
Abstract
Abstract
Background:
The Feeding Exercise Trial in Adolescents (FETA) aimed to evaluate whether a community-based, parents-involving, combined physical activity and nutritional education program was effective in improving adiposity profiles in overweight and obese adolescents.
Methods:
A total of 181 overweight and obese adolescents aged 13–15 years old were randomized in the three study groups (“Diet & Activity,” “Activity,” and Control). The Activity intervention included a 45-minute, 3-day per week supervised training program, while the Diet & Activity intervention included a supplementary 15 minutes of group-based sessions attended by the parents. The intervention lasted 3 months and the participants were followed for another 3 months after the intervention. The participants were assessed for anthropometric measures and activity and fulfilled the modified version of the questionnaire “Family Eating and Activity Habits Questionnaire” (FEAHQ).
Results:
Both “Activity” only and “Diet & Activity” groups reduced significantly (p < 0.001) their mean body mass index (BMI) (−1.1, 95% CI −1.3, −0.8, and −1.4, 95% CI −1.7, −1.2, respectively), waist circumference, systolic and diastolic blood pressure, pulses per minute, and 50 m sprint run test at 3 months, while greater reductions in BMI were observed at 6 months (−2.3, 95% CI −2.6, −2.0, and −3.1, 95% CI −3.3, −2.8). Significant changes in the total FEAHQ score were achieved only in the “Diet & Activity” group both at 3 months and at 6 months.
Conclusions:
FETA resulted in significant effects on improving adiposity profiles in overweight and obese adolescents, as well as family activity and feeding habits, maintained at 3 months follow-up.
Introduction
Childhood obesity has been recognized as “a new pandemic of the millennium.” 1 Due to the fact that it is directly associated with increased children morbidity, 2 as well as with adult obesity and morbidity, 3 its prevention and treatment have become a primary concern in developed countries. Although numerous interventions, mainly school based, have been previously tested, the development and implementation of effective prevention and treatment strategies remain a challenge.4,5
Review of published intervention programs have shown that over half of the school-based interventions were effective in reducing overweight, obesity, or adiposity measures for at least one subgroup of children. 4 In contrast, the strength of evidence for the effectiveness of combined diet and physical activity community interventions is moderate, since less than half have shown favorable changes.5,6 Different methodological approaches and cultural backgrounds may make comparisons among studies more difficult; however it has been argued that the diversity of effective interventions is desired since it increases the likelihood to find programs suitable for adaptation in different communities. 4 Furthermore, since the majority of previous studies have used only one intervention group,4,5 programs using more than one intervention groups are expected to provide a better insight in drawing more clear conclusions on the relative effectiveness of each intervention approach. Moreover, previous studies suggested that weight-related health interventions that required parent participation reduced more effectively body mass index (BMI) of child and adolescent participants, indicating the key role of parents in the prevention and treatment of childhood obesity.7–10
The Feeding Exercise Trial in Adolescents (FETA) was a randomized controlled intervention study designed to promote healthy weight in overweight and obese adolescents through a professional-delivered, community-based program with active parents' involvement, focused on supervised physical activity and structured nutritional education. The aim of FETA was to test the efficacy of two intervention groups, physical activity in isolation and combination of physical activity with provision of dietary information, in improving overweight and obesity in adolescents and also to compare each of them to a control group. Our primary hypothesis was that a combined program would be more efficacious than activity in isolation and that activity alone would also be effective compared to control group in improving adiposity profiles in overweight and obese adolescents, as well as family activity and feeding habits. Therefore, the results of the efficacy of FETA are expected to add to the literature of community-based programs, providing further support for the effectiveness of combined physical activity and nutritional interventions based on the parental involvement and modification of family habits.
Methods
Study Design
All students from the 15 public middle schools in the city of Larissa in central Greece were invited to measure their weight and height, to calculate their BMI. All the overweight or obese students were invited to take part in the study. The participation was free of charge for the children. Parents were informed about the purposes of the project and were asked to provide written informed consent for participation. It should be noted that despite all the participating schools being in urban area, several schools receive students from rural areas. Thus a number of adolescents were residents of rural areas. The study's protocol was approved by the Ethics Committee of the Medical Department of the University of Thessaly. The study was registered at clinicaltrials.gov (NCT02653508). The initial phase of FETA project has been previously published. 11
The flowchart of participation in the FETA is shown in Figure 1. One hundred eighty one adolescents were enrolled and randomized in the three groups of the study, by the same professional teacher of physical education who conducted the program. One hundred fifty remained at the end of the 6 months follow-up. One hundred and fifty children remained at the end of the 6 months follow-up, but 166 were included in the analysis using a modified intention-to-treat analysis. None of the subjects had an organic cause for his/her obesity and none received any medication, which would interfere with growth or weight control (e.g., corticosteroids and thyroid hormone).
