
Abstract
Abstract
Background:
Obesity is a complex disease that involves both environmental and genetic factors in its pathogenesis. Several studies have identified multiple obesity-associated loci in many populations. However, their contribution to obesity in the Vietnamese population is not fully described, especially in children. The study aimed to investigate the association of obesity with Val66Met polymorphism in brain-derived neurotrophic factor (BDNF) gene, delivery method, birth weight, and lifestyle factors in Vietnamese primary school children.
Methods:
A case–control study was conducted on 559 children aged 6–11 years (278 obese cases and 281 normal controls). The obesity of the children was classified using both criteria of International Obesity Task Force (IOTF, 2000) and World Health Organization (WHO, 2007). Lifestyle factors, birth delivery, and birth weight of the children were self-reported by parents. The BDNF genotype was analyzed using the polymerase chain reaction–restriction fragment length polymorphism method. Association was evaluated by multivariate logistic regression and cross-validated by the Bayesian model averaging method.
Results:
The most significantly independent factors for obesity were delivery method (cesarean section vs. vaginal delivery, β = 0.56, p = 0.007), birth weight (>3500 to <4000 g vs. 2500–3500 g, β = 0.52, p = 0.035; ≥4000 g vs. 2500–3500 g, β = 1.06, p = 0.015), night sleep duration (<8 h/day vs. ≥8 h/day, β = 0.99, p < 0.0001), and BDNF Val66Met polymorphism (AA and GG vs. AG, β = 0.38, p = 0.039).
Conclusions:
The study suggested the significant association of delivery method, birth weight, night sleep duration, and BDNF Val66Met polymorphism, with obesity in Vietnamese primary school children.
Introduction
Obesity in children is recognized as a global public health concern. The prevalence of childhood obesity has increased in most parts of the world. 1 In Vietnam, the prevalence of adolescent overweight and obesity in urban districts of Ho Chi Minh City doubled over a period of only 2 years, from 5.6% in 2002 to 13.7% in 2004. 2 In addition, obesity increases the risk of many diseases, including hypertension, type 2 diabetes, cardiovascular diseases, stroke, osteoarthritis, and several types of cancers. 3 Moreover, ∼50% of individuals who are obese in adolescence remain obese in adulthood. 4 Therefore, preventing obesity from early childhood is of great importance in terms of public health to reduce obesity prevalence and related diseases in adults.
Obesity is a complex disease that involves interactions between environmental and genetic factors in its pathogenesis. 5 Sedentary lifestyle and excess food intake are the main environmental factors that lead to obesity. 6 Another important factor is the duration of sleep, which could be a potential contributor to obesity in children.7–9 Both low and high birth weight would likely to lead to higher possibility of obesity.10,11 Studies on twins and nontwin siblings have shown that the genetic components contribute from 40% to 70% of the interindividual variation in common obesity. 12 The variation is reflected in differences of obese prevalence among racial populations and age groups because of differences in environmental factors, risk-factor profiles, and genetic background.6,13 It is necessary to identify the characteristics of genetic and environmental factors, which would increase the risk of obesity among different populations.
Recent advances in genome-wide association studies (GWAS) have evidenced the association of common variants of several genes with the BMI and other measurements of obesity.14,15 Among these genes, the brain-derived neurotrophic factor (BDNF) gene has been considered to confer obesity risk through its effects in the regulation of feeding. Studies in human and rodents have identified the role of BDNF in regulation of feeding and energy balance. Protein BDNF and its receptor (tropomyosin-related kinase B) are highly expressed in hypothalamus and hindbrain—two important energy homeostasis centers of adult animals. 16 The secretion of precursor and mature BDNF proteins is affected by a single-nucleotide polymorphism (SNP) rs6265 (Val66Met, G196A) in the coding region of exon V of the BDNF gene. This SNP resulted in the substitution of valine toward methionine in the 66th position of the amino acid sequence of protein, and the Met variants were found to be significantly responsible for the unusual intracellular packaging of the precursory BDNF, as well as the decline in producing mature BDNF. 17 In addition, several studies have noted a greater connection between BDNF Val66Met polymorphism and BMI not only in adults14,18,19 but also in children.6,13,20–22 However, some studies did not find the association of this SNP with obesity and BMI.23,24 Furthermore, both the A allele20,25 and G allele26,27 were reported to associate with obesity.
