
Abstract
Abstract
Background:
The aim of this study is to determine if sleep duration in early childhood is associated with cardiometabolic risk (CMR) in later childhood as assessed by a CMR cluster score [sum of age- and sex-standardized z-scores of waist circumference (WC), systolic blood pressure, triglycerides, glucose, and (inverse) high-density lipoprotein (HDL)]. Secondary objectives included examining sleep duration and the individual CMR factors and BMI z-score.
Patients and Methods:
A prospective cohort study was conducted using data from the TARGet Kids! practice-based research network in Toronto, Canada. Children (n = 597) with parent-reported 24-hour sleep duration in early childhood (12–36 months) and a follow-up visit (36–96 months) with all five CMR factors were included in the analysis. Multivariable linear regression was used to assess the relationship between early childhood sleep duration and later childhood CMR, adjusting for relevant covariates.
Results:
Average 24-hour sleep duration in early childhood [mean age: 28.1 (6.6) months] was 11.8 (1.4) hours, with 87% meeting or exceeding total sleep recommendations for their age. Sleep duration in early childhood was not associated with the CMR cluster score in later childhood. Shorter sleep duration was associated with higher HDL concentrations [adjusted β = −0.028 (95% confidence interval: −0.049 to −0.007), p = 0.009].
Conclusions:
Further research is needed to determine if early childhood sleep duration is associated with HDL in later childhood. Future studies, which investigate sleep quality in addition to sleep duration, may be helpful.
Introduction
Sufficient sleep duration and good quality of sleep are important in the regulation of metabolic and hormonal processes involved in childhood growth and development. 1 However, average daily sleep duration in children and adolescents has declined by ∼70 minutes in the past century. 2 Consequences of insufficient sleep reach beyond physical health and include poor academic performance, emotional and social problems, and risk-taking behaviors in children and adolescents.3,4
Short sleep duration in children and adolescents is associated with increased BMI.5–10 Overweight or obesity in childhood is common, 11 it tracks into adulthood, 12 and is associated with cardiometabolic diseases such as type 2 diabetes and cardiovascular disease later in life.13,14 Short sleep duration is also associated with cardiometabolic risk (CMR) factors in children such as high blood pressure,15,16 dyslipidemia,17,18 and glucose homeostasis.19–21 Understanding the association between sleep and CMR in early childhood is critical as sleep in childhood may be a modifiable risk factor for cardiovascular disease later in life.
Since metabolic syndrome cannot be calculated in early childhood, continuous CMR scores, which combine components of the adult metabolic syndrome, 22 have been developed and used in studies assessing CMR in children and adolescents.20,21,23–29 However, few studies have assessed sleep duration and its association with such a score.20,21,28 Furthermore, there is a paucity of data assessing this relationship longitudinally in young children.10,30 Accordingly, the primary objective of this study was to prospectively evaluate if sleep duration in early childhood (at ∼2 years) was associated with CMR in later childhood (at ∼4.5 years) as assessed by a CMR cluster score. Secondary objectives included examining the relationship between sleep duration and the individual risk factors of the CMR cluster score and BMI.
Patients and Methods
Study Design and Population
A prospective cohort study was conducted using data from TARGet Kids! primary care practice-based research network (www.targetkids.ca).31–33 Between December 2008 and February 2016, children 0–6 years of age were recruited from 10 pediatric or family practice primary care clinics in Toronto, Canada. Children in TARGet Kids! are recruited at any age up to 6 years and followed at scheduled well-child visits at <6, 6–12, and 18 months and annually from 2 years of age on.
Inclusion and Exclusion Criteria
Children were included if they were considered healthy by parent report and had at least two visits (one between 1 and 3 years old and one between 3 and 8 years old). Children were excluded if they had severe developmental delay, health conditions affecting growth, acute or chronic illness (other than asthma), or were unable to complete English questionnaires. For this analysis, we excluded children who did not have reported sleep duration between 1 and 3 years of age and a waist circumference (WC), blood sample, and blood pressure measurement at 3–8 years of age. If multiple visits met the inclusion criteria, we chose the visit closest to 2 years as baseline for sleep duration and covariates and the last available visit between 3 and 8 years as follow-up for CMR. Consent was obtained from parents. This study was approved by the Research Ethics Boards at The Hospital for Sick Children and St. Michael's Hospital (www.clinicaltrials.gov, NCT01869530).
