables, the structural equation model (SEM) approach was used to determine the directional associations among variables for each model. Three interaction terms associated with victimization were included in the model A: BMI z-score × physical appearance, BMI z-score × social competence, and BMI z-score × athletic competence. One interaction term associated with the three self-concept dimensions was included in the model B: BMI z-score × peer victimization. To interpret these interactions, the z scores (M, M + 1 SD, M − 1 SD) of BMI, self-concept domains, and peer victimization were computed on the basis of the means and standard deviations of these variables in the study sample, following the Aiken and West procedure. 31
Moreover, to test the moderating effect of participants' gender, a multiple-group SEM was executed as a function of gender. Specifically, to test this moderation, that is the equivalence of the structural parameters across groups (males vs. females), two nested models were considered: a configural invariance model (baseline model) that investigates the relationships between the variables simultaneously for males and females; and a more constrained model with the invariance of the structural paths across groups.
Finally, the models also included age, parental education, and ethnicity as potential covariates influencing all the variables, to minimize the possibility of detecting spurious relationships due to the omission of relevant variables (the effects of the covariates are not shown in the Figures for clarity of representations).
The maximum likelihood method was used to test the model's fit indices and path coefficients. Supplementary Data illustrates the indices for the evaluation of the models. Univariate analyses were performed using SPSS version 21 and SEM was computed using MPLUS 7.1 software.
Results
The means, standard deviations, and zero-order correlation coefficients among variables are listed in Table 1, separately for males and females. The analysis revealed many significant relationships. In particular, for both males and females, age was negatively correlated with BMI z-score and physical appearance; parents' education was positively correlated with physical appearance, social competence, and athletic competence; BMI z-score was negatively correlated with physical appearance, social competence, and athletic competence, and positively correlated with victimization; and physical appearance, social competence, and athletic competence were negatively correlated with victimization. Furthermore, for males only, parents' education was negatively correlated with BMI z-score and victimization, and for females only, age was negatively correlated with parents' education, athletic competence, and victimization.
Correlations for Measures of Age, Parents' Education, Ethnicity, BMI z-score, Physical Appearance, Social Competence, Athletic Competence, and Victimization by Gender
Means, standard deviations, and correlations for males are below the diagonal; means, standard deviations, and correlations for females are above the diagonal.
p < 0.05.
p < 0.01.
p < 0.001.
Then, we compared the two alternative models. First, we tested model A. To test our hypothesis, we initially examined the relationships between the variables simultaneously for males and females. The model was saturated and showed a perfect fit for the basic configural model, χ2 (0) = 0, p = 0.001, The Root Mean Square Error of Approximation (RMSEA) = 0.0, 90% confidence interval (CI) [0.0–0.0], Tucker Lewis Index (TLI) = 1, Comparative Fit Index (CFI) = 1, Akaike Information Criterion (AIC) 23594.96. Next, we set the invariance of the structural paths across males and females, and the fit for this model was χ2 (25) = 34.67, p > 0.05, RMSEA = 0.03, 90% CI [0.0–0.05], TLI = 0.97, CFI = 0.99, AIC 23579.63. The Δχ2 statistic showed that the constrained model was not significantly poorer than the baseline model, Δχ2 (25) = 34.67, p > 0.05. Therefore, we chose this last model because it showed good fit and indicated that the relationships between the variables were the same in males and females. Overall, the model explained a reasonable percentage of the variance for physical appearance (15% for males and 18% for females), social competence (8% for males and females), athletic competence (7% for males and 8% for females), and victimization (20% for males and 21% for females).
As shown in Figure 1, the following results were found in both gender groups: (1) BMI z-score was negatively related to physical appearance, social competence, and athletic competence, and positively related to victimization; (2) physical appearance and social competence were negatively related to victimization. Furthermore, the analysis of the indirect effects showed that BMI z-score was related to victimization via physical appearance (β = 0.04, p < 0.01 for males and females) and social competence (β = 0.06, p < 0.001 for males and females).