Until now, there has been paucity of published data on the association of BDNF gene with obesity among Vietnamese children. Moreover, given the multifactorial pathogenesis of obesity, it is crucial to use an approach to analyze the association of the BDNF gene with obesity, taking into account the influence of lifestyle factors. Therefore, the study aimed to investigate the association between BDNF Val66Met polymorphism and obesity, considering the contribution of delivery method, birth weight, and lifestyle-related factors in primary school children in Vietnam. The most significant independent predictors for obesity were also reported.
Methods
Recruitment of Subjects
A case–control study was conducted with a total of 559 unrelated subjects (278 obese cases and 281 normal controls) recruited from a cross-sectional population-based study. First, 7750 children aged 6–11 years in 31 Hanoi primary school were recruited randomly between October and December 2011 in five urban and three suburban districts of Hanoi. These children were measured anthropometric indices and were then classified into four groups, including underweight-, normal weight-, overweight-, and obese group. For genetic analysis, 2 mL of venous blood was collected from 321 normal children and 366 obese children. Written consent to participate in the study was given by the parents of all subjects. The Ethics Committee of the National Institute of Nutrition approved this study. Next, a self-report questionnaire was completed by parents to collect data on birth delivery, birth weight, and lifestyle factors of the children. Out of the 687 blood-donated children, only 559 subjects with complete data of lifestyle were used for analysis.
Measurements
Anthropometric indices, including weight, height, waist circumference (WC), and hip circumference (HC), were measured twice for each individual, and the mean was used for the purpose of analysis. Body weight and height were measured with subjects in light clothing and without shoes. BMI was calculated as the weight per square of the height (kg/m2). WC was measured midway between the lower rib margin and the iliac crest, while HC was measured at the broadest circumference below the waist. Waist–hip ratio (WHR) was calculated as the WC (cm) divided by the HC (cm).
Obesity children and normal-weight children were classified using the criteria of age- and sex-specific BMI cutoff points proposed by the International Obesity Task Force (IOTF, 2000). Children who were classified underweight or stunting or wasting by the criteria of World Health Organization (WHO, 2007) were excluded from the study. None of the recruited obese children had any medical causes of obesity, including disorders (Hypothyroidism and Cushing syndrome) or drugs (steroids, antidepressants, antipsychotics, and seizure medications).
Genotyping Method
Genomic DNA was extracted from peripheral blood leukocytes by using the Wizard® Genomic DNA Purification Kit (Promega Corporation, Madison, Wisconsin). Genotyping of BDNF Val66Met was carried out by using the polymerase chain reaction–restriction fragment length polymorphism (PCR-RFLP) method. The following primers were used: forward primer 5′-ccaggtgagaagagtgatg-3′ and reverse primer 5′-agtctgcgtccttattgtt-3′. A 15 μL PCR reaction was performed according to the following conditions: 94°C for 3 minutes and 35 cycles of denaturation at 94°C for 30 seconds, primer annealing at 56°C for 40 seconds, primer extension at 72°C for 30 seconds, and final extension at 72°C for 8 minutes. PCR products (281 bp) were detected on Redsafe-stained 2.5% agarose gel. Five microliters PCR products were digested with 0.5 μL FastDigest Eco72I (PmlI) restriction enzyme. Alleles were visualized as fragments by electrophoresis through a Redsafe-stained 2.5% agarose gel. Distribution patterns of the BDNF-rs6265 polymorphisms were AA (281 bp band), AG (three bands: 281, 211, and 70 bp), and GG (two bands: 211 and 70 bp).
