
Abstract
Abstract
Background:
Youth with disabilities are at increased risk for obesity compared with their typically developing peers and face unique barriers to healthy lifestyles. A limited number of weight management programs have been specifically tailored to accommodate youth with disabilities, and outcomes research in this population is scarce. We investigated the effectiveness of a specialized multidisciplinary weight management program for children with disabilities.
Methods:
Youth (N = 115) ages 2–18 years (mean age = 10.46) and their families receiving care in the Special Needs Weight Management Clinic (SNWMC) were followed over a period of 12 months. Child height and weight were measured by trained clinicians and used to calculate Body Mass Index z-scores (BMIz). A two-level multilevel model was estimated with repeated measurements of BMIz nested within patients.
Results:
Significant BMIz reductions of 0.02 per month were observed over the course of treatment when controlling for child age and baseline BMIz. A significant interaction between child age and time revealed that younger (vs. older) children exhibited greater decreases in BMIz over the course of treatment. Sex, ethnicity, disability diagnosis, and insurance moderated change in BMIz over the course of treatment.
Conclusions:
Outcomes of the SNWMC revealed significant decreases in BMIz with <5 sessions on average over 12 months and indicated the increased efficacy of early intervention in youth with disabilities. Future research should continue to modify interventions for families with adolescent children with disabilities as well as investigate additional variables that may impact success in treatment.
Introduction
Youth with disabilities, such as autism spectrum disorder (ASD), Down syndrome, intellectual disabilities, and physical disabilities, are at increased risk for obesity compared with their typically developing peers. 1 The National Survey of Children's Health has indicated that obesity occurs among 16.4% of youth with ASD compared with 9.9% of youth without ASD, and an ASD diagnosis is associated with a 1.76 greater likelihood of having obesity. 2 Maïano et al. 3 found adolescents with intellectual disabilities to have 1.8 times the risk of developing obesity than their typically developing peers. Furthermore, Rimmer et al. 4 calculated odds ratios for pediatric obesity across a number of developmental disabilities and found children with ASD and Down syndrome to be at increased risk (odds ratios of 2.19 and 3.0, respectively).
Several reasons have been hypothesized for an increased risk of obesity in youth with disabilities compared with their typically developing peers. Children with ASD experience significantly more feeding problems compared with peers, 5 as well as nutritional problems such as limited diet variety with higher food selectivity, 6 lesser consumption of fruits and vegetables, 7 and greater preference for snack foods. 8 Youth with disabilities may also experience metabolic abnormalities due to the prescribed psychotropic medications, which play a role in overconsumption and weight gain.1,9,10 Finally, youth with disabilities may have difficulty engaging in physical activity due to the physical complications of their diagnoses. Individuals with disabilities experience impairments in motor skill components such as balance, perceptual issues, and hand–eye coordination that can significantly impact their physical activity.10–12 Youth with Down syndrome exhibit low muscle tone, specifically in their legs, which affects their muscular strength to engage in certain exercises. 13
Despite these unique barriers and increased risk for obesity among youth with disabilities, there is no “gold standard” treatment for pediatric obesity in this population. For typically developing children, the “gold standard” treatment for obesity is a multidisciplinary, behavioral-based approach that incorporates the child's family into the behavior change process.14,15 Irby et al. 16 as well as Holcomb et al. 17 have offered several recommendations on strategies to adapt existing weight management programs for populations with disabilities. Specifically, adaptations have included involving parents as well as children while developmentally appropriate, utilization of a multidisciplinary team, collaboration with other medical providers, and setting realistic expectations for treatment goals. Finally, they advocate that treatment recommendations need to take into account an appropriate pace of behavior change, given food variety, texture, and behavior challenges.16,17
A limited number of weight management programs exist, which have been specifically tailored to accommodate youth with disabilities, and outcomes research in this population is scarce. Curtin et al. 18 assessed the effectiveness of adding a behavioral skills parent training to a nutrition and physical activity education group intervention for adolescents with Down syndrome. Results indicated the addition of the behavioral skills parent training compared with receiving education alone resulted in greater weight loss at 6 and 12 months, greater moderate/vigorous physical activity time at 6 months, and greater vegetable intake at 12 months. 18 Irby et al. 16 provided a description of a multidisciplinary, family-centered, tertiary-care pediatric weight management program and presented a case series of three examples where treatment was modified to meet the needs of children with cognitive disabilities and their families, resulting in improved nutrition, increases in physical activity, and reductions in Body Mass Index z-scores (BMIz). Brown et al. 19 examined the effectiveness of this specialized weight management program in youth with and without disabilities and found that those with disabilities lost significantly more weight at 4 months compared with their typically developing peers.
