
Abstract
Abstract
Background:
Sedentary lifestyle is growing among children and adolescents that may contribute to problems such as overweight and obesity. Consequently, interventions to improve weight loss in this population are necessary. The aim of this current review was to evaluate the effectiveness of game-based interventions to reduce body mass index (BMI) among children who were overweight or obese.
Methods:
All randomized controlled trials with a game-based approach for lowering weight in obese/overweight youths aged 5–18 years old were identified from January 2005 to June 2017 across PubMed, Web of Science, Embase, Scopus, and ScienceDirect. Two independent reviewers completed data extraction sheets on information such as sample size, country of origin, age of participants, type of interventions, and BMI change from pre- to posttest. A consensus on collected data was obtained, and a final list of studies meeting inclusion and exclusion criteria was arrived at. Data were analyzed using Comprehensive Meta-analysis software, and effect size was measured by standardized mean difference (SMD) and Hedges' g measure. Heterogeneity and publication bias were also examined using I2 index and funnel plot.
Results:
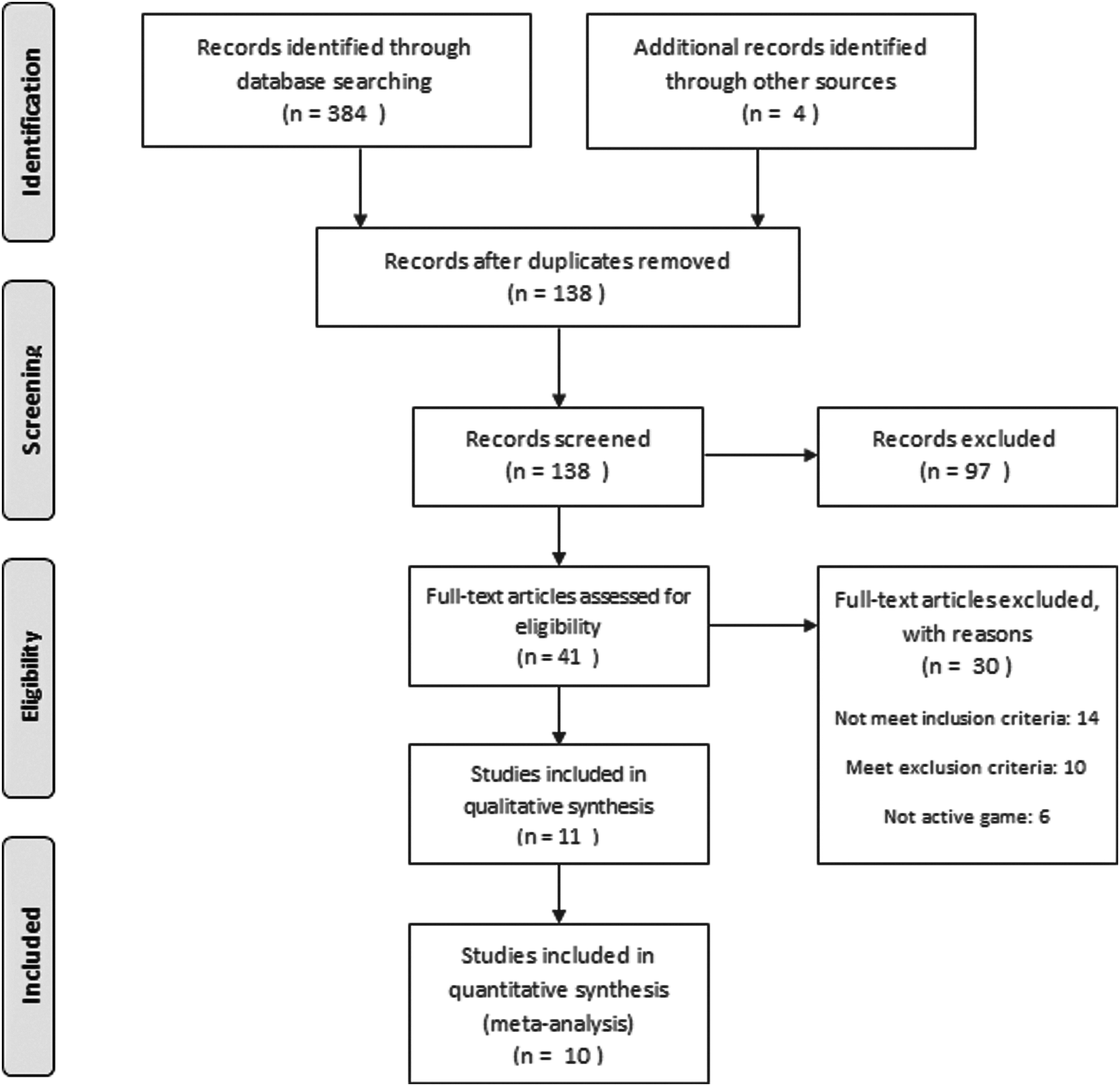
A total of 388 articles were identified from electronic and manuals' searches. After deletion of duplicated articles, 138 articles remained that were then screened in terms of relevance. Of those, 41 articles were examined to determine eligibility. Finally, 10 articles met inclusion/exclusion criteria and were entered into the quantitative meta-analysis. Results indicated a small but significant effect size in terms of BMI reduction [SMD, −0.234; standard error (SE), 0.069] among included studies. The average BMI z-score reduction was −0.181 (SE, 0.071). Trials which used other types of interventions along with active game-based approaches achieved greater effect sizes than single game-based interventions. There was a significant difference between studies based on their country of origin, BMI value, and intervention type. Those conducted in United States, those including participants with BMI ≥30, and studies with multicomponent intervention reported a higher reduction of BMI than others. However, no significant difference in BMI was found in terms of variables such as age, sample size, type of participant (overweight/obese), intervention duration, or participant gender. No publication bias was identified, and studies were homogenous (I2 = 22.5%).
