
Abstract
Abstract
Background:
Childhood obesity prevention interventions have engaged coalitions in study design, implementation, and/or evaluation to improve research outcomes; yet, no systematic reviews have been conducted on this topic. This mixed methods review aims to characterize the processes and dynamics of coalition engagement in community-based childhood obesity prevention interventions.
Methods:
Data Sources: Studies extracted from Ovid MEDLINE, PubMed, and Web of Science; complementary original survey and interview data among researchers of included studies. Eligible Studies: Multisetting community-based obesity prevention interventions in high-income countries targeting children 0–12 years with anthropometric, behavioral, or environmental/policy outcomes. The Community-Based Participatory Research (CBPR) Conceptual Model was used as an overarching framework.
Results:
Thirteen studies met inclusion criteria. Elements of CBPR were evident across all studies with community engagement in problem identification (n = 7), design/planning (n = 11), implementation (n = 12), evaluation (n = 4), dissemination (n = 2), and sustainability (n = 10) phases. Five studies reported favorable intervention effects on anthropometric (n = 4), behavioral (n = 1), and/or policy (n = 1) outcomes; descriptive associations suggested that these studies tended to engage community members in a greater number of research phases. Researchers involved in 7 of 13 included studies completed a survey and interview. Respondents recalled the importance of group facilitation, leadership, and shared understanding to multisector coalition work. Perceived coalition impacts included community capacity building and intervention sustainability.
Conclusions:
This review contributes to a deeper understanding of intervention processes and dynamics within communities engaged in childhood obesity prevention. Future research should more rigorously assess and report on coalition involvement to assess the influence of coalitions on multiple outcomes, including child weight status.
Community-based interventions are an important strategy for preventing childhood obesity.1–7 Interest to intervene in this setting is driven in part by the desire to have a large-scale impact on multiple sectors8,9 and the perceived importance of tailoring intervention design to context. 10 Community coalitions—defined as groups of leaders and stakeholders from diverse organizations, settings, and sectors working collectively on a common objective (sometimes referred to as steering committees, task forces, advisory boards, etc.)11,12—can help achieve large-scale interventions within the local context.
Coalitions may serve as a body to activate and empower community stakeholders and bolster cross-sector collaboration to design, implement, evaluate, and sustain interventions that leverage community assets, leadership, expertise, cultural norms, and systems infrastructure.11–17 These features could be considered mechanisms to achieve desired community-level health outcomes and/or outcomes in themselves. 18
However, despite national and international organizations' recommendations to involve community coalitions in obesity prevention efforts,4,5 little empirical evidence has documented contributions of coalitions to intervention processes and childhood obesity outcomes. This review aims to (1) characterize the processes and dynamics of coalition engagement in community-based childhood obesity prevention interventions, and (2) identify gaps in the literature and recommendations for future investigation and reporting of community-engaged approaches to childhood obesity prevention.
Methods
This research was guided by PRISMA (preferred reporting items for systematic reviews and meta-analyses)19,20 and the Community-Based Participatory Research (CBPR) Conceptual Model: a framework to understand factors related to community coalition work, such as local context and structural (e.g., diversity and formal agreements), relational (e.g., trust and flexibility), and individual (e.g., values and motivation) partnership dynamics that may influence multiple outcomes.21–23 The review was registered with the PROSPERO register of systematic reviews (#42017067822; www.crd.york.ac.uk/PROSPERO).
Information Sources and Search Strategies
The research team compiled search terms based on literature and content expertise (Table 1). Detailed search terms are available in Supplementary Appendix A (Supplementary Data are available online at www.liebertpub.com/chi). Initial database searches included Ovid MEDLINE, PubMed, and Web of Science, completed on October 2, 2015. Searches were updated on January 5, 2017 [timeline extension to accommodate substudy (see Substudy: Survey and Interview Data Collection section below)]. Citations from three relevant systematic reviews were also searched.3,13,24
Summary of Database Search Strategy
Detailed search strategies for Ovid MEDLINE, PubMed, and Web of Science available in Supplementary Appendix A.
CBPR, Community-Based Participatory Research.
Eligibility Criteria
Eligible studies were published in English since 1990, described multisetting community-based interventions conducted in high-income countries, 25 targeted children aged 0–12 years, reported anthropometric, behavioral, or environmental/policy outcomes, and engaged a community coalition in the research process. Studies with older children were included if ages 0–12 years were also represented. Articles with the following characteristics were excluded: reviews, reports, book chapters, observational and qualitative studies, pilot and program evaluation studies not powered to detect change, and focus on treating children with overweight or obesity.
Study Selection
A.R.K. and a trained research assistant screened the study titles. Next, two researchers independently screened each article abstract. E.H. or A.T. was consulted to resolve discrepancies. Finally, A.R.K. and a research assistant read the full text of included articles. To help confirm the presence or absence of coalition involvement, complementary peer-reviewed articles (protocols and process evaluation papers) and/or official reports of studies (e.g., for studies funded by government), if available, were reviewed.