Statistical Analysis
Categorical variables were represented as percentages and were tested by the χ2 test to compare their distribution between cases and controls. Quantitative variables were checked for normal distribution and compared to identify the difference between cases and controls, using either independent-sample t-test or Mann–Whitney U test, when appropriate. The Hardy–Weinberg equilibrium (HWE) was assessed using the χ2 test. Binary logistic regression analysis was used to test several models for the associations of obesity to the BDNF Val66Met risk allele and other variables, taking into account the covariates (age, sex, birth weight, living region, and lifestyle-related factors). The variables included in the analyses were checked for multicollinearity to ensure the stability of the parameter estimates. In this study, data are presented as odds ratios with 95% confidence intervals (CI). The Akaike information criterion (AIC) was used to assess model fit for a given set of data; lower values indicated improved model fit. To assess the model performance, a receiver operating characteristic (ROC) curve was built to plot probabilities resulted from the multivariate logistic regression analysis, and the area under curve (AUC) was used to measure the power to predict individuals with obesity. The above statistical procedures were performed using SPSS version 16.0 (SPSS, Chicago, Illinois). The Bayesian model averaging method was used to cross-validate the final model using Bayesian Model Averaging Software with the R Statistical Environment version 3.1.3. 28
Results
The characteristics of subjects in cases and controls are shown in Table 1. There were significant differences between obesity and control groups with regard to living region, birth weight, height, weight, BMI, WC, HC, and WHR. Supplementary Table S1 (Supplementary Data are available online at www.liebertpub.com/chi) shows that the frequencies of the AA, AG, and GG genotypes differed significantly between case and control groups (p = 0.03). The G allele frequency was 0.42 in the controls and 0.46 in the cases. The observed genotype frequencies in the control group were in HWE (p = 0.893), but not in the obese group (p = 0.001). The analysis of the best-fit model for the BDNF Val66Met polymorphism with obesity among genetic modes of inheritance (additive, codominant, dominant, overdominant, and recessive) showed that the lowest AIC values was found in the overdominant mode, indicating that it is the best-fit model in the data (Supplementary Table S2). This mode was used to further multivariate analyses.
Characteristics of Participants in Control and Obese Groups
Data are the mean ± SD unless otherwise indicated.
p-value by Student's t-test or Mann–Whitney U test or chi-square test.
Data are median (interquartile range).
Data are geometric mean (95CI).
HC, hip circumference; WC, waist circumference; WHR, waist–hip ratio.
Univariate and multivariate logistic regression analyses of potential associated factors for obesity are presented in Table 2. The results showed that delivery method, birth weight, living region, night sleep duration, and BDNF Val66Met polymorphism were significantly associated with children obesity in univariate analysis. The association remained significant in the model after adjustments for sex, age, residence, time spent for television and computer games, school travel mode, and sport participation. The variables including delivery method, birth weight, living region, night sleep duration, and BDNF Val66Met polymorphism were also confirmed using the Bayesian model averaging, in which they were selected in almost models (Fig. 1). Table 3 shows the most significant independent predictors for obesity in final prediction model. The area under ROC curve was 0.657 (95%CI: 0.610–0.704, p < 0.0001) (Fig. 2) for the model of obesity on the predictors, including delivery method, birth weight, living region, and night sleep duration. Adding the genetic marker to these covariates improved the area under ROC curve slightly from 0.657 to 0.668 (p = 0.001, Wilcoxon Signed-Ranks Test).