Conclusions:
Interventions that involve active gaming may produce small effects in terms of improving BMI among children who are overweight/obese. Therefore, we recommend that supplemental interventions be used to enhance the effectiveness of game-based interventions.
Introduction
The problem of overweight and obesity (OO) has spread worldwide among children and youths. According to global estimates presented by World Health Organization, more than 41 million children between ages 0 and 5 years old were obese in 2014, and nearly 20% of school aged children were either overweight or obese.1,2 Both developed regions of the world and developing countries experience this problem. For example, in the United States nearly one third of adolescents are either overweight or obese. 3 There is a broad range of OO among Asian countries as well, from 5% (in China) to 36% (in Bahrain). 4 In Iran among those under 18 years old, OO was estimated at between 3.2% and 13.5%. 5
According to current definitions, having a body mass index (BMI) between the 85th and 95th percentile of the same age and sex of children and teens is recognized as being overweight; those who are at the 95th percentile or higher of the BMI are labeled as obese. 6 Sedentary behaviors such as watching TV and playing computer or video games without active movement contribute to the development of OO in children.7,8 Such behaviors often continue in adulthood and ultimately result in threatening health issues, including cardiovascular diseases, diabetes, osteoarthritis, and hypertension. 9 Unfortunately, changes in lifestyle especially in urban areas toward decreasing physical activity (PA) and consuming unhealthy foods with high amounts of fat and sugar exacerbate this condition, increasing the urgency to develop interventions that may reduce these poor health behaviors.
Encouraging health lifestyles using effective interventions is the heart of health education and promotion programs, and there are many such programs that target high risk children and youth.10,11 Since children prefer to engage in enjoyable and entertaining activities, using these types of interventions may provide a golden opportunity to practice health education and promotion. In other words, health education may be integrated into game-based activities to improve healthy lifestyles. 12 Health education and promotion programs include programs that seek to change behavior toward a healthier lifestyle. Therefore, even those programs that may not clearly contain an educational component will implicitly include learning experiences. In other words, encouraging involvement in a fitness program involves learning new behaviors which can replace unhealthy ones. This is the definition of a health promotion program used in this article.
Promoting PA using active games is an important strategy among youth because they are often willing to reserve considerable time for game playing. 13 Active game-based interventions are a new approach to PA that has many benefits in terms of increasing exercise and sport-like activities and may have different types, including active video games or exergaming to exercise using competitive games.12,14
Several studies have evaluated the impact of active gaming and game-based programs to increase PA and reduce sedentary screen time in children and youth.13,15,16 There is also evidence on increasing energy expenditure and improving anthropometric/physiologic parameters among children involved in active gaming.17,18 Similarly, a number of systemic reviews have assessed the role of active gaming to change lifestyle in youth. For example, playing certain video games may increase light- to-moderate intensity PA, 19 but the authors did not recommend using these games to increase PA in children because the mechanism by which it reduces sedentary behaviors is not entirely clear. In a review, playing video games was recognized as an effective way to increase heart rate and moderate PA among children, although they acknowledged that there is not sufficient evidence yet that indicates long-term efficacy of such activities. 18
In another review, playing video games alone was insufficient to enhance PA when in a home setting. 20 In a review of studies examining the role of active video gaming to promote PA, investigators identified 13 intervention studies, of which only 3 reported that the intervention effectively increased PA. 21 However, in a systematic review of video game interventions to combat obesity, Guy et al. 22 concluded that video games—despite their widespread reputation of increasing obesity—may be used to help overcome OO by increasing PA and knowledge about nutrition. Similarly, DeSmet et al. 23 emphasized the effectiveness of serious digital games either as a standalone or as a component of a multidimensional program to increase knowledge and encourage behaviors that might lead to a healthy lifestyle. Given the heterogeneous nature of these games, further exploration to identify the benefits of specific games was recommended. 23
An analysis of the abovementioned reviews reveals that there is no consensus on the effectiveness of game-based interventions in reducing obesity or impacting its determinants such as PA or diet. In addition, the type of intervention, sample size and characteristics, and geographical location of the interventions have received little attention in prior reviews. Systematic reviews that have attempted to assess the benefits of active game playing on health have mostly focused on measures such as PA diary or self-reported screen time that are not considered robust and objective outcomes or have only considered one specific type of active game like exergaming. Furthermore, the target populations of such studies were primarily healthy boys and girls with only limited emphasis on those with OO.