Data Extraction
For each included study, two researchers independently extracted data, including location, study name and years, research/evaluation design, sample (size, age), intervention features (scope, duration), study phases with participatory community engagement (problem identification, design and planning, implementation, evaluation, dissemination, sustainability), 26 coalition description, and primary outcome. Discrepancies were reviewed as a team. If study authors did not state the primary outcome in any associated article, the funding source and/or clinicaltrials.gov were used to source this information. Frequencies and means [± standard deviation (SD)] were calculated in Excel to explore associations between the number and type of participatory study phases by intervention results (positive, mixed, null, and negative). Studies with dual primary outcomes (e.g., BMI and physical activity) were categorized as having “positive,” “null,” or “negative” results if both outcomes fell in the same category; otherwise, studies were categorized as having “mixed” results.
Substudy: Survey and Interview Data Collection
All included studies lacked some level of detail on the coalition's involvement. To address this gap, the principal investigators or senior researchers (“researchers”) of those studies were recruited to complete a survey and interview. Multisite or multicountry studies were excluded from the substudy because of anticipated difficulty of asking one respondent to recall coalition-related information across multiple geographies. In one case, a study participant was also the systematic review principal investigator (C.D.E.; participation approved by the Tufts University Institutional Review Board).
Online survey
Informed by the CBPR Conceptual Model21–23
and gaps in the published literature, the research team created a 28-item web-based survey (Qualtrics) to assess history and context (n = 2 items), partnership dynamics (n = 13), intervention and research processes (n = 11), and impact and sustainability outcomes (n = 2) of community coalitions (Supplementary Appendix B). Items were generated by the research team. Surveys were programmed individually to include the relevant study name and coalition name. Question types varied, including categorical select one or select all that apply items with options, where applicable, to include “Other” open-ended responses or indicate “I'm not sure” to minimize guessing; a 4-point scale to rate coalition activities as a major function, minor function, intended as a function but not carried out, and not intended as a function; and a 10-point scale to estimate level
Phone interview
Four semistructured interview questions were developed by the research team to elicit additional information about the domains described above, with probes addressing coalition leadership, group dynamics, facilitators and barriers to coalition involvement, and perceived impact on intervention outcomes. Interview guides were populated with participants' survey responses to facilitate discussion (Supplementary Appendix C).
Procedures
Researchers' contact information (email and/or telephone) was acquired through existing professional relationships and the Internet. Email or telephone recruitment occurred between April and May 2017. Participants completed the Qualtrics survey between April and June 2017 and a follow-up phone interview conducted by E.H. or A.T. (April–July 2017). Interviews were audio-recorded and transcribed verbatim; transcripts were complemented by interviewer notes. Human subject procedures were approved by the Tufts University Institutional Review Board. Elements of informed consent were provided upon recruitment and survey and interview initiation.
Data analysis
Survey and interview data were analyzed in aggregate. Findings were interpreted based on four CBPR Conceptual Model domains: history and context, coalition partnership dynamics, intervention and research process, impact and sustainability outcomes.21–23 Survey data were analyzed using Qualtrics and Excel to calculate frequencies and means (±SD). Open-ended responses were recoded and categorized when possible. Interview data were analyzed with inductive and deductive thematic analysis and guided by the CBPR Conceptual Model.21–23 A.R.K., A.T., and C.F. generated an initial structural codebook using two transcripts over two rounds of iterative coding. A.R.K. independently coded all interview transcripts and made codebook modifications. A.T. reviewed this work and discussed further modifications with A.R.K., adapting ∼20% of the codebook structure. All researchers contributed to thematic analysis and selection of representative quotes. Themes were organized into a visual guiding framework to facilitate analysis and interpretation.
Results Synthesis
All available data were analyzed for common themes using qualitative synthesis.