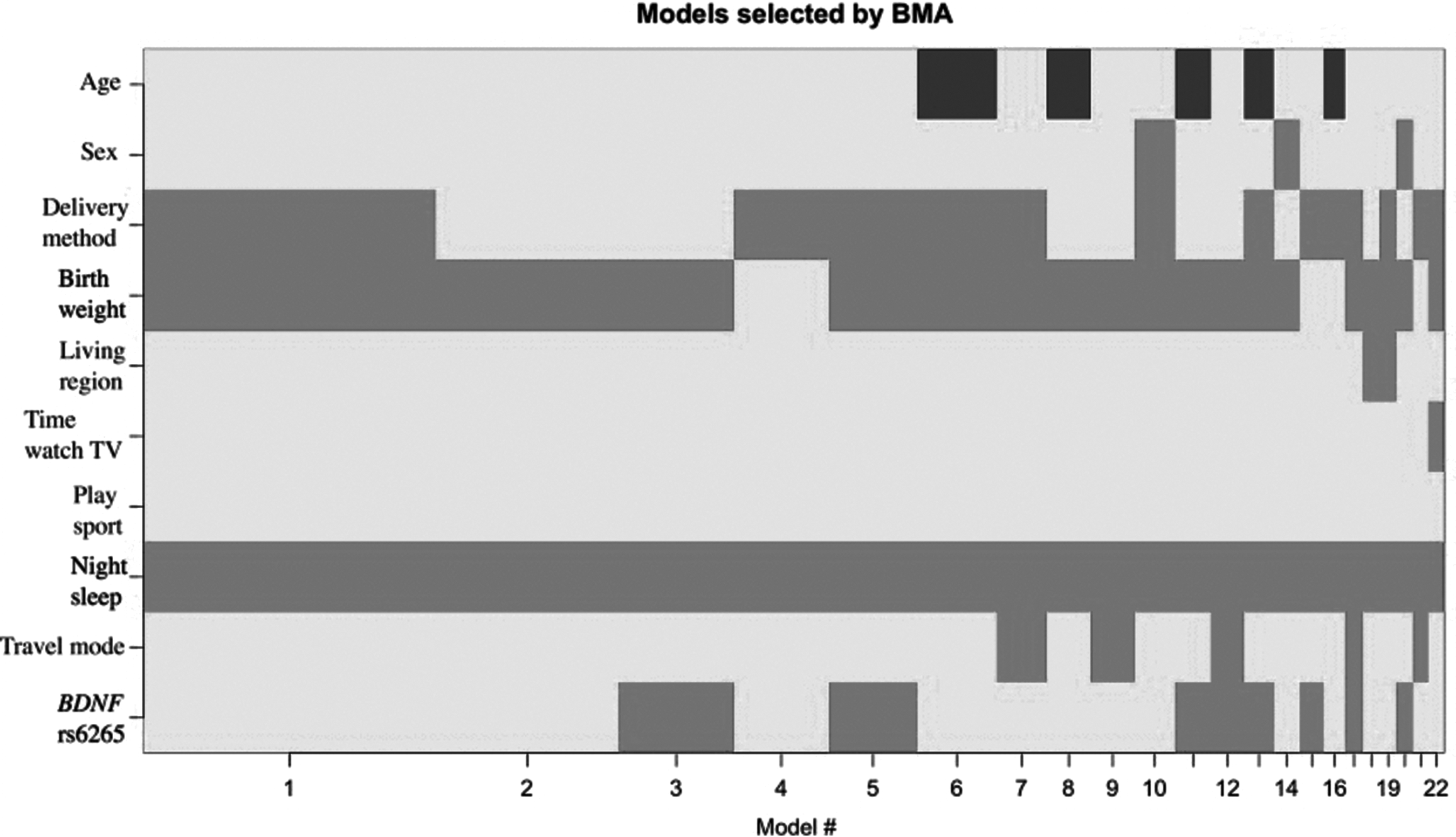
Analysis BMA analysis to cross-validate the final model. The above figure shows the finding of the BMA analysis to cross-validate the final model found by multivariate logistic regression analysis. There were 22 models selected by BMA, in which delivery method, birth weight, living region, night sleep duration, and BDNF Val66Met polymorphism were presented in most of the selected models. BDNF, brain-derived neurotrophic factor; BMA, Bayesian Model Averaging.