Among the few reviews that specifically addressed obese or overweight children, the findings were presented in a descriptive manner without statistical examination of effect sizes. Therefore, because game-based intervention reviews have not yet examined a measurable outcome like BMI in youth with OO (at higher risk than healthy youth) and there is no comprehensive evidence regarding the role of adjunctive factors (intervention type, sample characteristics, etc.), we decided to conduct a systematic review to fill these research gaps. Two primary research questions were addressed in this review as follows: (1) How effective are game-based interventions in reducing BMI among participants? and (2) What are the active ingredients (e.g., age, sample size, type of intervention, location, BMI category, intervention duration, and participant gender) to such interventions?
Methods
Search Strategy
A systematic search was conducted from January 2005 to June 2017 using PubMed, Web of Science, Embase, Scopus, and ScienceDirect. We also manually assessed the reference lists obtained from studies identified using electronic sources. Used in the search were keywords such as game, play, active game, exergaming, active video game, exertainment, intervention, program, health education, children, adolescents, students, school age, obesity, overweight, obese, BMI, body composition, randomized controlled trial (RCT), and RCT for the title, keyword, and abstract sections of articles.
Boolean operators (and, or, not) were used to execute a purposeful search and to combine the keywords. For example, in advanced search of PubMed, we considered the following combination of the keywords for a single search: “Game [Title/abstract] AND program [Title/abstract] AND Children OR adolescents [Title/abstract].” When a search did not include any results or of only limited findings, we reduced or changed the search terms and replicated our search with fewer or different keywords. We also attempted to try different combinations of main keywords in every database.
Selection Process
All articles were retrieved that examined an active game to reduce weight or increase activity in overweight/obese children or adolescents (age range 5–18 years) that measured BMI and was designed as an RCT. Only interventions that used active gaming alone or combined with other types of interventions such as nutrition counseling or health education were included in this review. When a study was conducted on both normal and obese children or on those beyond the age range of 5–18 years old, only subgroups that were consistent with inclusion criteria were included (where they could be distinguished from others), otherwise the study was excluded. Normal weight children/adolescents or those outside the defined age range were not included in the review. Articles written in English with full text available were selected. Intervention studies involving subjects with normal weight or those with other comorbidities such as diabetes were excluded. No reviews or qualitative research was included, although reviews were searched to find additional studies. Inclusion and exclusion criteria were established before the review based on initial assessments of similar reviews.
Screening for study selection was conducted in two phases. First, the title and abstract of the articles were screened to identify relevant articles and then the full texts were retrieved and examined for eligibility criteria. The selection process is described using PRISMA flow diagram (Fig. 1) with the primary outcome being BMI. The BMI may be calculated in three different ways as follows: metric BMI (kg/m2), BMI z-score, and BMI percentile. While metric BMI can be used for all ages and is especially recommended for adults, two other ways of calculating BMI (adjusting for age and sex) have been suggested for children and adolescents. BMI z-score and percentile more accurately identify adiposity and excess fat in young children because they are compared to standard references for age and sex. 24 For the purpose of current study, metric BMI, as well as BMI z-score (only for studies that reported this measure), was examined. These outcomes were chosen because many interventions on obesity report them as primary outcome measures. In the present review only 6 of 11 studies reported z-scores as an outcome, while 10 of 11 studies reported metric BMI. In addition, only three studies reported BMI percentile change. Therefore, we used the first two parameters (BMI and BMI z-score) in this meta-analysis.
Data Extraction
A data extraction sheet was developed with following information: authors and year, title, country of origin, sample size, age, BMI, inclusion and exclusion criteria, summary of intervention, duration of study, setting of data collection, number (percent) of obese participants, gender, findings, and design of study. Two investigators (A.A. and H.S.) using the same extraction form collected this information, and any discrepancy was resolved by discussion after review of the full text and consultation with a third investigator (M.S.). To assess the quality of included studies we used criteria described by Jadad et al., 25 as well as the latest guideline from the Cochran handbook for systematic reviews of intervention studies. 26 These criteria included examination of bias risk in selected studies as follows: randomization, allocation concealment, blinding, reasonable dropout or withdrawal rates, nonselective reporting of outcomes, and sufficient data reporting.
We considered one score for every criteria and classified studies into four levels in terms of quality: high (score 5–6; grade A), moderate (score 4–5; grade B), fair (score 2–3; grade C), and low (score <2; grade D). Only studies with grade C or higher could have been included in our final evaluation (Table 1). For criteria that were not reported in the article or for those that were unclear, we contacted the authors through e-mail to obtain this information.
Methodological Quality of Studies Included in the Systematic Review
 , 1 score;
, 1 score;  , 0 score.
, 0 score.