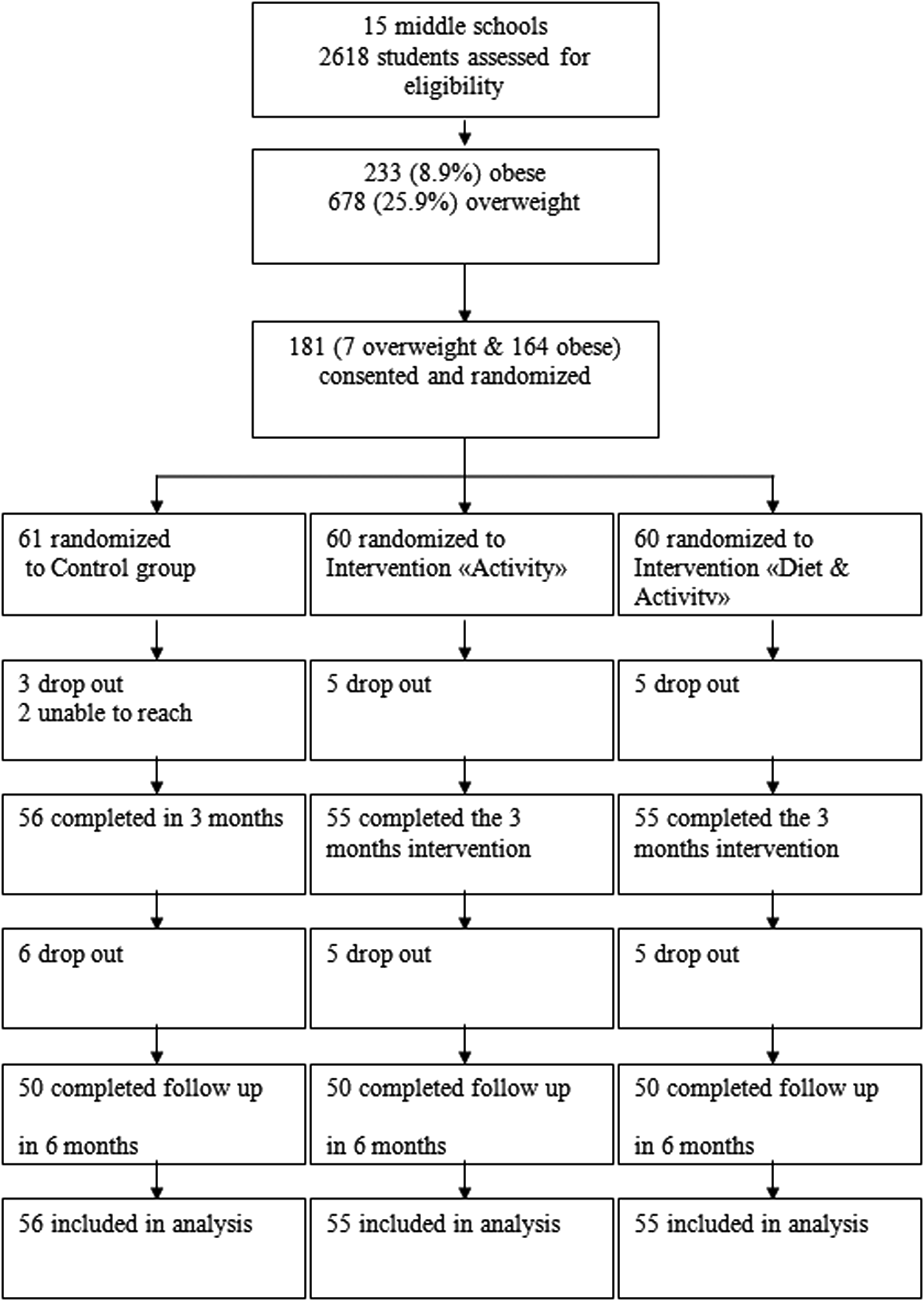
Flowchart of participation in the Feeding Exercise Trial in Adolescents and the number analyzed for primary outcomes.