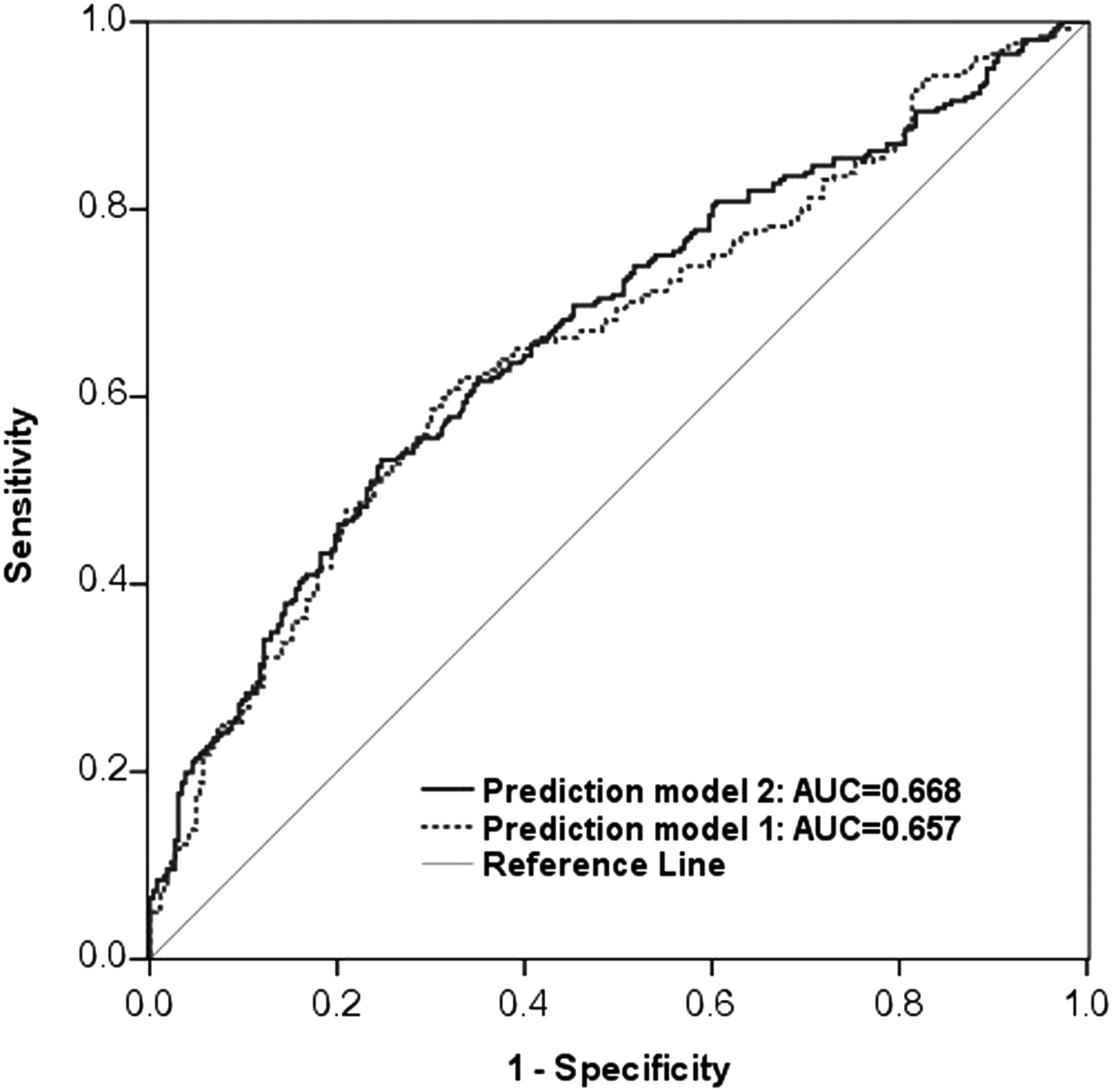
ROC curves for obesity prediction on the BDNF Val66Met polymorphism, delivery method, birth weight, living region, and night sleep duration in Model 2 and Model 1 without genetic marker. Predictors were adjusted for age and sex. AUC, area under the curve; ROC, receiver operating characteristic.