Exposure Variable
The primary exposure was 24-hour sleep duration measured between 1 and 3 years. Sleep duration was assessed using parent-reported questionnaires derived from the Canadian Community Health Survey. 34 Parents answered the question, “How many hours does your child usually spend sleeping in a 24-hour period?” in hours. To evaluate whether children met sleep recommendations for their age set by the National Sleep Foundation, 35 we presented descriptive characteristics stratified by the recommended sleep durations for various age groups. For toddlers 1–2 years old, 11–14 hours of daily sleep are recommended; for preschoolers 3–5 years old, 10–13 hours are recommended and the lower values of these ranges were used as cut points.
Outcome Variables
Cardiometabolic measures
The primary outcome (measured between 3 and 8 years of age) was a continuous CMR cluster score quantified as the sum of z-scores from WC, systolic blood pressure (SBP), glucose, triglycerides, and (inverse) high-density lipoprotein (HDL). The z-scores were calculated using the mean and SD within our population as has been done in other cohorts. 36 The inverse of HDL was used in the score since higher HDL is indicative of a better metabolic profile. A lower CMR cluster score indicates lower CMR. Similar CMR scores have been used in the literature to assess CMR in children and adolescents.20,21,23–29 Secondary outcomes were the individual components of the CMR cluster score (WC, SBP, glucose, triglycerides, HDL) and BMI z-score.
At every well-child visit, height, weight, and WC were measured by trained research staff using standardized guidelines. 37 Weight was measured using calibrated precision digital scales (Seca, Hamburg, Germany). Standing height was measured using a stadiometer (Seca, Hamburg, Germany) or, for children under 2 years, child length was measured using a length board. BMI was calculated as weight in kilograms divided by height (or length) in meters squared. Age and sex-adjusted BMI z-scores were defined using the World Health Organization standards for growth in children 38 as recommended in Canada. 39 Overweight was defined as a BMI z-score between 1.0 and ≤2.0, and obese was defined as >2. 39 Trained research assistants measured blood pressure annually in children 3 years and older at the time of the child's clinic visit (between 9am and 6pm). Readings were interpreted according to the guidelines of the National High Blood Pressure Education Program. 40
Glucose, triglycerides, and HDL were measured from nonfasting blood samples collected in the primary care office by experienced pediatric phlebotomists. Obtaining fasted blood samples from preschool children in a clinical setting for research purposes is challenging; however, previous studies, 41 including ours, 42 have shown that duration of fasting has minimal impact on lipids and glucose in children. Blood specimens were transported immediately to Mount Sinai Services Laboratory, Toronto, Canada, for analysis using standard procedures (www.mountsinaiservices.com).
Glucose was measured using the enzymatic reference method with hexokinase; triglycerides and HDL were measured using enzymatic colorimetric on the Roche Modular platform (Roche Diagnostics, Laval, Canada). All data were uploaded to the central MediData Rave platform (MediData Solutions, New York) and housed at the Applied Health Research Centre of the Li Ka Shing Knowledge Institute, St. Michael's Hospital (Toronto, Canada).
Covariates
Covariates identified as potential confounders were determined a priori from the literature. Covariates that were collected at the same time as sleep duration (the primary exposure) included child's sex, birth weight, maternal ethnicity, median neighborhood household income from postal code, BMI of the parent who attended the visit, child's age, outdoor free play time (in minutes), juice and sugar-sweetened beverage (SSB) consumption (in daily cups), and bottle use in bed. Maternal ethnicity was determined for the biological mother through a questionnaire with 20 response options 43 and was then categorized into four categories: European, East Asian/Southeast Asian, South Asian, and Other. Daily juice and SSB consumption was determined by summing the number of cups on a typical day for 100% juice, sweetened drinks, and soda or pop. Bottle use was determined by asking, “Does your child use a bottle in bed?” and responses were dichotomized to no/yes.