Results
Study Selection
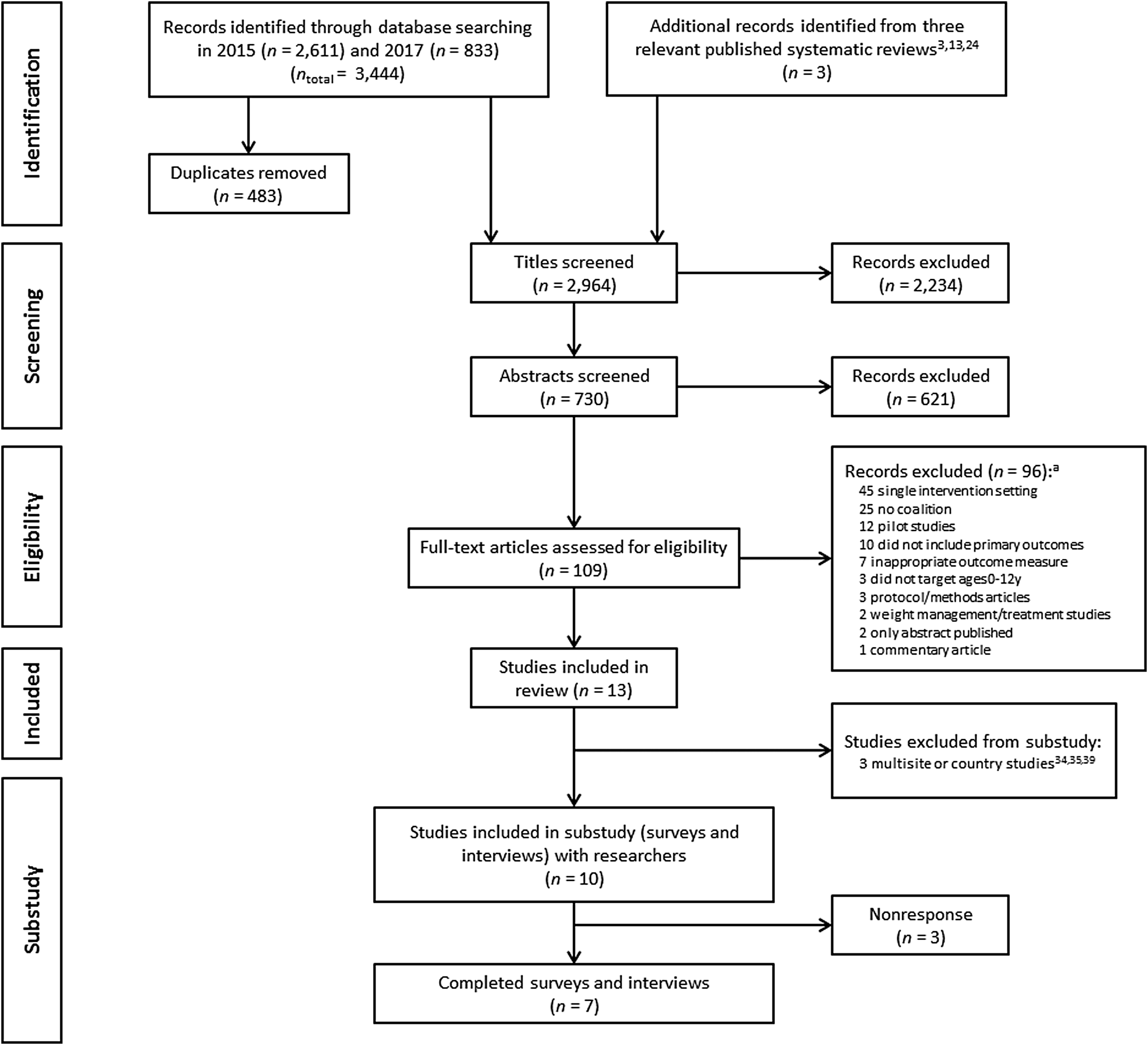
The study selection process is given in Figure 1 with 2964 records identified and 109 full-text articles screened for eligibility. Thirteen studies met all the inclusion criteria and were included in the review.27–39
Study Characteristics: Published Literature
Table 2 includes study descriptions extracted from the published literature. Studies were conducted between 1999 and 2016 in the United States (n = 8),27–34 Europe (n = 2),35,39 and Australia (n = 3).36–38 Intervention durations ranged from 6 months to 5 years. There was one randomized controlled trial, 30 nine nonrandomized controlled trials,27,29,31–33,36–39 two pre-post nonexperimental designs,28,35 and one nonexperimental design with postdata collection only. 34
Study Characteristics of 13 Studies Included in the Systematic Review, Organized by Primary Outcome, Results, and Alphabetized by Study Name; Data from Published Peer-Reviewed Literature and Reports
The article narrative includes citations for studies' primary outcomes paper, whereas this table includes additional citations if applicable (e.g., process evaluation article that includes information about the coalition's involvement). Mebane on the Move and Switch what you Do, View, and Chew had primary anthropometric and behavioral outcomes and therefore these studies are presented twice in the table; study characteristics (e.g., location, intervention description, and coalition description) are included in both anthropometric and behavior sections for ease of interpretation.
Protocol for a separate 2-year school-based evaluation of Programa Thao-Salud Infantil that includes information about the coalition.
Policy wins definition: “concrete, quantifiable movements toward improving local environments and policies to support children's healthy eating and active living that were directly traceable to grantees' CCHE interventions and obtained during or within 6 months postintervention.” (page 918). 34
EPODE, Ensémble Prevenons l'Obesité des Enfants (Together Let's Prevent Childhood Obesity); IDEFICS, Identification and prevention of Dietary- and lifestyle-induced health EFects In Children and infantS; Niños Sanos, Familia Sana: Healthy Children, Healthy Family; Programa Thao-Salud Infantil: Thao-Child Health Programme; N/A, not applicable.