Associated Factors of Obesity in Primary School Children
BDNF, brain-derived neurotrophic factor: CI, confidence intervals; OR, odds ratio.
The Most Significant Independent Predictors for Obesity in Vietnamese Children in Primary Schools
β and p-values were calculated by multivariate logistic regression adjusted for sex and age.
Discussion
To the best of our knowledge, this is the initial report on the significant association of BDNF Val66Met polymorphism, delivery method, birth weight, and night sleep duration with obesity among primary school children in Vietnam. Other factors, such as living region, time spent for watching TV and playing computer games, participation in sports, and school travel modes, were not significantly related to obesity in the cohort.
The relationship between delivery method and obesity has been reported in many studies. In the United Kingdom, children born by cesarean section involved harvesting fat tissue increases from 6 weeks after birth, at the age of 11 they had a 1.83-times higher risk of overweight and obesity than those born by vaginal delivery. 29 The association between cesarean section and childhood obesity was reported in Europe 30 and Brazil 31 ; while no association was found in Canada 32 and Hong Kong. 33 An association between cesarean delivery with obesity was observed in children at 2 years, but not in those aged from 6 to 10 years. 34 In a recent systematic review and meta-analysis, including 28 studies, 35 children born by cesarean section were at higher risk of developing obesity in childhood. In the present study, the children born by cesarean delivery were 1.6 times more likely to have obesity than those born by vaginal delivery. The difference of the associations can be explained by the fact that the cesarean section is often done for children with high birth weight, 36 early gestational age, or higher age mothers. 33 Moreover, recent studies on microbiome may also explain why cesarean section born children are more likely to be obese compared with vaginal born children. 37 The vaginal born infants carried gut microbiome similar to that of mother, whereas the cesarean born babies lacked this similarity of gut microbiome. 38 Individuals born by cesarean delivery were 15% more likely to become obese during follow-up than those born by vaginal delivery; those born via cesarean delivery had 64% higher odds of obesity compared with their siblings born via vaginal delivery. 39
The present data showed that primary school children with birth weight of 3500–4000 g and over 4000 g had higher risk of obesity odds ratio (OR = 1.8 and 2.86, respectively) than those with birth weight of 2500–3500 g. Epidemiological studies have demonstrated that both low and high birth weight have increased obesity in later life because the utero environment may influence the fetus's epigenetic process.40,41 However, how the four epigenetic modalities—DNA methylation, noncoding RNA, transcription factors, and histone modifications—contribute to epigenetic memory and how epigenomic changes may mediate the altered control of fetal gene expression as a consequence of maternal obesity are not well characterized. 42
Experimental studies in humans have found that a short period of sleep duration could result in important changes in the secretion of cortisol and the growth hormone, 43 as well as levels of leptin and ghrelin, which are related to the regulation of hunger and satiety. 44 Several cross-sectional studies discovered positive association between short sleep duration and obesity,9,45 while some did not find the similarity results. 46 In this study, children who slept fewer hours (<8 h/night) had much higher risk of obesity (OR = 2.56). It could be suggested that parents should be well aware of their child's night sleep duration to prevent children from becoming obese from an early age.
Studies on the relationship between BDNF Val66Met variants and obesity reported that both the A allele20,25 and G allele26,27 were associated with obesity. Several reports found the relationship between this SNP and obesity in childhood Asians22,47 and Caucasians.20,48 Meanwhile, other research efforts indicated a lack of association between the SNP and obesity traits in Spanish school children 49 and in young German participants. 50 The varied results may be explained, in part, by differences in environmental factors, risk-factor profiles, and genetic backgrounds of those populations. 6 Reports of GWAS 18 and meta-analysis 19 indicated that G allele of BDNF rs6265 polymorphism was significantly associated with obesity. In this study, according to the model of overdominant genetic, the heterozygous genotype AG increased the risk of obesity by 1.49 times compared with the other two genotypes (95% CI = 1.02–2.17). Compared with AA homozygotes, subjects with G allele (AG or GG) had an increased odds of obesity [OR (95%CI) = 1.58 (1.09–2.29) in the codominant model]. However, GG homozygotes in the dominant and copy number of G allele in the additive model were not significantly associated with obesity. This is likely due to the small sample size of the study.