Data Analysis
The Comprehensive Meta-Analysis software (CMA) version 2.0 for Windows was used to analyze the data. The unit of the analysis was any publication that met our inclusion/exclusion criteria. We used two types of effect sizes as follows: the standardized mean difference (SMD) and Hedges' g for overall and subgroup analyses. The preferred index for assessing effect sizes for RCTs is the SMD. However, Hedges' g uses a simple correction for variance that may address the overestimation of variance that occurs with small samples. 27 Generally, the effect size is classified as small (<0.5), medium (0.5–0.8), and large (>0.8). To assess heterogeneity of included studies the measure of I2 is useful. When this measure is higher than 50% there is a notable heterogeneity between studies, and random effect models provide more accurate results. However, for studies that are homogenous, fixed effect models are recommended. Another measure used to identify heterogeneity is the chi-square test, where a significant p-value (p < 0.05) also indicates heterogeneity. 28 Subgroup analyses based on important characteristics of the studies were conducted to identify factors that could impact outcome. The z-test based on mean difference in effect sizes was used to compare study subgroups. A 95% confidence interval and α <0.05 were set to indicate significance.
Assessment of Publication Bias
A funnel plot was used to examine publication bias. This visual tool provides a scatter plot of treatment effects based on heterogeneity. The vertical axis of this plot indicates study precision and standard error (SE) of the effect. When the distribution of studies in the funnel plot is symmetrical and the data set is appropriate, there is no publication bias. In this plot, the most powerful studies place near the top. Two statistical tests that may be used to assess heterogeneity in a funnel pot are the Begg and Mazumdar's test to examine interdependence of variance and effect size and Egger's test to indicate asymmetry of the funnel plot. Significant results from either of these tests (p < 0.05) suggest publication bias. 29