Intervention
The FETA project involved one control and two intervention groups: a Physical Activity Skill Development Program (Activity) and a combination of a Dietary Information and a Physical Activity Skill Development Program (Diet & Activity).
Activity
All adolescents participated in a 3-day per week training program (45 minutes per training session) for 12 weeks. Training was directed by a professional teacher of physical education in a public training center. The training program was designed according to the type and intensity of exercise that school children normally perform. Many activities were delivered as games to encourage enthusiasm and participation. Endurance type activities accounted for most of the time spent in training (about 50% team sports and 50% running games), with attention to coordination and flexibility skills. To encourage adolescents' behavioral change, they were instructed to add an extra 30–45 minutes of walking or other sport activity of their preference at least once a week and to reduce inactivity (discouraging television watching and playing video games and encouraging the use of stairs instead of lifts and playing outdoors).
Diet and Activity
In addition, to the training sessions, the participants of the combined intervention attended a structured, nutritional education program. In the introductory meeting (45–60 minutes) general information was presented about the reasons behind childhood obesity, dietary and cooking habits, and the motivation for weight loss in an effort to involve the whole family in the “battle” against obesity.
During all the following meetings, before the initiation of the training sessions, 15 minutes were devoted to an interactive discussion with participants on the food pyramid, food choices, food labels, food preparation and cooking, eating habits, regular meals, and controlling environments that stimulate overeating. The topics discussed were given to the adolescents in the form of a printed notebook, while parents were also invited to attend these sessions. The discussions were led by the same person who performed the training session. On a weekly basis the parents attended the sessions with a participation rate from 60% to 90%.
Outcome Measures
All the outcomes measures were taken at baseline and every month until the end of the sixth month, when the 3-month follow-up period after the intervention ended.
Anthropometric measurements
Students were weighed on a digital scale twice, and the average was recorded. Participants removed shoes and jackets before heights and weights were measured using Tanita HD646 scales (Tanita Corporation of America, Inc.) to 0.1 kg. Height is measured to 0.1 cm using the stretch stature method and PE87 portable stadiometers (Mentone Educational Center). Body weight and height were measured using the same instruments, at the same place and day of the week, before the start of the day's program. Nonextensible steel tapes were used to assess waist circumference, which was measured at the level of the midpoint between the lower costal border and the iliac crest. All the anthropometric measures were conducted using the International Society for the Advancement of Kinanthropometry procedures. 12 BMI was determined according to the following formula: BMI = [weight/height 2 ]. We used the cutoff points for the BMI in childhood presented by Cole et al. to allow international comparisons with our findings in the prevalence of overweight and obesity. 13 Systolic blood pressure, diastolic blood pressure, and pulses per minute are measured using an automated blood pressure monitor (CRITIKON) under standardized procedures. 14
Fitness assessment
Pre- and postintervention evaluations (at 3 and 6 months) of physical fitness were based on the EUROFIT Test Protocol 15 designed by the Committee of Experts on Sports Research 16 that has been used in several European countries. The 50 m sprint Run Test that was used is a test for the evaluation of speed and was recorded in seconds. 17
Revised Family Eating and Activity Habits Questionnaire
The modified version of the Family Eating and Activity Habits Questionnaire (FEAHQ) was completed by parents and adolescents. 18 FEAHQ is a validated 32-item self-reported instrument designed to assess the eating and activity habits of family members, as well as obesogenic factors, in the overall home environment related to weight. FEAHQ is divided into four subscales: (a) Leisure time activity (four items: frequency of parents' and children's engagement in physical and sedentary activity), (b) Eating habits and style [12 items: eating while standing at the open refrigerator, or watching TV, or doing homework, or reading, following stress (frustration, anger, and boredom), or between meals; parental presence when the child is eating], (c) Response to internal hunger and satiety cues (three items: testing the family members' responses to hunger and satiety cues and assessing the eating initiator), and (d) Stimulus exposure and control (13 items: presence and visibility of snacks, sweets, cakes, and ice cream at home, boundaries of the child's autonomy in buying or taking these foods, and parents' presence during meals). 18 Scores were calculated separately for each member of the family. Higher numerical scores reflected less appropriate eating patterns.
Blinding
The randomized adolescents in each group were not aware of the existence of the other two study groups. The risk of participants realizing that there were other study groups was minimized by different attendance times and asking participants not to discuss their study experience until the completion of the follow-up, at 6-months from the initiation of the study.