Gillette et al. 20 reported on a multidisciplinary intervention tailored to treat obesity among youth with disabilities. Results showed a significant decrease in BMIz at the 6-month follow-up and a trend toward the youngest children having more significant BMIz changes. Results of this initial evaluation were limited by relatively high attrition rates at the 6-month follow-up, although not atypical of those seen in clinical weight management samples. 21 The present study aimed to address some of the limitations from the initial study and extend the follow-up time period. Study aims included (1) examining the overall trajectory of BMIz over the course of treatment, and (2) exploring patient characteristics (i.e., disability diagnosis, age, sex, ethnicity, and insurance status) that may be predictive of differential trajectory of BMIz over the course of treatment.
Methods
Participants
Inclusion criteria for the study included youth between the ages of 2 and 18 years; diagnosis of ASD, Down syndrome, intellectual disabilities, or physical disabilities; BMI ≥95th percentile based on age and gender norms; and English or Spanish as a primary language. Most of the youth arrived at clinic were already diagnosed with one of the primary diagnoses categories. In the case that youth had not received a specific diagnosis, they were placed into one of the categories for the purposes of analyses based on the diagnosis codes documented in the primary psychologist's documentation in the medical record. All children and families received care as part of a multidisciplinary clinical obesity treatment program in the Special Needs Weight Management Clinic (SNWMC) at a Midwest children's hospital. Requirements for clinic entry were the same as the inclusion criteria for the study, except for the requisite of English or Spanish as a primary language to complete the research consent process. Patients were referred to the SNWMC for specialized weight management by primary care providers and subspecialists locally and within approximately a 4-hour region. Data collection procedures in the SNWMC were approved by the hospital's Institutional Review Board. All patients attending the SNWMC who met inclusion criteria for the study were asked to provide consent for their clinic outcome data to be accessed for research purposes. All families signed informed consent before their data being used for any research purposes.
Of the eligible patients, 96% consented to participate in the research study. Youth who only completed an initial session and did not return for treatment were excluded from analyses (17%). Patients who completed only an initial session were more likely to be male and have a diagnosis other than physical disability in comparison with those who completed more than 1 session; there were no differences on any other demographic variables between groups.
Measures
Medical record review
Demographic data, including disability diagnosis, age, sex, ethnicity, and insurance status, were abstracted from the patient medical records and entered into the research database by a trained research assistant. If a patient presented to the SNWMC with more than one disability diagnosis, the leading pediatric psychologist on the team determined which diagnosis was the most predominant in terms of impacting eating-, weight-, and health-related behaviors. For example, if a child presented with both ASD and Down syndrome, the latter would be determined the predominant diagnosis due to the comorbid presence of significant metabolic abnormalities that play a significant role in overconsumption and weight gain.9,13
Anthropometric data
Child height and weight were measured at each SNWMC visit by a care assistant or a registered nurse who was trained in standardized procedures to obtain height and weight in youth with obesity and disabilities.
Weight at SNWMC visits was measured with patients in light clothing and shoes removed on a digital scale (Scale-Tronix, Wheaton, IL) and recorded to the nearest 0.1 kg. Height at visits was measured with patients standing without shoes, with their backs facing a wall-mounted stadiometer (Accurate Technology, Inc., Fletcher, NC) and head positioned in the Frankfort plane and was recorded to the nearest 0.1 cm. Height and weight measurements were used to calculate BMI, BMIz, and BMI percentile using the CDC BMI calculator for statistical analysis software program (available at www.cdc.gov/nccdphp/dnpao/growthcharts/resources/sas.htm).