Statistical Analyses
All analyses were conducted using SAS software, version 9.3 (SAS Institute, Inc., Cary, NC). Descriptive characteristics were stratified by the recommended sleep duration for age. Differences between groups were assessed using chi-square and t-tests for categorical and continuous variables, respectively.
Linear regression was used to model the association between early childhood sleep duration and CMR in later childhood. For clinical relevance, secondary outcome variables (WC, HDL, glucose, and triglycerides) were dichotomized and the odds ratio and 95% confidence interval (CI) were estimated using logistic regression models. Cut points for high risk were defined as follows: <1.17 mmol/L for HDL, >0.84 mmol/L for triglycerides based on pediatric guidelines, 44 and >90th percentile within our sample for WC and glucose due to no established reference. There was insufficient sample size for SBP >90th percentile as defined by NHANES.40,44 Multivariable linear and logistic regression models included all covariates, and models with HDL, glucose, and triglycerides were additionally adjusted for time of blood collection and fasting time since last meal/snack in hours.
All variables had levels of missing <10%. Multiple imputation analysis was used to impute missing values of covariates and secondary outcome BMI z-score using the fully conditional specification method. Predictive mean matching was used for continuous variables and logistic regression and discriminant approach for dichotomous and categorical variables, respectively. Results of the 50 imputation datasets were combined and the parameter estimates (95% CI) for the adjusted pooled models were reported. All statistical tests were two-sided and statistical significance was defined as p < 0.05.
Results
Exposure and Outcome Time Point in Early Childhood
There were 4822 children with multiple visits in the TARGet Kids! cohort (Fig. 1). Of these, 2527 had visits during the specified exposure and outcome time periods, of which 1681 had a sleep duration measurement between 12 and 36 months. One or more CMR score components were missing between 36 and 96 months for 1084 children, therefore the final analysis included 597 children.
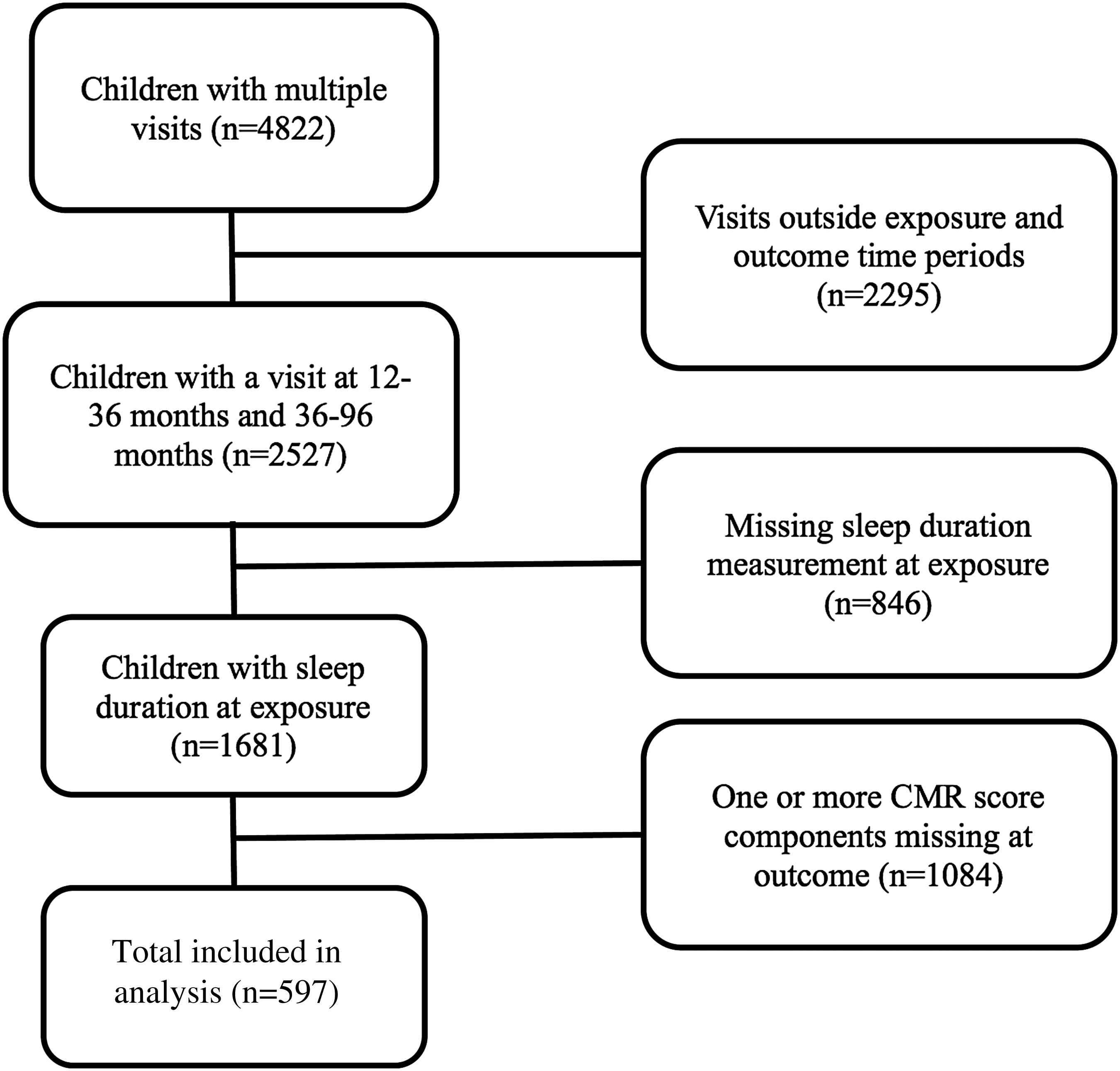
Study participant flowchart.