Results
A total of 384 articles were retrieved from databases: PubMed (n = 96), Web of Science (n = 72), Embase (n = 83), Scopus (n = 78), and ScienceDirect (n = 55). From examining citations of articles retrieved, we identified four extra articles that were not uncovered during the electronic search. After removing duplicates, the number of studies was reduced to 138 articles. Articles that described the effects of screen time only, those that examined exercise activities without a gaming approach, and those that did not focus on obese or overweight children were excluded. This reduced the number to 41 full text articles, and of these, only 11 articles met the inclusion/exclusion criteria.30–40 After 1 article was dropped because it reported only BMI z-score as the outcome, 36 this left 10 articles that could be used in the meta-analysis (Fig. 1). However, this study was included in the meta-analysis that examined BMI z-score as the primary outcome.
All studies included in the review found that game-based interventions had a positive impact on reducing weight and BMI among participants. However, several studies demonstrated no significant difference between intervention and control groups in terms of BMI reduction. Most studies were conducted in the United States (6/11), and 7 studies had sample sizes of <100. The pooled mean age of participants in all reported studies was 11.7 [standard deviation (SD) = 1.37] and 58% of them were girls. Five studies did not report the number of obese subjects, but among other six studies 95.7% were obese. The pooled mean duration of the intervention was 4.8 (SD = 2.9) months, and majority (63%) used some types of exergaming for the intervention. Details of study characteristics are found in Table 2.
Characteristics of Studies
For follow-ups more than once, the last follow-up has been reported.
For this study BMI z-score has been reported.
SD, standard deviation.