Intervention
Intervention details are more fully described in Gillette et al. 20 The SNWMC is a hospital-based clinical treatment program providing multidisciplinary assessment and treatment for children and adolescents with disabilities and obesity and their families. Providers include a medical professional (MD, Pediatric Nurse Practitioner), pediatric psychologist, occupational therapist, and registered dietitian. Care is delivered in a team-based format with all providers participating in the appointments at the same time. Participants are scheduled for follow-up visits on the approximate time line as noted below, but these vary based on clinic availability and patient/family need. At the initial appointment, a complete medical, behavioral, feeding, sensory (related to feeding behaviors), and dietary history is obtained, and treatment goals and recommendations are provided taking into account the unique challenges of the child. For example, children with Down syndrome and physical disabilities receive diet plans that are ∼20% to 30% lower than would be expected based on their weight. We utilize indirect calorimetry to assist with diet planning when more detail is needed. All patients are taught balanced eating utilizing MyPlate, behavioral principles of making small, but noticeable changes, environmental controls, food scientist or other methods to assist with acceptance of new healthier foods, and increasing physical activity. At subsequent sessions, response to treatment is assessed, and additional recommendations are provided utilizing a gradual behavioral approach.
Appointment Schedule Flow
Appointments were scheduled based on clinical needs and availability and occurred at baseline, (∼6 weeks, 3 months, 6 months, 12 months). Visit data were included at each time point in the research dataset if they fell within a range of these target points (±1 month from time points during first 6 months of treatment and ±2 months during 12-month follow-up; see Fig. 1). Visit data were only included in one time window. Given that these time points were approximate and their windows fairly wide, a more precise time variable was created indicating the number of days and months since baseline that each measurement was taken.
Appointment schedule flow.
Statistical Analyses
The goal of the present study was to assess long-term outcomes as well as differential outcomes of the SNWMC based on patient characteristics (i.e., disability diagnosis, age, sex, ethnicity, and insurance status). Patients who were within or past the 12-month follow-up window (i.e., 12 ± 2 months since their initial treatment appointment in the SNWMC) were considered eligible for 12-month follow-up and included in analyses. A multilevel model (MLM) was used to test patient-level change in BMIz between baseline and 12-month follow-up. MLM was deemed appropriate for longitudinal analysis as it can use all available data, properly account for the correlation between repeated measurements of BMIz on the same patient, handle missing data adequately without the need for data imputation, flexibly model fixed and random time effects, and allow for examination of between-patient moderator effects by including cross-level interactions. 22 As such, all participant cases were retained in analyses despite attrition, which reduces the risk for biased outcome estimates in long-term programs resulting from participant drop-out. The model specified was person-level repeated measures of BMIz (level 1) nested within individuals (level 2), controlling for baseline BMIz and patient characteristics (i.e., disability diagnosis, age, sex, ethnicity, and insurance status), using a random slope and intercept and a homoscedastic error structure (i.e., scaled identity). A variable representing the number of months since baseline for each anthropometric measurement was entered into the model to examine linear change in BMIz over treatment. This linear measurement was squared to create a second time variable that was entered into the model to examine quadratic change in BMIz over treatment. Several possible interactions were also explored to identify whether patient characteristics relate to differences in the trajectories of BMIz change over the course of treatment. Interactions between the linear time variable and the following patient characteristics were examined while controlling for baseline BMIz: disability diagnosis, age, sex, ethnicity, and insurance status. It is important to note that child age was transformed to z-scores to aid with interpretation.
Analyses were completed in SPSS version 23.0 (SPSS, Inc., Chicago, IL) using the MIXED procedure and the full information maximum likelihood estimator. This estimator was deemed appropriate over others (e.g., restricted maximum likelihood) as it allows for the calculation and comparison of fixed effects in nested models, which are the primary variables of interest in the current study. 23 Furthermore, this estimator can appropriately address missing data in longitudinal analyses when data are missing at random or completely at random on the dependent variable, 24 which was indicated in the current study by Little's Missing Completely at Random test (χ2 = 3.93, p = 0.14). Nonetheless, it is important to note the level of missing data across time points to aid with interpretation of conclusions. Of the 115 patients who were eligible for 12-month follow-up, 50 (43%) had data at this time point. Patients with Medicaid insurance were less likely to have 12-month follow-up data compared with those with commercial insurance, but no other demographics or characteristics examined (i.e., disability diagnosis, age, sex, ethnicity, and baseline BMIz) predicted missing data at 12 months.