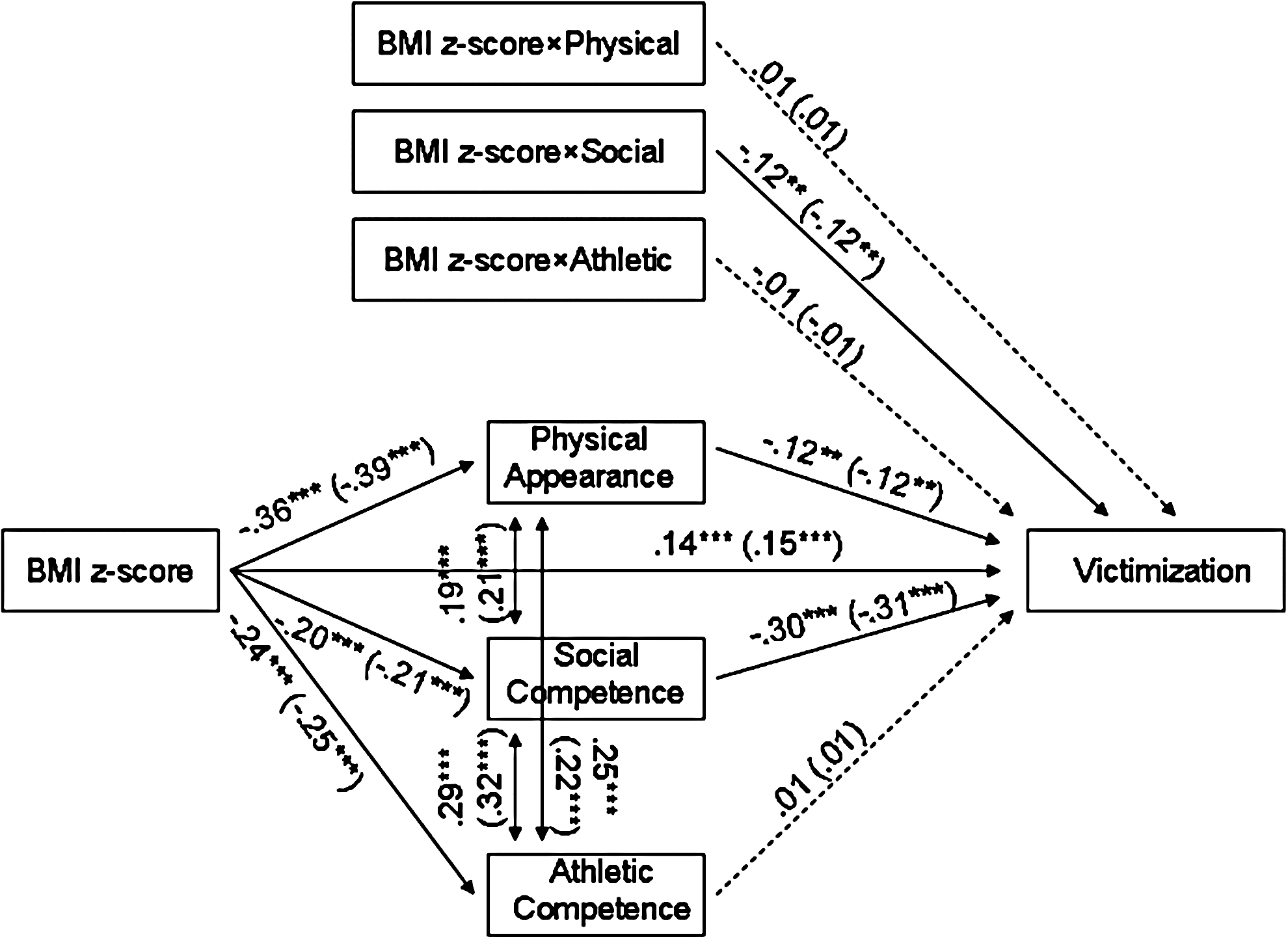
Model A: relationships among BMI z-score, physical appearance, social competence, athletic competence, and victimization. BMI z-score × physical: interaction term BMI z-score × physical appearance. BMI z-score × social: interaction term BMI z-score × social competence. BMI z-score × athletic: interaction term BMI z-score × athletic competence. Standardized path coefficients. The interaction terms covary with all other variables. Parameters for males are shown without brackets, parameters for females are shown in brackets. Dashed lines indicate nonsignificant paths. *p < 0.05, **p < 0.01, ***p < 0.001. The paths from age, parents' education, and ethnicity to all other variables were omitted for sake of simplicity and are reported in Supplementary Table S1.
The interaction term BMI z-score × social competence was negatively associated with victimization (Fig. 2). The association between social competence and victimization was negative at higher (t = −9.17, p < 0.0001, 95% CI [−3.73 to −2.41]) and medium (t = −8.72, p < 0.0001, 95% CI [−2.72 to −1.71]) BMI z-score values, and remained negative, although attenuated, at lower BMI z-score values (t = −3.34, p < 0.001, 95% CI [−2.16 to −0.56]). For clarity in interpreting the results, we point out that the BMI z-scores were restandardized in these interaction analyses, so higher or lower values of BMI z-score should not be interpreted in absolute terms, but relative to the distribution of the scores in the whole sample.
