
Abstract
Abstract
Background:
Obesity in children on the autism spectrum (AS) is becoming a significant health concern. The purpose of this study was to identify the predictors of obesity in a cohort of AS youth and to assess the impact of psychoactive medication use while exploring the second-generation antipsychotics (SGAs) dose–response curve.
Study Design:
A nested case–control study was conducted using Quebec public administrative databases. Subjects with AS <18 years [≥2 diagnoses International Classification of Diseases: 9th revision (ICD-9): 299.X] were identified (January 1993 to May 2011). Cases were defined as subjects with an obesity diagnosis (ICD-9: 278.X) during the coverage period and matched to 10 controls for age, gender, and follow-up duration. Potential risk factors for obesity (sociodemographic characteristics, other neuropsychiatric conditions, and psychoactive drug use) were evaluated and analyzed using conditional logistic regression.
Results:
From a cohort of 5369 AS subjects, we identified 135 obesity cases. Among the different risk factors, only SGAs [rate ratio (RR): 1.04, 95% confidence interval (CI): 1.01–1.07] increased the probability of obesity in multivariate analysis. Exposure for ≥12 months increased significantly the likelihood of obesity (RR: 2.01, 95% CI: 1.18–3.42). Higher risk was observed with chlorpromazine-equivalent daily doses ≥100 mg (RR: 2.20, 95% CI: 1.00–4.84). Among SGA users, concomitant antidepressants (per 30-day exposure) slightly increased the probability (RR: 1.08, 95% CI: 1.01–1.15).
Conclusions:
Longer and higher SGA exposure increased the risk of obesity, which has to be considered in relation to the paucity of evidence supporting long-term psychoactive medication use in AS children. Results highlight the need to promote optimal use and interventions to mitigate metabolic side effects of SGAs in this population.
Introduction
Autism spectrum (AS), identified as “Autism spectrum disorder” (ASD) in the DSM-5, is a lifelong developmental condition defined by qualitative and quantitative alterations in social communication and interaction, and restricted and repetitive behavior, interests, or activities. 1 The prevalence of AS is increasing, and was most recently estimated to be between 1% and 2% of all children. 2 Several physical and mental health comorbidities also frequently accompany this condition.3,4 A number of studies have reported that children on the AS are at greater risk of developing obesity compared with their typically developing peers.5,6 Childhood obesity, which is defined as an age-adjusted and gender-specific body mass index at or over the 95th percentile,6,7 has been associated with detrimental health consequences such as type 2 diabetes and cardiovascular disease.7–9 Furthermore, recent findings show that obesity may also affect cognitive function and increase the risk of developing dementia, or other cognitive impairments, later in life.9,10 The increased risk of obesity seen in AS youth could significantly add to the public health burden associated with this lifelong condition.11,12
The etiology of obesity in AS is most probably multifactorial.4,11,13 Age and gender have been shown to have an impact on the development of obesity in AS children.13,14 Although some of the associated factors may be similar to those seen in the general pediatric population, additional risks specific to AS may be at play. 11 These include genetic predisposition, unusual dietary patterns, and reduced physical activity levels.4,11
In addition, a number of co-occurring mental health conditions such as depression, anxiety, aggressiveness, and attention deficit and hyperactivity disorder (ADHD) have been associated with obesity. 15 These various psychiatric comorbidities have been associated with extensive psychoactive medication use and polypharmacy in AS youth.16,17 The median prevalence of psychotropic drug use as reported by 39 studies is 45.7%, 16 which contrasts with the paucity of evidence supporting psychoactive medication use in children on the AS. 17 The medication classes commonly prescribed include antipsychotics, antidepressants, anticonvulsants, ADHD medications, and anxiolytics/hypnotics, often used in combination.16,17