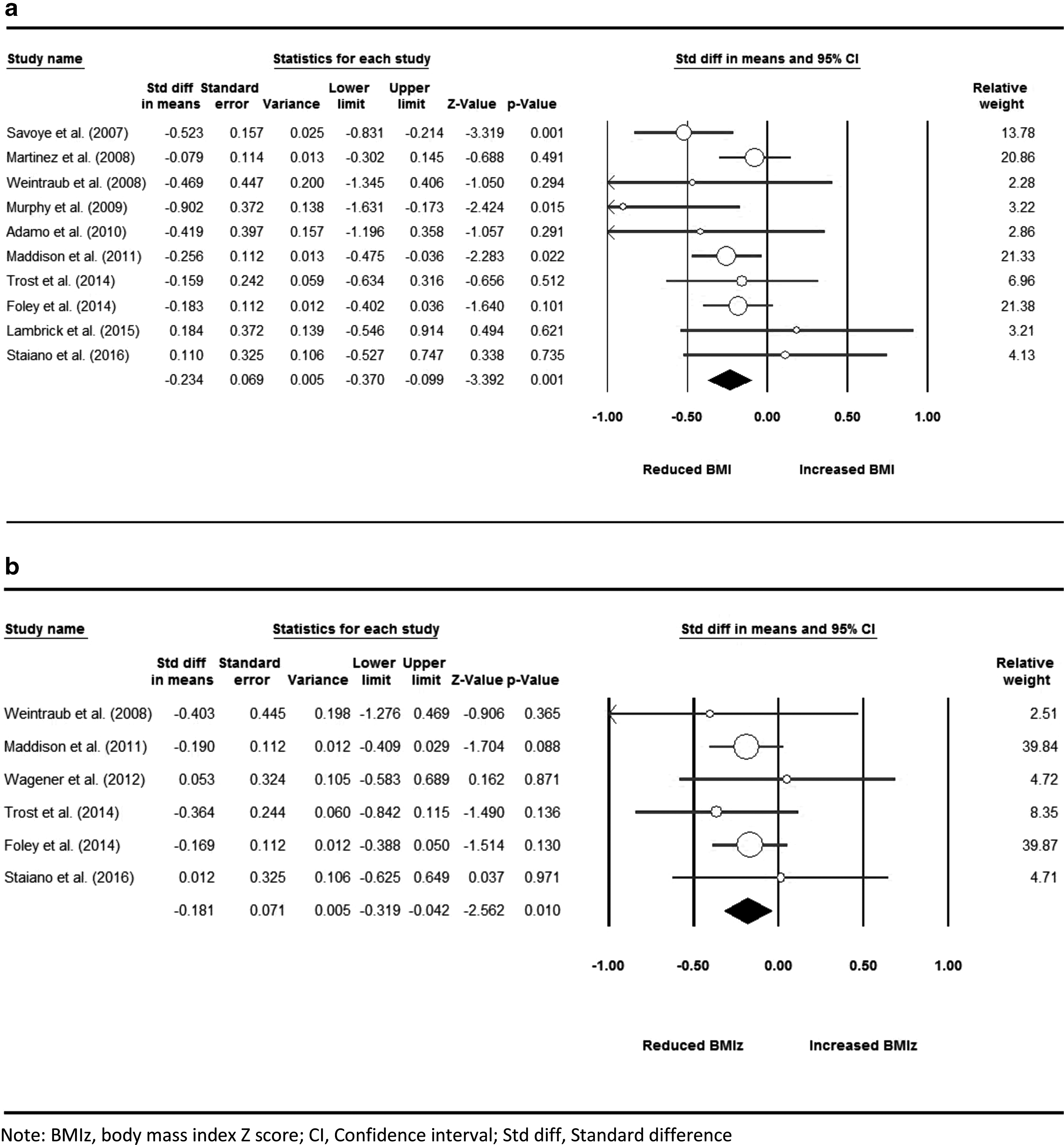
The results of the meta-analysis using BMI mean score and z-score are presented in the Figure 2. Overall, the SMD was −0.234 (SE = 0.069), and articles using BMI z-scores had a SMD slightly lower (−0.181, SE = 0.071). In the meta-analysis examining mean BMI change, only three articles indicated a significant BMI reduction between groups, and in the second analysis that examined BMI z-scores, no studies reported a significant reduction compared to the control group. However, both meta-analyses when examining pooled results demonstrated a significant reduction with the intervention (p < 0.05).
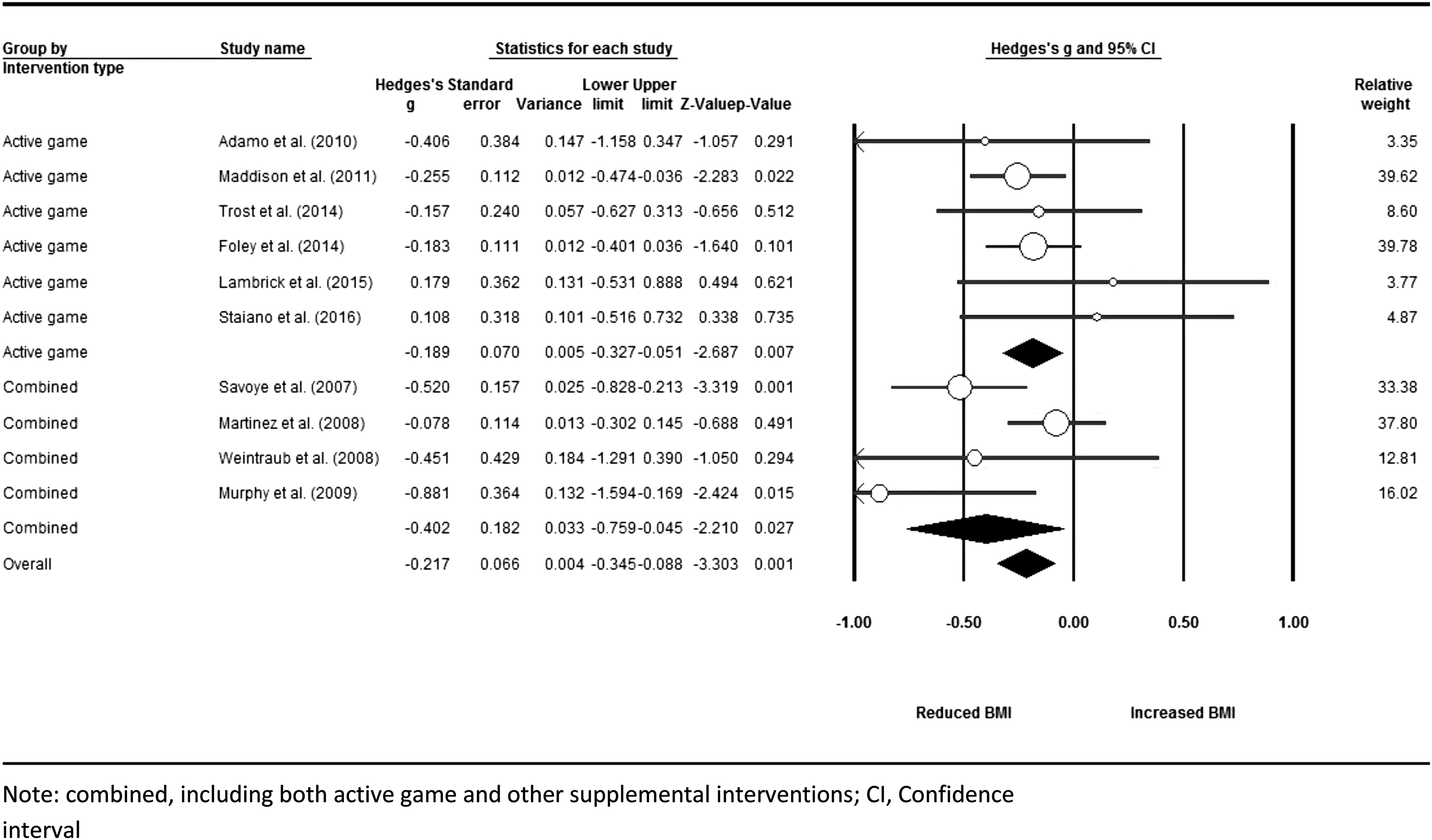
Grouping studies by intervention type (Fig. 3), a combined approach (active gaming along with other interventions), had a greater effect on BMI reduction (Hedges' g = −402, SE = 0.182, compared to g = −189, SE = 0.070, for intervention involving active gaming alone). There were significant differences between studies conducted in the United States compared to those conducted in other countries and between studies on participants with BMI <30 compared to those with BMI ≥30. Those studies conducted in the United States, as well as those conducted on samples with BMI ≥30, reported greater effect sizes than other studies (p < 0.05). However, there was no significant difference between subgroups in terms of age, sample size, condition of the participants (overweight/obese vs. obese), intervention duration, or gender (Table 3).
Subgroup Analyses Based on Study Characteristics
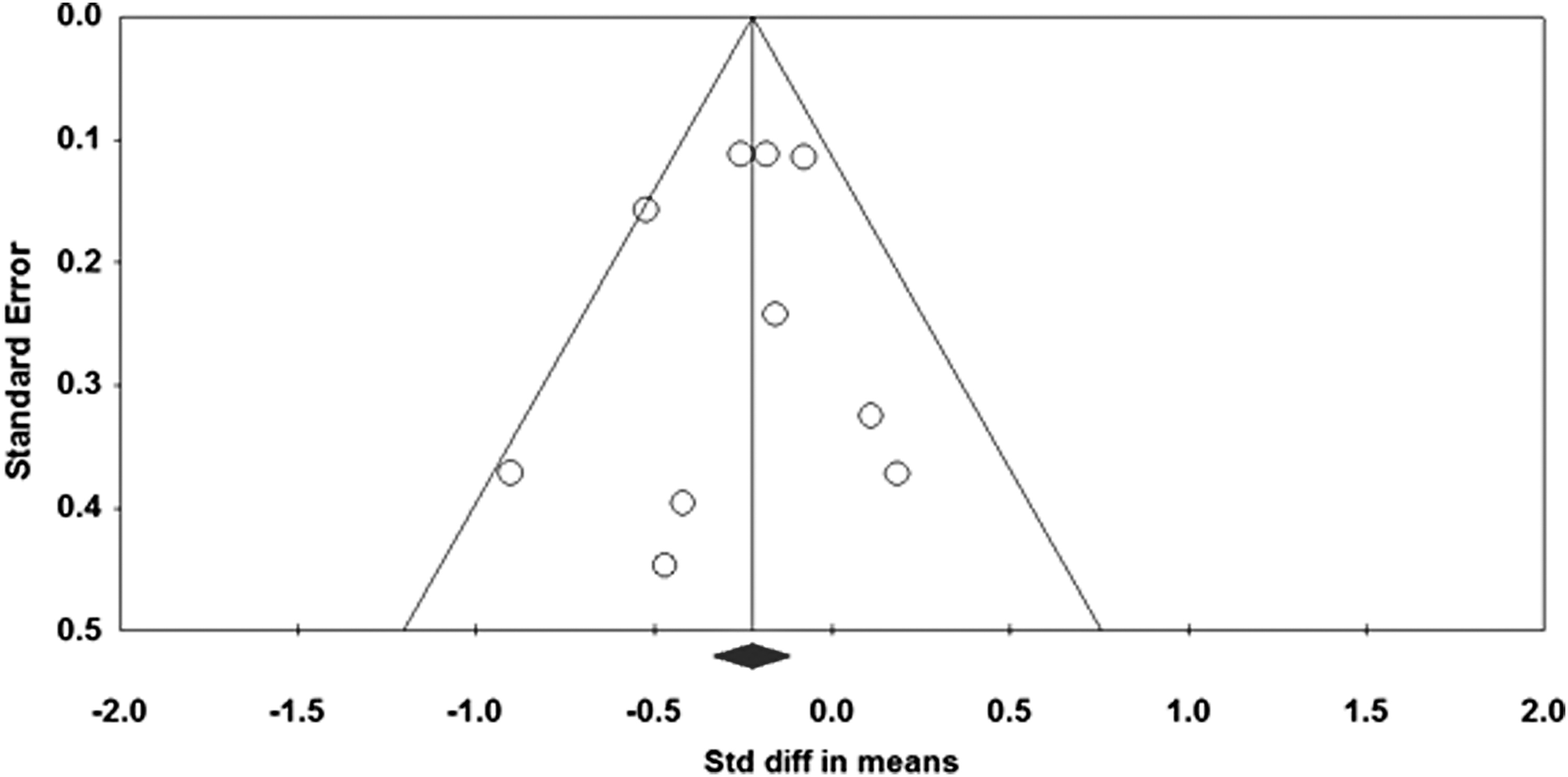
The funnel plot (Fig. 4) revealed a relatively symmetric diagram without considerable heterogeneity. Kendall's τ value (Begg and Mazumdar rank correlation test) was not significant (z = 0.626, p = 0.531). Similarly, Egger's regression intercept showed no significant heterogeneity (t = 0.537, p = 0.605). Finally, assessment of homogeneity using I2 and chi-squared test both confirmed the homogeneity of included studies (I2 = 22.5%, p = 0.236).