Results
Approximately two-thirds of the 115 patients were male, with a mean age of 10.46 years. The majority of patients was white (57.4%), had an ASD diagnosis (51.3%), and had Medicaid or used hospital financial assistance to pay for medical services (64.3%). Of those patients with a physical disability, three patients had a diagnosis of cerebral palsy, and one patient had a diagnosis of spinal bifida. Patients' average baseline BMIz was 2.46 (range, 1.65–4.19), corresponding to an average BMI percentile of 98.83%, and an average BMI percent over the 95th percentile of 136.48%. Patients attended an average of 4.27 [standard deviation (SD) = 1.77; range, 2–10] clinic visits by the time of their 12-month follow-up. See Table 1 for complete participant demographics.
Sample Characteristics at Baseline (N = 115)
ASD, autism spectrum disorder; BMIz, Body Mass Index z-scores; SD, standard deviation.
The quadratic time variable was not significant in explaining change in BMIz over the course of treatment, β < 0.001; standard error (SE) <0.001; t = −0.66; and p = 0.51. Therefore, the model examining change in BMIz was reanalyzed with only the linear time variable. Significant reductions in BMIz were observed over the course of treatment for the sample as a whole, β = −0.02; SE = 0.002; t = −9.91; and p < 0.001. The slope for change over the course of treatment (β = −0.02) indicates that, on average, children showed a BMIz reduction of 0.02 per month in treatment controlling for baseline BMIz. These results suggest that the overall trajectory of BMIz over the course of treatment represents a linear decrease.
Regarding patient characteristics that were predictive of a differential trajectory of BMIz over the course of treatment, child age was the only variable that moderated change in BMIz over the course of treatment while controlling for baseline BMIz and other patient characteristics, β = 0.01; SE = 0.003; t = 2.47; and p = 0.014. Therefore, the model examining change in BMIz was reanalyzed with only the main effect and interaction term for child age and BMIz and patient characteristics as covariates (interaction terms for disability diagnosis, sex, ethnicity, and insurance status were removed). Significant linear reductions in BMIz were observed over the course of treatment while controlling for baseline BMIz and patient characteristics, β = −0.01; SE = 0.003; t = −4.50; and p < 0.001. The slope for change over the course of treatment (β = −0.01) indicates that children of the mean age and mean baseline BMIz showed a BMIz reduction of 0.01 per month in treatment. The main effect of child age (z-score) was not significant in explaining change in BMIz across time in treatment β = −0.01; SE = 0.006; t = −1.27; and p = 0.226. However, there was a significant interaction between child age (z-score) and the linear time variable while controlling for patient characteristics, β = 0.01; SE = 0.003; t = 2.14; and p = 0.03. This finding demonstrates that younger children exhibited a greater decrease in BMIz than older children did, and older children actually increased their BMIz, over the course of treatment while controlling for patient characteristics. See Figure 2 for a visual illustration of the moderating effect of child age on BMIz change over the course of treatment.
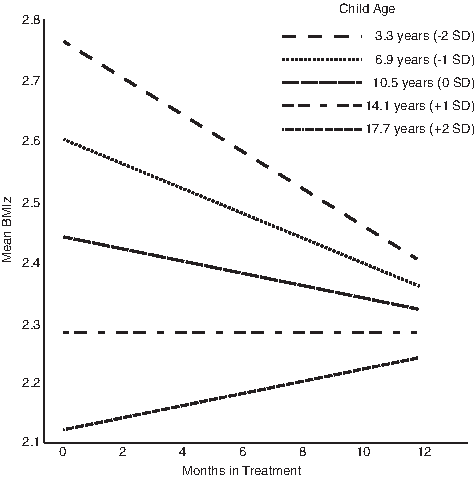
Moderating effect of child age on BMIz change over the course of treatment. BMIz, Body Mass Index z-scores; SD, standard deviation.
Discussion
The present study sought to determine the 12-month outcomes of a multidisciplinary, family-based weight management clinic tailored for youth with disabilities by examining the overall trajectory of BMIz over the course of treatment and identifying patient characteristics that may be predictive of differential trajectories of BMIz change. Our results indicated linear reductions in BMIz over the course of treatment for the sample as a whole while controlling for baseline BMIz. The reductions in BMIz were 0.02 per month in treatment, which amasses to 0.24 over a 12-month period. There is evidence to suggest that this degree of change is likely to have a positive impact on the health status of the child. Indeed, previous researchers25–27 have found metabolic benefits with smaller reductions in BMIz, ranging from 0.13 to 0.18. This finding and supportive literature is promising and provides insight into treatment responses for youth with disabilities who also have obesity.