Descriptive characteristics of the study population stratified by the recommended sleep cut point in early childhood are shown in Table 1. Children were on average 28.1 (6.6) months at baseline. Overall, 79 (13%) children were below and 30 (5%) children were above the recommended sleep range for age. Children meeting or exceeding the recommended sleep range were older (p = 0.04), had less nighttime bottle use (p = 0.002), and were more likely born to mothers of European descent (p = 0.02) compared with children below the recommended sleep range. Seventeen percent and 4% of children were overweight (1 < BMI z-score ≤ 2) or obese (BMI z-score >2), respectively, between 12 and 36 months of age. The mean age at follow-up was 54.8 (14.8) months, with an average time period between exposure and outcome of 26.7 months. There were no significant differences between age or outcome variables between those below or above the recommended sleep range cut point.
Descriptive Characteristics of Participants Stratified by Below or Equal to/Above the Recommended Sleep Range at 12–36 Months of Age
Significant differences between sleep cut point groups using *Pearson's chi-square test and **two-sample t-test.
Data presented as mean (SD) or frequency (percentage).
Recommended sleep cut point is ≥11 h/day for 12 to <36 months of age and ≥10 h/day for 36 to <60 months of age (Ref. 35 ).
Maternal ethnicity group “Other” contains African, Afro-caribbean, Latin, Arab, North African, West Asian, Aboriginal, and Mixed.
Outcome variables measured between 3 and 9 years of age.
BMI z-score, age- and sex-standardized body–mass index; BP, blood pressure; CMR, cardiometabolic risk; HDL, high-density lipoprotein; SSB, sugar-sweetened beverage; WC, waist circumference.
Association between Early Childhood Sleep Duration and CMR Score in Later Childhood
At follow-up, the mean CMR cluster score was −0.22 (2.44), ranging from −7.05 to 9.06. The CMR score increased with increasing BMI z-score categories at follow-up (Table 2). The average CMR cluster score was more favorable in girls [−0.50 (2.42)] than boys [0.00 (2.44)] (p = 0.01).
CMR Cluster Score by BMI z-Score Category in Later Childhood, n = 569
Underweight (n = 2) and normal (n = 475) BMI z-score.
Data presented as mean (95% CI).