In association studies, the p-value correction of multiple hypotheses testing is necessary, especially for studies with a large number of SNP such as GWAs. Actually, we have only checked one hypothesis on the relationship between BDNF Val66Met polymorphism and obesity in the present study, considering the contribution of delivery method, birth weight, and lifestyle-related factors. Therefore, the correction for multiple testing was not been applied in the study. The multivariate logistic regression analysis indicated that the association reported was not changed by covariates. In addition, the independent variables in the final model were cross-validated by the Bayesian model averaging method.
Major factors which affect the genetic equilibrium are as follows: mutations, recombinations during sexual reproduction, genetic drift, gene migration, and natural selection. In the present study, given that obese and normal subjects were recruited randomly in a large population of 7750 children aged 6–11 years in 31 Hanoi primary schools in five urban and three suburban districts of Hanoi City, the disturbance of HWE in the obese group could be partly explained by natural selection, but not the others. Obese children were a specific group who may have higher frequency of risk alleles susceptible to obesity. For instance, the observed frequency (24.1%) of AA genotype of the BDNF Val66Met polymorphism in our cohort was significantly lower than expected frequency (28.9%) estimated by Hardy–Weinberg principle.
In addition to genetic factors, a variety of studies have provided strong evidence demonstrating that sedentary behavior was positively related to obesity among children.51–53 Hence, reducing television viewing time and increasing outdoor activities are effective strategies for managing the obesity epidemic in children.7,54 In addition, walking and cycling to school are regarded as valuable opportunities for children to accumulate physical activity 42 and maintain a healthy weight.56,57 In this study, children's total time consumption for watching television and playing computer games per day was classified into three different categories (<2, ≥2–3, and >3 hours) as recommended by the American Academy of Pediatrics, children should only spend a maximum of 2 h/day for watching television and playing video/computer games. 58 The present results showed that the total time spent on television and computer games, sport participation, and active transport were not significantly associated to children obesity in Vietnam.
The present findings must be interpreted in the context of several limitations. First, the case–control design did not allow a causal conclusion. Second, given the relatively small sample size, the association of obesity with sedentary behaviors, including total time spent on television and computer games, sport participation, and school travel modes, was found to be not statistically significant in the cohort; and it should be further evaluated in prospective study with larger sample. Third, the lifestyle factors of the children who were self-reported by parents could be recorded incompletely. Next, we were unable to collect information regarding the food intake and physical activity levels of the participants, so the relationship between those two factors toward obesity could not be evaluated in the study. Finally, genetic factor was only the BDNF Val66Met polymorphism. Although it was significantly associated with childhood obesity in the cohort, adding the genetic marker in clinical covariates improved the area under ROC curve slightly.
Conclusions
This study showed the significant association of BDNF Val66Met polymorphism, delivery method, birth weight, and sleep duration with the risk of obesity in primary school children in Vietnam. It is necessary to extend the scale of the research and collect more information on both genetic and environmental factors to identify the gene–environment interactions to childhood obesity in Vietnam.
Footnotes
Acknowledgments
We thank colleagues in Hanoi National University of Education and National Institute of Nutrition for their kindly help and support. This study was supported by the Grant No. DHSP2015-422 from Hanoi National University of Education, the Grant No. B2014-17-47 from the Ministry of Education and Training, and the Grant No. 01C-08/05-2011-2 from Hanoi Department of Science and Technology, Vietnam.
Author Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.