Most studies included anthropometric primary outcomes (n = 12), including BMI z-score,27–30,33,36–38 overweight and obesity prevalence,31,35,39 and infant rapid weight gain. 32 Two studies had anthropometric and behavioral primary outcomes, each with assessments of BMI z-score in addition to physical activity 27 and screen time, 30 respectively. One study assessed policy outcomes. 34
Three studies reported using a CBPR approach28,29,33 and two studies reported participatory community engagement in all study phases.28,29 Table 3 shows the frequency of community-engaged study phases presented alongside study results (positive, mixed, null, and negative). Across the 13 included studies, community members engaged in an average 3.5 ± 1.6 phases, including problem identification (n = 7),27–29,31,34,36,37 design and planning (n = 11),27–34,36–38 implementation (n = 12),27–30,32–39 evaluation (n = 4),28,29,37,38 dissemination (n = 2),28,29 and sustainability (n = 10).27–30,32,34–38 Descriptive associations suggested that the five studies with positive findings on BMI z-score,28,29,38 BMI z-score and physical activity, 27 and policy change 34 tended to engage community members in more phases (4.8 ± 1.1),27–29,34,38 than studies with mixed (n = 2; 3.5 ± 0.7),30,36 null (n = 4; 3.0 ± 1.4),32,33,35,37 and negative results (n = 2; 1.5 ± 0.7).31,39
Community-Engaged Research Phases Presented Alongside Study Results
Data from published peer-reviewed literature and reports of 13 studies included in the systematic review are given.
SD, standard deviation.
Substudy: Surveys and Interviews
Studies and participants
Ten of 13 studies included in the review were eligible for the substudy,27–33,36–38 with three multisite studies excluded.34,35,39 Of the 10 researchers recruited, seven participated in the survey (4–23 minutes to complete) and interview (20–35 minutes) and three did not respond to recruitment efforts. Data were collected an average of 9 years (median: 9 years; range: 5–12 years) after the interventions concluded. Respondents' coalition roles included chair/leader (n = 4), member (n = 3), researcher/evaluator (n = 2), observer (n = 1), and meeting facilitator (n = 1). Three respondents reported dual roles of chair/leader and member.
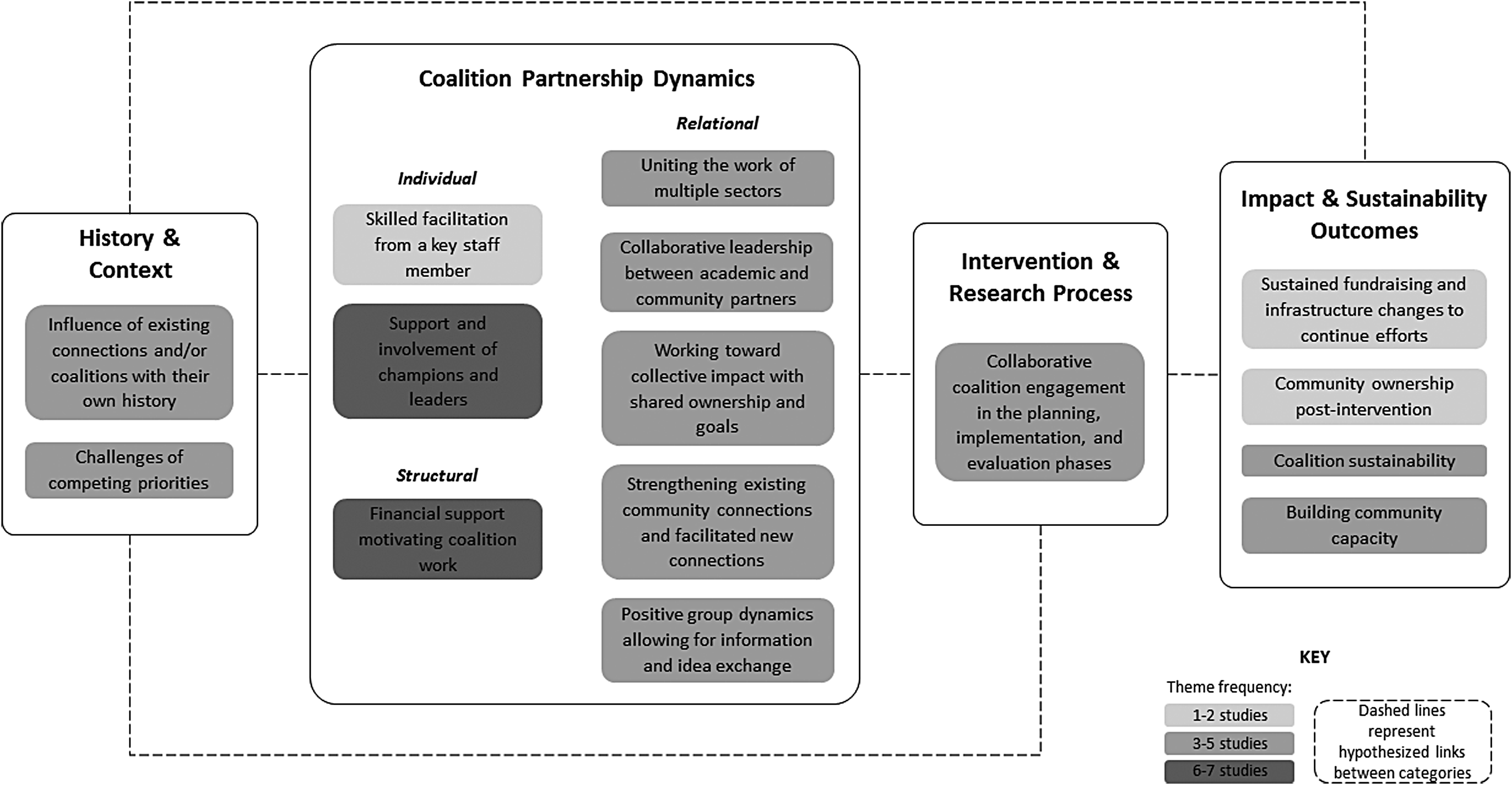
Figure 2 illustrates aggregated interview findings with 15 emergent themes presented as a guiding framework. Representative quotes for select themes are included in the narrative hereunder.