Overall, there was no significant association between sleep duration in early childhood and CMR cluster score in later childhood (Table 3). Secondary analyses of the individual components and BMI z-score yielded one association: later childhood HDL was significantly associated with early childhood sleep duration; however, the relationship was in the unexpected direction [−0.032 mmol/L (95% CI −0.051 to −0.013), p = 0.0008]. This relationship remained significant in multivariable models [−0.028 mmol/L (95% CI −0.049 to −0.007), p = 0.0092] after adjusting for maternal ethnicity, parental BMI, median income from postal code, child's sex, birth weight, age difference between exposure and outcome, early childhood BMI z-score, juice and SSB consumption, outdoor free play, bottle use in bed, time of blood collection, and fasting hours.
Linear Regression Analysis between Sleep Duration in Early Childhood and Cardiometabolic Outcomes in Later Childhood, n = 597
Model adjusted for maternal ethnicity, parental BMI, median after-tax income, child's sex, birth weight, age difference between exposure and outcome, baseline BMI z-score, juice or sugar-sweetened beverage consumption, outdoor free play time in minutes, and bottle use in bed.
Models with CMR cluster score, HDL, triglycerides, and glucose further adjusted for time of blood collection and fasting hours.
Using age- and sex-standardized components of the CMR cluster score instead of nonstandardized values yielded the same associations; HDL was significantly associated with sleep duration, while all others remained nonsignificant. Using logistic regression, sleep duration was not associated with the risk group for any of the cardiometabolic measurements (Supplementary Table S1; Supplementary Data are available online at www.liebertpub.com/chi).
Discussion
This prospective longitudinal analysis suggests that 24-hour sleep duration in children 1–3 years old was not associated with a CMR cluster score in later childhood. Furthermore, in secondary analyses, components of the CMR cluster score and BMI z-score in later childhood were not associated with 24-hour sleep duration except for HDL concentrations; however, this was not in the expected direction.
To the best of our knowledge, this is the first study to assess sleep duration and CMR using a cluster score in early childhood. The evidence to date examining CMR factors is more abundant in older children and adolescents. 10 Furthermore, the most convincing evidence appears to be with inadequate sleep duration and increased adiposity.10,30 Therefore, our lack of statistically significant findings suggests that CMR factors at ∼4.5 years of age is potentially too early to detect an association with early sleep duration.
Although there is no consensus on the definition of CMR in childhood,45–48 numerous CMR scores have been developed20,21,24–29,36,49,50 in the absence of a metabolic syndrome definition in children younger than 10 years of age. 51 Components of our score were previously identified using principal component analysis in children 3–5 years of age in the TARGet Kids! cohort. 33 These factors align well with the five factors used to define and diagnose metabolic syndrome in adults. 52
A small number of studies using a CMR score as the primary outcome in cross-sectional 28 and longitudinal20,21 analyses have shown sleep duration to be associated with various scores in older children and adolescents. In obese adolescents, objectively measured total sleep duration was inversely associated with a cMetScore [sum of age- and sex-standardized scores of WC, mean arterial pressure, (inverse) HDL, triglycerides, and glucose]. 28 In Danish children 8–11 years old, short sleep duration (assessed by actigraphy and sleep logs) was associated with a higher metabolic syndrome score [sum of age-, sex-, and pubertal status-standardized scores of WC, mean arterial pressure, HOMA-IR, triglycerides, and (inverse) HDL] following a 200-day follow-up period 21 ; however, no association was found in the cross-sectional analysis. 21 Last, a continuous sleep curtailment score (parent-reported sleep duration) from 6 months to 7 years of age was inversely associated with a metabolic risk score [sum of age- and sex-standardized scores of WC, SBP, (inverse) HDL, and log-transformed triglycerides and HOMA-IR] at age 7; however, this relationship was attenuated after adjusting for mid-childhood BMI z-score. 20 None of these studies evaluated CMR before 7 years of age.