Discussion
The present review evaluated the effect of game-based programs for reducing BMI among young people between 5 and 18 years old considered overweight or obese. Ten studies met inclusion and exclusion criteria for the primary meta-analysis, which revealed a small but significant effect of such programs on reducing BMI, particularly those using a combined approach. Country of origin and mean BMI of study participants also influenced the average effect size of interventions.
This systematic review identified only a few studies that examined the impact of game-based interventions on improvement in weight management of children or adolescents who were overweight or obese. However, there are many studies that describe the negative effects on weight of sedentary behaviors or computer/TV screen time among children and teenagers.41–43 Thus, there is an urgent need to conduct RCTs to identify solutions for reducing BMI in those who are overweight or obese especially using game approach.
Although video or computer games are traditionally sedentary activities, using the main characteristics of such games and including motion and activity (such as active video games) may be useful in improving PA in children and youth. Several systematic reviews have reported the effectiveness of this strategy for increasing PA in healthy children and young adults.18,20,44 However, the situation is different in obese and overweight youths because only a small-to-moderate increase in PA may not lead to weight reduction. A systematic review of the effectiveness of interventions to prevent and manage obesity among preschool children included 32 RCTs in the analysis, and only 12 studies reported significant promising results (37% success). The main components of interventions in their review were: PA, nutrition education, and parent education. The authors also found that weight management interventions had greater impacts on weight loss than preventive measures. 45 The findings of our study are comparable to that review. First, the present study found that 8 articles from 11 reported small but significant results (72% success). Although the types of interventions were different from our review of game-based approaches, this may be due to the age and conditions of studies in the two reviews. The mean age of our participants was 11.7 (SD = 1.4), while that review studied only children ages 2–5 years old. Thus, interventions that target school age children may have greater effect on outcome than those that target younger preschool children. Second, we assessed interventions that sought to manage obesity or being overweight, not preventive interventions as did the studies in that review. In other words, interventions that target overweight or obese children may have better success than those that seek to prevent the problem. However, this does not mean that preventive interventions are not useful or effective, but rather that children and youth who already have a problem may be more receptive to and compliant with interventions for its treatment.
In a review that assessed the effectiveness of exercise on BMI z-score among overweight and obese children/adolescents, effects related to several types of exercise, including aerobic, strength training, and combined aerobic and strength exercise, were examined. The authors reported that combination of strength and aerobic exercises yielded the greatest reduction in BMI z-score. 46 This finding suggests that active video games designed using these types of exercises may be more effective in combating obesity.
In another systematic review, Brown et al. 47 examined intervention studies that focused on diet and PA in children or adults in south Asia to prevent or treat obesity. They found seven studies conducted in children, but none reported significant effects in terms of reducing BMI compared with control groups. However, 20 of the 24 studies in adults reported significant improvement in BMI. 47 Two points are relevant when comparing these results to our findings. First, the location or country in which the study is performed may influence the effectiveness of the intervention. We also found that those intervention studies conducted in the United States had greater effects than those conducted in other countries. This may be related to cultural differences between populations or quality of the planned interventions having to do with the environment and availability of resources and appropriate facilities. Other fact that may explain this difference includes the nature of obesity and its consequences that may be perceived differently in different regions of the world based on factors such as knowledge, attitude, beliefs, values, as well as social support and social worthiness. Individuals may choose to participate in such interventions to address their weight problems with higher or lower degrees of intention and willingness, which may affect the results reported. Second, these findings may vary depending on differences in success of intervention in children vs. adults. In the Brown et al. 47 review, similar to several studies in our review, the interventions produced no significant reduction in BMI among children, but many of the intervention studies in adults produced significant improvement in BMI (83%). This finding has been replicated in other intervention studies that have addressed childhood obesity.48,49 However, when interpreting the results of Brown et al.'s 47 review we must consider that the types of interventions assessed in their study were diet and PA and did not include game-based interventions. In addition, measuring children specific measures of BMI such as BMI z-score or percentile may lead to differences in effectiveness.