The only patient characteristic that moderated change in BMIz over the course of treatment while controlling for baseline BMIz was child age, whereby younger children exhibited greater reductions in BMIz over the course of treatment in comparison with their older counterparts. In fact, children with an age 2 SD above the mean actually had a positive rather than a negative slope for their BMIz trajectory. This finding suggests that intervention at younger ages for pediatric weight management produced increased treatment effects, likely related to smaller change in decreased calories and increased activity needed to effect a change in BMIz due to increase in height and smaller size of the child at baseline. Previous research in typically developing youth shows the risk for developing obesity to be highest at younger ages 28 and supports the increased efficacy of early childhood intervention for both the treatment and prevention of pediatric obesity in the typically developing population.29,30 Our finding is consistent with this research and provides additional support that early intervention can substantially improve weight outcomes in youth with disabilities. The finding also suggests the need to identify more intensive supports for older adolescents with obesity.
The patient characteristics of disability diagnosis, sex, ethnicity, and insurance status did not moderate BMIz change over the course of treatment while controlling for baseline BMIz. Of particular interest is the lack of influence of a child's diagnosis on his or her weight change in treatment. This finding suggests that the SNWMC demonstrates equal effectiveness in managing weight and meeting the needs of children with various types of neurodevelopmental disorders by utilizing an adaptive design for each patient. This is promising given that different neurodevelopmental disorders are associated with varied health-related factors, including a combination of dietary and physical challenges, as well as metabolic abnormalities, which play a significant role in overconsumption and weight gain.5,9,13,31 Nonetheless, our findings serve as support for the notion that pediatric weight management programs can be successfully tailored to meet the needs of, and can result in weight loss among, youth with disabilities.
The present study has a few limitations that should be considered when evaluating the results. The attrition rate in this clinical program was high and, thus, even with the safeguards put in place to control for the missing data in statistical analyses, the sample may not be representative of all children with disabilities weight trajectories over time. However, the level of attrition was consistent with other weight management treatment research, 21 and the only difference between patients with and without 12-month follow-up data was insurance status. Anthropometric data were assessed clinically (one measurement each of height and weight) as opposed to the research standard of triplicate. However, the clinical staff received training in obtaining the best possible measurement, and it can be very difficult to obtain measurements in children with disabilities. Our dietitian reviews measurements at each visit and will recommend redoing the measurement if it falls outside a normal variation. The patient population is very heterogeneous in this clinic and reflects a wide range of diagnoses, ages, and severities of illness, and thus may limit conclusions about any particular type of patient population. Furthermore, we did not assess for factors such as ambulatory status or cognitive ability so, while diagnosis did not affect the overall results, it is unknown that for who this clinic approach is best suited in terms of these additional variables. Given that this is a clinical setting and the treatment is adapted to each patient, it is difficult to assess generalizability to other settings. Finally, conclusions about the clinic's efficacy are also limited by the lack of a control group.
This study represents the evaluation of a clinical intervention for children with disabilities and obesity delivered in a clinical setting. The staffing and structure are feasible and sustainable in a clinical setting, the dose is low, and yet, the clinical improvement is significant. We demonstrate significant decreases in BMIz with an average of <5 sessions over a 12-month period. Although adolescents had a statistically significant lower BMIz at baseline, the majority of our patients at all ages presented to the SNWMC in the severe obesity range. Thus, even among a population with more severe obesity, early intervention continues to show increased efficacy as evidenced by the fact that younger children lost more weight over the course of treatment compared with adolescents. We need to continue to develop tailored interventions specific to the needs of families with adolescent children, both with and without disabilities. Finally, future research is needed to investigate additional variables that may impact success in the intervention such as sensory issues, limited food variety, severity of illness, and level of behavioral difficulty. It is imperative that these variables be assessed in a comprehensive and valid manner to adequately capture their constructs. Along similar lines, future research should consider, including other assessment instruments, to measure different clinical outcomes, such as behavioral and/or metabolic assessments.
Footnotes
Acknowledgment
The authors acknowledge funding from the Healthcare Foundation of Greater Kansas City.
Author Disclosure Statement
No competing financial interests exist.