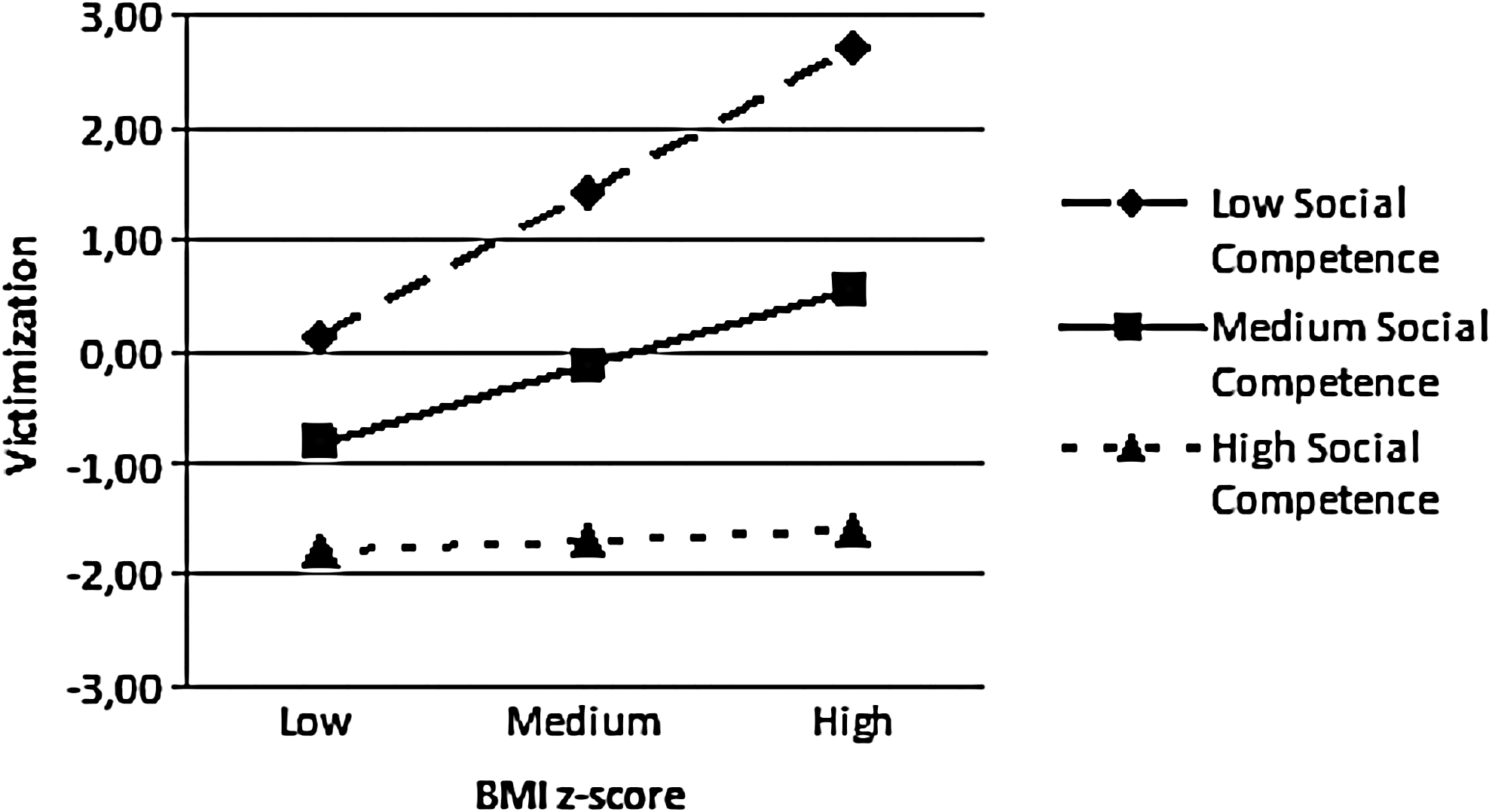
Interaction effects between social competence and BMI z-score on victimization. Plotted the interaction effects between social competence and BMI z-score on victimization. The labels “low,” “medium,” and “high” for BMI z-score and social competence correspond to −1 SD; 0; +1 SD relatively to the distribution of these variables in the total sample. Low levels of BMI z-score are associated with victimization independent of the levels of social competence. Conversely, medium and high levels of BMI z-score associated to medium and low levels of social competence expose individuals to higher victimization.