Regarding the effectiveness of exergames on obesity related outcomes, results of a systematic review of 18 RCTs conducted in children revealed only 4 studies that reported no significant results in terms of outcomes such as BMI, PA, or weight between intervention and control groups. 50 Similarly, Zeng and Gao 51 in another review that assessed the relationship between exergaming and obesity in youth found that there was a positive impact on BMI, body composition, and body fat in four out of seven RCTs that were included.
Although the results of this meta-analysis indicated that game-based interventions may have a significant impact on BMI reduction in children and teenagers, the effect size of this impact is relatively small compared to what others have found. For example, in a review that assessed lifestyle interventions for the treatment of overweight children, trials with no-treatment controls showed an effect size of 0.75, whereas trials with education/information-only controls produced an effect size = 0.48. 52 Moreover, any reduction of BMI z-score >0.25 has been recognized as an improvement in body composition and cardiometabolic risk among obese adolescents. 53 Therefore, the BMI z-score effect size reduction of 0.18 in the current study raises questions about the clinical significance of these interventions. This suggests that game-based interventions alone may not be sufficient to improve weight loss in this population, and supplemental measures are necessary.
Ahn et al. 54 used a combination of interventions, including health-coach visits, dietitian visits, and PA consultations provided over 1 year in obese adults, finding that combining different interventions together increased weight loss and resulted in more long-term changes. This finding is consistent with our results when grouping studies by intervention type. When studies used a combination of other interventions together with active gaming, the effect size increased considerably (nearly twice greater than when game-based interventions were used alone). When several types of intervention are administered, the weak points of each intervention may be addressed by others and in this way enhance their quality and effectiveness. This combined approach has been now suggested by several authors.55,56 Another advantage of the combined approach is that this can address a continuum of participant needs, such that a person who may need psychological readiness to be involved in active gaming (to progress from pre-action stages into action stage based on the transtheoretical model of behavior change), 12 using a psychoeducation component, will help to encourage increased involvement in the program. Likewise, knowledge and attitude are defined as the prerequisites of the behavior change, and focusing on these components together with active gaming may help to motivate involvement in the program.
Another important finding of the current study was that the outcomes of interventions conducted in children with a BMI >30 may be different from those conducted in children with a lower BMI. Obese children appear to respond more robustly to such interventions. This may be due to the fact that obese children perceive greater distress from being overweight and therefore are more active in weight loss programs. This explanation is in line with the health belief model that suggests that when a person feels at higher risk than other people, he or she may participate more vigorously in treatment to reduce that risk. 12 Another explanation may be related to nature of PA prescribed in overweight and obese children. Obese children usually participate in less PA than those who are overweight. Even a small increase in PA may lead to significant weight loss in such children. Several studies have now found that interventions on weight management in obese children have more promising results than in children who are overweight but not obese.57,58
The present systematic review has several limitations that should be considered. First, our review was limited to five databases, studies published in English, and studies where the full text was available. Thus, there may be additional intervention studies in overweight or obese children published in other languages or where only the abstract was available. Given that obesity is an international problem across many countries with different languages, relying exclusively on a single language to come up with a comprehensive appreciation of the problem at a global level is difficult or impossible. However, because many available electronic resources are in English only and translation from other languages requires experts in those languages, we chose to review only those in English. Future review of this type should expand their searches without these limitations. Second, because of limited resources and budget, we addressed only one outcome measure (BMI) in our review. There are other anthropometric and physiologic parameters that could be considered in a comprehensive review. Third, we only included studies conducted on obese or overweight youth, and there are numerous studies on at-risk individuals that assess interventions focused on prevention of obesity in children. Including such studies in future reviews is recommended. Finally, subgroup analysis based on limited number of articles included in the review may have some degree of bias to detect differences, so larger samples are needed within the subgroups to have confidence in making a statement of no differences.
Conclusions
The present review revealed that game-based interventions have a relatively small effect on improving BMI in obese or overweight children. This review indicates that multiple combined approaches are likely to enhance the effectiveness of game-based interventions. For example, using parent education along with other concurrent interventions to modify nutrition and affect behavior may be more effective in reducing weight than any one of these interventions alone. Game-like activities may help to reduce screen time and sedentary behaviors in obese children and adolescent, particularly when combined with other measures to alter lifestyle in obese children. Further assessment of these types of intervention is recommended to obtain a better understanding of how to help children achieve and maintain a healthy weight.
Footnotes
Acknowledgments
The authors thank Prof. Tom Baranowski for critically reviewing our article and his valuable comments that helped us to improve the scientific writing of this study. They also thank the Baqiyatallah University of Medical Sciences for supporting them to conduct this study.
Author Disclosure Statement
No competing financial interests exist.