Statistical Analysis
To detect a 0.28 standardized effect size from baseline to 6 months in BMI score for power of 80% at two-sided 5% level of significance and assuming a drop-out rate of 20%, a minimum sample size of 65 participants per group was required. Analyses were conducted on a modified intention-to-treat basis, which included all randomized participants who had a baseline and at least one postbaseline completed questionnaire, with the last observation carried forward.
Quantitative variables are presented as mean with standard deviation or with 95% CI (confidence interval), and qualitative variables are presented as frequencies with percentages. Chi-square test for qualitative variables and Kruskal–Wallis test or ANOVA for quantitative variables were used to compare baseline anthropometric characteristics, fitness, and score of the modified version of the Family Eating and Activity Habits Questionnaire among groups.
Linear mixed models (LMM) were used to evaluate the impact of intervention programs, time, and the program-by-time interaction on the child's measured outcomes over the 6-month period adjusting for the fixed effects of gender, age, and mother and father education levels and for the covariates of baseline value of the outcome variable and baseline of BMI score. LMM were performed using maximum likelihood estimation method, and Bonferroni correction was applied for multiple comparisons. Normality of model residuals was assessed using either Kolmogorov–Smirnov test or Shapiro–Wilk test without showing deviation from normality. Results were considered statistically significant when the p-value was less than 0.05. Data were analyzed using Epi Info (version 3.5.3; CDC) and SPSS 21.0 (IBM SPSS, Inc.).
Results
The baseline anthropometric characteristics, as well as the results on the Shuttle run test and the modified version of Family Eating and Activity Habits Questionnaire (FEAHQ) collected for the 181 adolescents, are presented in Table 1. In Table 2, the percentages and the absolute numbers of overweight and obese participants in each of the three groups from baseline to 3 and 6 months are presented. Both “Activity” only and “Diet & Activity” groups not only reduced their mean in BMI but also a significant percentage of obese became overweight in the two groups (Activity: p = 0.002, Diet & Activity: p < 0.001). No adverse events were observed in the intervention groups.
Baseline Characteristics of the 181 Adolescents of the Three Groups Who Remained Until the End of the 3 Months Program and the 3 Months Follow-Up
Data are mean with standard deviation (SD) unless otherwise stated.
Chi-square test or Kruskal–Wallis test or ANOVA.
FEAHQ, Family Eating and Activity Habits Questionnaire; BMI, body mass index; ns, not significant.
Percentages and the Absolute Numbers of Overweight and Obese Participants in Each of the Three Groups from the Baseline and Until the End of the 3 Months Program and the 3 Months Follow-Up
Chi-square test.
The changes in the outcome variables by group from baseline to 3 months and from baseline to 6 months are shown in Table 3. Both “Activity” only and “Diet & Activity” groups reduced statistically significantly (p < 0.001), at 3 months, their mean BMI [−1.1 and −1.4, respectively], waist circumference [−2.2 and −2.4, respectively], systolic blood pressure [−4.9 and −3.7], diastolic blood pressure [−4.6 and −4.2], pulses per minute [−16.0 and −16.7], and 50 m sprint test time [−0.4 and −0.4], while greater reductions were observed at 6 months [BMI: −2.3 and −3.1]. Significant changes in the total FEAHQ score, both in adolescents and parents, were achieved only in the “Diet & Activity” group at 3 months and at 6 months [−20.8 and −25.4]. In the Control group, significant increases (p < 0.001), compared to the baseline, were observed in BMI at 3 months, waist circumference at 3 and 6 months, in pulses per minute at 6 months, and at 50 m sprint run time both at 3 and 6 months.
Changes in Anthropometric Variables within Treatment Group of Adolescents (n = 150), from Baseline to 3 Months Program and Baseline to 3 Months Follow-Up
Time changes calculated as 3 months-baseline and 6 months-baseline.
Data are mean changes with 95% confidence intervals as estimated using LMM.
LMM, linear mixed models.
Differences in outcomes among the three groups at 3 and 6 months are presented in Table 4. Looking into differences in outcomes among the two intervention groups, compared with those in “Activity” only group, those in “Diet & Activity” group had a greater reduction in BMI at both 3 and 6 months and at FEAHQ scores of both adolescents and parents. Adolescents in both intervention groups, compared to those in the control group, achieved statistically significant (p < 0.001) reductions in all anthropometric parameters and at the sprint run test. However, for the FEAHQ scores only the participants of the “Diet & Activity” group achieved significant improvement at both 3 and 6 months compared to the control group. Finally, no adverse events were reported in any of the groups during the program or the follow-up phase.