History and context
Survey respondents reported various reasons for having the coalition involved in the study, with project design/planning (n = 5) and implementation (n = 4) as the most common. Interviewees cited the importance of existing coalitions and community connections. One respondent explained:
It became very clear that in many of these smaller communities, all these folks had a history of interaction. You know, they've been on the job for a long time. And, they had ways of doing things that we probably weren't very much going to influence. There was history there.
Further, interviewees recalled challenges about competing priorities:
Yeah, I mean just some competing priorities in the community. So, you know, there were people working on elder services, and suicide prevention, you know really important things. But, it was hard to initially get people to understand how this could fit together and competition within a community always exists when there are limited resources… So, that's always a barrier doing community work.
Coalition partnership dynamics
Group dynamics were influenced by a variety of factors:
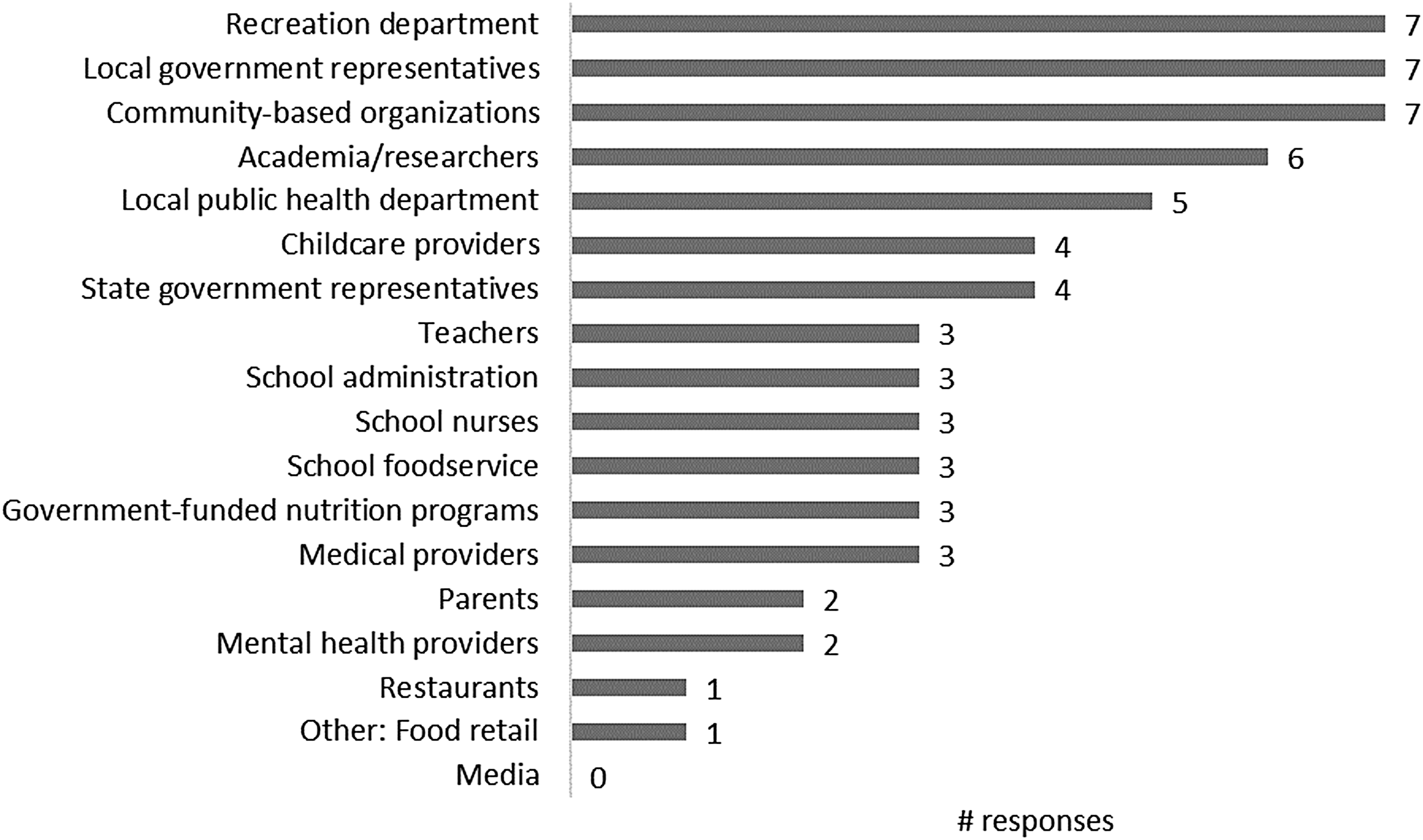
Coalition size and meeting frequency. Survey respondents reported varying coalition sizes: 5–10 (n = 3), 16–20 (n = 2), >20 members (n = 2). Meeting frequency varied: monthly (n = 2), every other month (n = 2), quarterly (n = 2), and unsure (n = 1). Most respondents estimated that about three-fourths of members attended each meeting (n = 5). (ii) Membership. All survey respondents reported coalition representation from community-based organizations, recreation departments, and local government, with a total of 18 groups/sectors cited across studies (Fig. 3). Three respondents recalled that coalition membership changed throughout the study, with members leaving and being added. When asked to characterize the coalition composition, all respondents reported that coalitions represented various sectors or settings involved in the project. One respondent stated that ‘member demographics represented the target population.’ (iii) Structural dynamics. Structural dynamics were influenced by financial support that progressed and motivated coalition efforts. Three of seven survey respondents recalled that coalitions had formal agreements (e.g., subcontracts and memorandums of understanding) to solidify the research partnership. Members of only one coalition received explicit monetary support (e.g., stipends and gift cards) to incentivize involvement. (iv) Individual dynamics. Interview participants recalled the importance of (a) community champions and leaders that garnered support for childhood obesity prevention efforts, and (b) key actors that coordinated and motivated intervention components, such as staff members skilled in facilitation:
The nature of the coordinator was critically important, and having a good facilitating person with strong kind of community-building expertise.
Relational dynamics. Interviewees emphasized the importance of collaborative leadership between academic and community partners involved in the research, and further, the ability to strengthen existing connections and facilitate new connections. This contributed to collective impact with shared ownership and goals across settings and sectors:
The group dynamics were interesting in that everybody was actually committed to the cause, to the eventual objective. They saw it was a problem, they saw it was sitting in their area, that they had a role, that they wanted to see something done collectively. So, I think there was a coherence around what we were trying to achieve… I think in the end it was that, um, that common vision, I guess, and that energy that went towards, that carried it through all of the back and forth.
I remember we did have a lot of logos banging into each other, and they all wanted their little piece and their area and their objective… we kind of found ways where they can add things to the total and that the total becomes more than the sum of the parts was, I think, a part of the strategy.
This common vision and commitment may have facilitated knowledge sharing among coalition members. One respondent explained:
I think generally speaking, it was a pretty interactive group. They didn't just sit and listen, they were exchanging ideas and information, and I think generally speaking it was positive.
Survey respondents estimated that from 1 to 10, on average, coalition knowledge about childhood obesity prevention increased from intervention beginning [5.4 ± 2.1 (range: 3.0–9.0)] to end [8.7 ± 0.9 (8.0–10.0)]. Respondents also recalled increases in coalition engagement with the issue [5.9 ± 3.0 (2.0–10.0) to 8.7 ± 1.0 (7.0–10.0)].
Intervention and research process
Respondents emphasized coalition members' roles in the planning, implementation, and evaluation phases of the research. Major coalition functions frequently cited in the survey included networking (n = 6), priority decision-making (n = 6), and local public policy advocacy (n = 5). Common minor coalition functions included data collection (n = 4) and disseminating research findings (n = 4).
As explained by one interviewee, coalition study involvement was critical for adapting interventions to fit local contexts:
It meant that the intervention itself was tailored and we didn't miss the mark. And before we put any intervention out and rolled out any sort of intervention, we knew it was going to work because we talked it through with a number of really key and motivated providers in that area. And they were able to fine-tune it for us.