The same procedure was followed for the model B. We initially examined the relationships between the variables simultaneously for males and females. The model was saturated and showed a perfect fit for the basic configural model, χ2 (0) = 0, p = 0.001, RMSEA = 0.0, 90% CI [0.0–0.0], TLI = 1, CFI = 1, AIC 24133.36. Next, we set the invariance of the structural paths across males and females, and the fit for this model was χ2 (25) = 32.09, p > 0.05, RMSEA = 0.03, 90% CI [0.0–0.05], TLI = 0.98, CFI = 0.99, AIC 24115.45. The Δχ2statistic showed that the constrained model was not significantly poorer than the baseline model, Δχ2 (25) = 32.09, p > 0.05. Therefore, we chose this last model because it showed good fit and indicated that the relationships between the variables were the same in males and females. Overall, the model explained a reasonable percentage of the variance for victimization (6% for males and 7% for females), physical appearance (19% for males and 22% for females), social competence (21% for males and 18% for females), and athletic competence (9% for males and 10% for females).
As shown in Figure 3, the following results were found in both gender groups: (1) BMI z-score was positively related to victimization and negatively related to physical appearance, social competence, and athletic competence; (2) victimization was negatively related to physical appearance, social competence, and athletic competence. Furthermore, the analysis of the indirect effects showed that BMI z-score was related to physical appearance (β = −0.04, p < 0.001 for males and females), social competence (β = −0.07, p < 0.001 for males and females), and athletic competence (β = −0.03, p < 0.01 for males and females), via victimization.

Model B: Relationships among BMI z-score, victimization, physical appearance, social competence, and athletic competence. Standardized path coefficients. The interaction terms covary with all other variables. Parameters for males are shown without brackets, parameters for females are shown in brackets. Dashed lines indicate nonsignificant paths. *p < 0.05, **p < 0.01, ***p < 0.001. The paths from age, parents' education, and ethnicity to all other variables were omitted for sake of simplicity and are reported in Supplementary Table S1.
The interaction term BMI z-score × victimization was negatively associated with physical appearance (Fig. 4). The association between victimization and physical appearance was significant and negative at lower (t = −4.01, p < 0.0001, 95% CI [−0.06 to −0.02]) and medium (t = −3.75, p < 0.0001, 95% CI [−0.03 to −0.01]) BMI z-score values, and not significant at higher BMI z-score values (t = −0.52, p > 0.05, 95% CI [−0.01 to 0.0]).

Interaction effects between physical appearance and BMI z-score on victimization. Plotted the interaction effects between physical appearance and BMI z-score on victimization. The labels “low,” “medium,” and “high” for BMI z-score and physical appearance correspond to −1 SD; 0; +1 SD relatively to the distribution of these variables in the total sample. High levels of BMI z-score are associated with negative physical appearance independent of the levels of victimization. Conversely, low and medium levels of BMI z-score associated to high and medium levels of victimization expose individuals to higher negative physical appearance.
Supplementary Table S1 illustrates the effects of the three covariates, age, parents' education, and ethnicity on all the examined variables of the two posited models.
Discussion
This study tested two conceptual models depicting the interplay among BMI z-score, self-concept in three domains (physical appearance, athletic competence, and social competence), and peer victimization. The sample involved children and adolescents recruited in 14 Italian hospitals, mostly overweight and obese. Bivariate correlations showed the expected significant relationships among the study variables since, according to previous studies, BMI z-score was negatively associated with self-concept in multiple domains12,17 and positively associated with peer victimization.1–5
Two plausible competing models of interrelationships of the study variables were tested. In model A, self-concept in multiple domains was hypothesized to mediate and moderate the relationship between BMI z-score and peer victimization. In model B, peer victimization was hypothesized to mediate and moderate the relationship between BMI z-score and self-concept. Since both Model A and B showed excellent indexes of fit, neither model could be excluded. Specifically, both models showed a direct association between (1) BMI z-score and peer victimization; (2) BMI z-score and self-concept in multiple domains. Model A also showed (3) a partial mediation of social competence and physical appearance on the relationship between BMI z-score and peer victimization; (4) an interaction between BMI z-score and social competence on peer victimization. Model B also showed (3) a partial mediation of peer victimization on the relationship BMI z-score and all the self-concept domains; (4) an interaction between BMI z-score and peer victimization on physical appearance. No differences by gender were found regarding these paths of relationships in both models.