Differences in Anthropometric Variables among the Treatment Groups at 3 Months Program and 3 Months Follow-Up
Time changes calculated as 3 months baseline and 6 months baseline.
Data are differences of means with 95% confidence intervals as estimated using LMM.
Discussion
The FETA study demonstrated that a community intervention introducing modest intensity supervised activity combined with a parents-involving, nutritional education program was the most efficacious in reducing BMI in overweight and obese adolescents at the end of the 3 months program and maintaining the reduction at the 3 months follow-up after the intervention. Significant reduction in BMI was also achieved by the Activity in isolation program, while waist circumference, blood pressure,19,20 pulses per minute, 21 and performance in fitness tests were also improved significantly in both intervention groups compared to the Control group, both at the end of the program and at the 3 months follow-up. The combined program resulted in significantly modifying all the family eating and activity habits toward healthier patterns, including activity level, stimulus exposure, eating related to hunger, and eating styles, while the Activity in isolation achieved to influence only the activity related habits, both retaining the positive effects at the 3 months follow-up.
Our results support the hypothesis that the intervention groups would both achieve a reduction in BMI compared to the control group and that the combination Activity and Diet program is more efficacious than the Activity program in isolation. Although a recent review has shown that only four out of the nine community interventions on overweight and obese children have showed significant improvement in reducing BMI, 5 our study has reinforced the effectiveness of such treatment interventions. Our results are in line with findings indicating that programs targeting dietary modifications perform significantly better than the activity interventions in isolation. 22 Moreover, the combination of interventions in obesity programs has also been suggested to have higher probability to be effective, by providing information on behavior-to-health links, prompting practice and planning social support. 7
Developing a community program with parents' involvement was found to be an effective way to influence parental behavior toward family eating and activity habits. Actively involving parents, by asking them to bring their children thrice a week during the period of the intervention and attend dietary modification instructions at the diet and activity group, was found to be an effective strategy to achieve change in family habits, developing a healthier lifestyle. Family-based approaches to pediatric obesity treatment are considered the “gold-standard,” 8 since the role of parents as key agents of change in the treatment of childhood obesity has been previously studied, showing superiority to approaches focusing only on children.7,9,10,23 Moreover, parental support should be encouraged, since it is fundamental for the continuation of any community and for most of the school-based programs. 4 Our study provides further evidence, building on the long-established approach of family-based treatment, since parents seem to have a key role in developing a healthier lifestyle with a number of different ways. Their food preferences, the quantities and variety of foods in the home, the parents' eating behavior, and the parents' physical activity patterns are inevitable parameters that create an environment in which obesity may or may not be prevented. 9
The main strength of our study is that it is one of the few internationally 3-arm parallel group, prospective cohort studies that have evaluated the efficacy of a community program with activity in isolation and combined dietary information and activity in overweight and obese adolescents. One limitation of the study is that the randomization, the training, and the follow-up measurements were conducted by the same person, the physical education teacher. Although this may raise blinding issues and an observation bias, having the same person in the training of all groups and in conducting all the measurements can ensure homogeneity in the procedures that were followed. Another limitation of this study is that the follow-up phase was limited to 3 months after the end of the program. However, it should be outlined that our study is among those that have provided even a short-term follow-up. Since few studies have assessed long-term outcomes, it is difficult to draw on any previous studies to predict the long-term success of FETA.10,24,25 However, based on our promising short-term follow-up results, we believe that our intervention could have a high possibility to maintain long-term changes that should be assessed in the near future.
Conclusions
In conclusion, FETA was a 12-week community intervention that resulted in significant effects on improving adiposity profiles in overweight and obese adolescents, as well as family activity and feeding habits, maintained at 3 months follow-up. This low cost, family-involving intervention has shown to be suitable for delivery in community settings, even in countries facing economic restrictions, although further work is required to test whether its effectiveness is sustained in the long term. The FETA study's findings add further support for the effectiveness of community, combined physical activity, and nutritional interventions based on the parental involvement and modification of family eating and activity habits.
Footnotes
Acknowledgments
This study was part of a PhD dissertation supported by University of Thessaly, Faculty of Medicine, and School of Health Sciences. The authors express their sincere gratitude to the participants in the study and their families, who generously provided their time and trust.
Author Disclosure Statement
The authors declare no conflict of interest.