Impact and sustainability outcomes
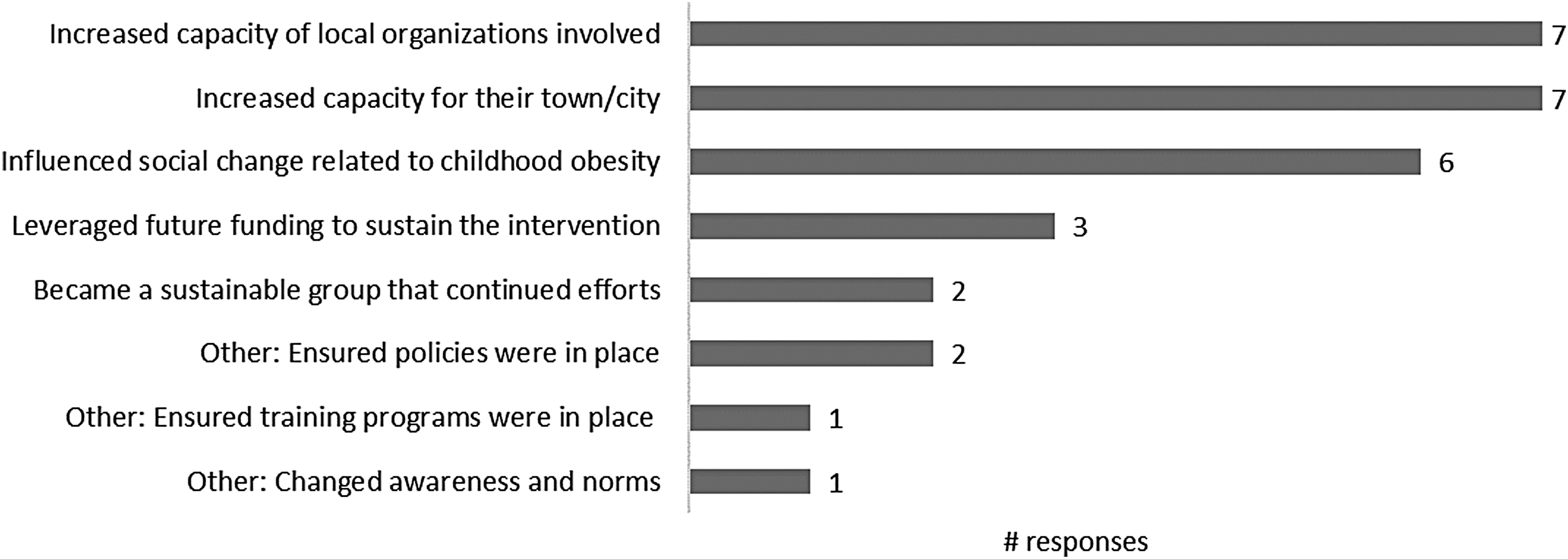
All survey respondents reported that main achievements of coalitions included capacity building for the town/city and organizations involved (Fig. 4). Six of seven respondents recalled the coalition influencing social change about childhood obesity. Sentiments about sustained community ownership and capacity building were also expressed in interviews:
I think that the capacity-building was really huge. I think that particularly given the time and space, the fact that we were able to find secure funding and actually see projects and policies implemented in real time was huge… people were empowered to make changes, and they did.
Interview respondents recalled the importance of fundraising and infrastructure changes to sustain intervention efforts:
There were some things institutionalized within the town and the city as a result of the work: a walkability coordinator that became a permanent position, the [intervention] coordinator, and then the Mayor instituting a benefit for city employees around wellness and nutrition and fitness.
Interviewees also addressed coalition sustainability. Some respondents reported that coalitions continued to meet postintervention, whereas others viewed the coalition as a shorter term strategy to enhance study implementation:
These [coalitions] are really useful while a project is active, and they generally don't survive afterward because they don't have that facilitator anymore, but I don't think that means that they weren't useful… because I don't think that is part of the strategy that needs to be sustainable. I think it did its purpose: it helped with the planning and the intervention and the roll out of the project. It did its role and it did what it needed to do. So, I didn't actually need to see those groups being sustainable in their own right. I think what needs to be sustainable is the strategies you put in place and the actions that were in the ground.
When asked how important the coalition was to the study's success, all survey respondents selected the highest category, “extremely important”, from the five-point scale.
Discussion
Elements of CBPR were evident in each of the 13 community-based obesity prevention interventions included in the systematic review.27–39 Community engagement was most frequent in the intervention design/planning27–34,36–38 and implementation27–30,32–39 phases. Five interventions reported favorable findings related to anthropometric, behavioral, or environmental/policy outcomes;27–29,34,38 associations suggested that these interventions tended to have a higher level of community engagement compared with studies with mixed, null, or negative findings. Survey and interview results revealed a variety of individual and group-level attributes that influenced coalition work, including facilitation skills, leadership, and knowledge about childhood obesity prevention, exchange of information and ideas, and shared vision. Respondents perceived coalitions as extremely important to studies' successes, independent of research outcomes. Success may have been attributed to roles of coalitions in building community capacity and sustaining childhood obesity prevention efforts. Quotes from the interviews presented previously also highlight the role of coalitions in effectively tailoring and translating evidence-based intervention strategies to local context. Overall, results emphasize the dynamism of community coalitions and varied contributions to childhood obesity prevention intervention studies.
In 2016, Ewart-Pierce et al. summarized findings from 14 multilevel, multicomponent childhood obesity prevention interventions and concluded this approach holds promise in impacting child behavior and biology. 24 The authors stated that “engaging various stakeholders” (page 362) was concomitant with the multifaceted approach, but provided little discussion of the mechanisms and contributions of stakeholder involvement. Current review findings contribute to this gap by providing detailed information about community engagement processes and dynamics. Findings offer support for stakeholder engagement in multisetting community interventions, but as described below, also elucidate the need for further research.