While our finding between sleep duration and HDL was in the unexpected direction, interestingly, similar trends have been reported in other pediatric studies. In obese adolescents, longer parent-reported sleep duration was associated with lower HDL concentrations 53 and the beta coefficient was similar in magnitude to our study. However, their relationship was not statistically significant when sleep was self-reported or measured using actigraphy. Another study in girls 11–12 years of age identified that the sleep pattern, late to bed/early rise, was also associated with higher HDL concentrations. 54 The magnitude of association in these previous studies53,54 and our current study was small (all betas <0.10) and we cannot rule out the possibility of chance findings. However, although there is no clear mechanism as to why shorter sleep duration is associated with higher HDL cholesterol, it is possible that sleep quality may play a role. Disruptions in circadian rhythms and subsequent poor quality sleep may contribute to dyslipidemia. 55 For example, in nonobese children with sleep-disordered breathing, HDL concentrations were significantly higher than controls 56 ; however, this was not shown elsewhere. 57 Sleep quality data were not available to evaluate for our analysis.
This study is one of few to report on total sleep duration in children younger than 3 years of age. Parent-reported 24-hour sleep duration in our cohort (∼12 hours) is comparable with previously reported durations in a similar age range.58–60 Regarding sleep recommendations, 35 less than 15% of our participants were below, while 5% exceeded, the age-specific sleep recommendation ranges. A recent analysis of 24,896 nationally representative older children and adolescents in Canada reported that nearly 30% of children aged 10–13 years were below the recommended sleep amount, while only 1% exceeded the sleep recommendation. 61 There are limited published data in Canada for children younger than 6 years. 62
Existing evidence for the relationship between sleep and CMR has been mainly cross sectional, thus temporality cannot be established, and has been in older children and adolescents. A major strength of this study is the prospective analysis of sleep duration and CMR in very young children. Limitations include parent-reported sleep duration instead of measuring sleep objectively63,64; however, a validation study has shown good agreement between actigraphy and parent-reported sleep measurements. 65 Nonetheless, our analysis may have been strengthened with additional data on sleep quality, consistency, and details on daytime naps. We also used nonfasting blood samples, which may affect concentrations of glucose and triglycerides. However, HDL concentrations appear to be less influenced by fasting status.41,66 We controlled for this possibility by adding fasting time before blood work as a covariate and the results did not change.
Since CMR cluster scores are standardized based on the population studied, the score is cohort specific. Scores can only be compared between studies when the two samples have analogous demographics, data distribution, and variability and the scores are derived and calculated from the same variables.36,67 Furthermore, each score component is not weighted and therefore is considered equally important in CMR, which may not be appropriate. 67 Finally, our cohort consisted of primarily healthy urban children with mothers who reported European ethnicity and therefore our results may not be generalizable to other populations.
Conclusion
Our findings suggest that sleep duration between 1 and 3 years of age is not associated with a CMR score ∼2 years later; however, there may be a relationship with CMR in older childhood not captured in our analysis. Furthermore, sleep quality may be more important than sleep duration on cardiometabolic disease risk in young children. Further research is needed to confirm these findings in addition to the unexpected association between longer sleep duration and decreased HDL concentrations. Finally, future longitudinal studies are warranted to determine if early childhood sleep predicts CMR into adolescence and adulthood.
Footnotes
Acknowledgments
The authors thank all of the participating families for their time and involvement in TARGet Kids! and are grateful to all practitioners who are currently involved in the TARGet Kids! practice-based research network. Advisory Committee: Eddy Lau, Andreas Laupacis, Patricia C. Parkin, Michael Salter, Peter Szatmari, and Shannon Weir. Research Team: Charmaine Camacho, Arthana Chandraraj, Dharma Dalwadi, Ayesha Islam, Thivia Jegathesan, Tarandeep Malhi, Megan Smith, and Laurie Thompson. Applied Health Research Centre: Christopher Allen, Bryan Boodhoo, Judith Hall, Peter Juni, Gerald Lebovic, Karen Pope, Jodi Shim, and Kevin Thorpe; Mount Sinai Services Laboratory: Azar Azad. Funding of the TARGet Kids! research network was provided by the Canadian Institutes of Health Research (CIHR) Institute of Human Development, Child and Youth Health, the CIHR Institute of Nutrition, Metabolism and Diabetes, the SickKids Foundation, and the St. Michael's Hospital Foundation. The Pediatric Outcomes Research Team is supported by a grant from The Hospital for Sick Children Foundation. The funding agencies had no role in the design and conduct of the study, the collection, management, analysis, and interpretation of the data, or the preparation, review, and approval of the manuscript.
Author Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.