Even though our results are partially in line with previous studies, they provide a novel contribution to the research investigating simultaneously the relationship between BMI z-scores, self-concept, and peer-victimization. The findings related to the first two hypotheses of Model A and B are consistent with a wide breadth of literature9,13 showing that higher levels of BMI z-scores are associated with higher levels of peer victimization and lower levels of self-concept. These associations were found both in males and in females and they remained stable even after controlling the results for age, parental education level, and ethnicity. An innovative result was that the close association between high levels of BMI z-scores and a negative self-concept was detectable not only in predictable domains, such as physical appearance and athletic competence, but also in the social domain. Examining the reason that obese children perceive themselves as less competent in the social domain was not an aim of the present study; nevertheless, it is conceivable that the low levels of self-regulatory abilities affecting obese individuals 32 might extend, at the same time, their detrimental effects to social relationships.
By comparing the indirect effects (third hypothesis) indicated by both models, a complex interplay was found between self-concept and peer victimization in relation to BMI z-score. Model A suggests that the negative self-perception in several domains elicited by higher levels of BMI z-score may be associated to higher levels of victimization, because low self-concept may render children and adolescents more vulnerable to the attacks of peer bullies, 24 who explicitly burden those individuals whom they perceive as weaker and unable to defend themselves. At the same time, model B suggests that victimization, elicited by higher levels of BMI z-score, may be associated to a negative self-concept 25 since the experience of victimization might trigger a self-debasing process.
Considering the interaction effects (fourth hypothesis), model A evidenced that high levels of perceived social self operate as a protective factor against peer victimization even in the presence of high levels of BMI z-score, whereas low levels of perceived social self operate as an incremental risk factor when associated with high levels of BMI z-score. This finding suggests that the relationship between BMI z-score and peer victimization should not be simply assumed. Indeed, personality variables (such as the self-perception of social abilities) may assume an important role in amplifying or minimizing this relationship. Model B evidenced that high levels of BMI z-score are associated with low levels of perceived physical appearance independent of the levels of peer victimization, whereas low levels of BMI z-score in association with low levels of peer victimization amplify a positive concept of physical appearance in children.
Limitations and Future Directions
Results from this cross-sectional study should be interpreted as associations rather than causal influences. Since path analysis evidenced the goodness of fit of both models, longitudinal research is needed to establish the real causal pathways. More specifically, cross-lagged panel models should test the longitudinal stability of the variables and their reciprocal influence over time, not only to establish whether self-concept affects peer victimization or vice versa but also to detect whether negative self-concept or peer victimization might affect BMI z-score. For instance, it is also plausible that repeated experiences of victimization or that a negative self-concept could lead to emotional overeating behavior or to social withdrawal with a detrimental effect on the BMI z-score. It should be also taken into account that the obese participants in the present study were weight-loss treatment-seeking outpatients who represent a specific category within the obese population. Indeed, they might perceive their obesity more seriously than untreated obese individuals and suffer more from psychological or physical issues than obese individuals who are not in treatment.
Conclusions
The novel contribution of the present study relies on the simultaneous investigation of the complex relationships between BMI z-score, self-concept in multiple domains, and peer victimization in a sample of children and adolescents mainly overweight and obese. High levels of BMI z-score resulted a direct risk factor for peer victimization and negative self-concept in multiple domains such as physical appearance, athletic competence, and social competence. The two tested models provide a basis for understanding the psychological mechanisms linking BMI z-scores, peer victimization, and self-concept. Even though the study was not able to cover the gap about which is the actual direction of the influence among variables, it suggests that peer victimization and poor self-concept should be considered serious comorbidities of overweight and obesity. Results suggest the urgent need to implement policies aimed to support overweight and obese children and adolescents paying particular attention to the needs of weight-loss treatment-seeking subjects. Community, family, and school policies should be aimed at fighting prejudices and stereotypes, 33 which can lead to peer victimization, to break the vicious circle between physical, psychological, and sociorelational status.
Providers involved in the care of pediatric obesity should incorporate their area of expertise into developing a comprehensive evaluation of patients' characteristics, strengthening their self-concept to prevent peer victimization. At the same time, they should alert parents and teachers to monitor the peer network of children, to avoid a vicious circle between peer victimization and self-concept, which could negatively affect the adherence to weight-loss programs.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.