Using a CBPR framework, this research provides insight to contextual factors, coalition group dynamics, intervention processes, and perceived impacts of coalitions involved in childhood obesity prevention efforts. Findings are supported by a 2015 review by van der Kleij et al. reporting that successful implementation of multisector childhood obesity interventions require collaborative partnerships and human capital. 13 By integrating review findings with original data collected in the substudy, the current research provides insight to factors that facilitate or inhibit implementation efforts.
Owing to eligibility criteria and search timing, some relevant studies were not included in this review (e.g., cited40–43 and discussed below). In a pilot Head Start intervention, parents and other community representatives served on an advisory board—“an intervention in of itself” (page 3)—aiming to empower members to address childhood obesity. 44 Furthermore, relevant published protocols include the Ecological Model of Childhood Overweight study that engages coalitions in “Community Coaching” interventions to improve healthy eating and physical activity environments, 45 and the Canadian Sustainable Childhood Obesity Prevention through Community Engagement initiative that investigates the impact of a multisetting CBPR intervention on childhood obesity outcomes. 46
This review included the Spanish EPODE intervention, Programa Thao-Salud Infantil, 35 but not other EPODE research [e.g., VIASANO 47 (Belgium), OPAL 48 (South Australia)], as these studies did not meet eligibility criteria during the latest database searches. Utilizing a local steering committee, EPODE's overarching community engagement approach leverages community connections, holds decision-making power, and implements intervention components. 49
This study was challenged by the limited information available in the peer-reviewed literature about community coalitions engaged in childhood obesity prevention interventions. To address this gap, researchers should consider publishing greater detail about coalition involvement, perhaps in Supplementary Data if article word limits are prohibitive. Furthermore, rigorous research is needed, particularly studies examining how coalitions influence intervention processes (e.g., participant recruitment and retention and implementation), community-level change, and individual-level outcomes related to obesity risk, and to characterize how coalitions engage in different types of community-based studies (e.g., efficacy vs. effectiveness trials). By understanding such mechanisms, researchers and community partners can strengthen intervention design, implementation, evaluation, and sustainability by coordinating efforts within and across sectors, leveraging existing resources, and responding to local contexts.8,10 New, sensitive, and valid measurement tools and mechanistic models are likely needed to gain new insights into this understudied area, with the aim to understand why interventions do or do not succeed and what approaches may curb childhood obesity rates. 50
Study strengths include rigorous search strategies in three electronic databases at two time points. To address the limited coalition information available in the published literature, review findings were complemented with original survey and interview data from intervention researchers. Because of the emphasis on coalition involvement, appraisal of study quality as traditionally assessed in reviews of controlled trials (e.g., bias, research design, and blinding) was deemed outside this research scope.
Several study limitations should be considered. To minimize heterogeneity, included interventions were conducted in high-income countries 25 that targeted children aged 0–12 years: an important life stage for obesity prevention. These criteria may limit generalizability to interventions in developing nations and among adolescents. Findings were not summarized quantitatively because of the small number of included studies and variability in study design and outcomes. The review was not designed to compare intervention effectiveness with and without coalitions or to understand potential confounding factors (e.g., influence of coalitions on participant retention or intervention dose); therefore, only associations can be cited and conclusions about impact of coalitions on intervention outcomes cannot be made. As demonstrated by the limited information available in the peer-reviewed literature about community coalitions, included studies may be subject to selection bias despite the comprehensive database search terms used (Supplementary Appendix A). Some studies were not represented in the substudy because of a priori exclusion of multisite studies34,35,39 and nonresponse. Responses were perceptions of one intervention researcher and may reflect recall inaccuracies, although questions were designed to minimize guessing. The decision to invite researchers (vs. researchers and/or coalition members) to participate in the substudy was informed by feasibility concerns of acquiring current contact information of community members who historically served on coalitions and the desire to maximize data collected from one type of perspective, allowing for comparisons across studies.
Conclusions
Communities play a critical role in curbing the global childhood obesity epidemic.6,7 This systematic review examined how community coalitions engaged in 13 multisetting community-based interventions. Overall findings revealed leadership roles of coalitions in building relationships, structures, and capacity to implement strategies that promote children's healthy behaviors and weight trajectories. Further research is required to evaluate the impact of community coalitions on intervention implementation processes and child weight outcomes.
Footnotes
Acknowledgments
The authors acknowledge Amy LaVertu for helping to develop the database search strategies, and Sarah Andrus, Michelle Borges, and Brittany Peats for assisting with the searches and data extraction. The authors are grateful to the study participants who generously contributed their time and invaluable insights. This work was supported by the National Institutes of Health (NHLBI and OBSSR, R01HL115485) and the Brookings Institution. The funders were not involved in the study conception, research design, data collection, analysis, manuscript writing, or in the decision to submit the article for publication. The views expressed in this article do not necessary represent the views of the US Government, the Department of Health and Human Services, or the National Institutes of Health.
Author Disclosure Statement
No competing financial interests exist. C.D.E. participated in the substudy as principal investigator of one of the studies included in the systematic review. The Tufts University Institutional Review Board approved her participation upon expectation of unbiased responses.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.