The role of different psychoactive medications used by AS youth in the development of obesity remains unclear. Second-generation antipsychotics (SGAs) have been of particular interest since their impact on body mass index has been previously documented in AS youth.18,19 In a number of studies using the Autism Treatment Network (ATN) registry,20,21 Western Australian Autism Biological Registry, 22 medical chart review, 23 and US HealthCare System Research Patient Database Repository administrative database, 12 no association between psychoactive medication use and obesity was found. However, a link was present in a study based on the US National Survey of Children's Health. 24 Use of SGAs was associated with greater odds of obesity in AS adolescents, 25 and the risk of obesity increased with the number of psychoactive medications used 14 in further studies using the ATN registry. Furthermore, taking various mood stabilizing medications almost doubled the odds of obesity in AS youth in a study based on the US Simons Simplex Community registry. 26
Regardless of their conclusions, all the previously mentioned studies were, however, limited in sample size, and/or could not adjust for medication dosage or duration of use. Very few studies with comprehensive medication data have been published. A study based on a medical database from the US Military Health System using prescription-level data for 27,765 AS children concluded, however, that those on mood stabilizers, antipsychotics, anticonvulsants, and selective serotonin reuptake inhibitors (SSRIs) had increased odds of being diagnosed with obesity. 27 The last study, however, only adjusted for the presence of psychoactive polypharmacy.
With questions remaining on the factors involved in the development of obesity in AS children, our study had two aims: first, to identify the predictors of obesity in a sample of AS youth and second, to provide further evaluation of the impact of psychoactive medications on weight based on robust prescription-level data. Here, we used a population-based nested case–control design among a cohort of young AS individuals to evaluate the link between obesity and factors such as sociodemographic characteristics, other neuropsychiatric conditions, psychoactive drug use, and polypharmacy while also exploring the SGA's dose–response curve.
Methods
Data Sources and Study Sample
Data were obtained from the public health services programs for residents of Quebec, Canada, administered by the Régie de l'assurance maladie du Québec (RAMQ). Demographic data in RAMQ databases include age, gender, demographic region, social assistance status, and date of death. The RAMQ databases include claims for medical services such as outpatient, inpatient, and emergency room visits paid on a fee-for-service basis with an associated ICD-9 (International Classification of Diseases: 9th revision) diagnostic and procedure codes.28–30 Furthermore, the RAMQ databases provide information on medications and pharmaceutical services delivered to those covered by the public drug plan. Medications dispensed during hospitalization are not recorded in this database. The public drug plan covers ∼43% of the Quebec population, including individuals benefiting from social assistance, all residents aged 18–64 without access to a private drug plan with their children, and people aged ≥65. 29 The medication database has been validated for use in pharmacoepidemiological studies.30,31
AS individuals were identified from the medical services database by an algorithm requiring ≥2 diagnostic codes for ASD defined as ICD-9 code 299.X, recorded between January 1993 and May 2011. We included diagnostic codes repeated at least twice to reduce the risk of misclassification 32 in our AS cohort.
Selection of Cases and Controls
A nested case–control design was chosen for this study. Cases were identified among the cohort of ASD individuals by the first diagnosis of obesity (ICD-9: 278.X), which occurred from the beginning of available data as provided by the RAMQ databases. The index date was defined as the date of the first obesity diagnosis, which could occur before or after the ASD diagnosis. Each case was matched to 10 controls (ASD individuals without diagnosis of obesity) for age at the index date (±1 year), gender, and duration of follow-up using the risk set sampling method. Cases and controls of ≥18 years at index date, those not covered by the drug insurance plan for the 2 years before the index date, or those exposed to corticosteroids for at least 14 days during ≥2 months within the 2 years before the index date were excluded.
Exposure to Psychoactive Medication
Exposure to psychoactive drugs in the year before the index date was measured for cases and controls. Drug classes were categorized according to the American Hospital Formulary System, 33 and included anticonvulsants/mood stabilizers (including lithium), antipsychotics (first and second generations), antidepressants, anxiolytics, and ADHD drugs (stimulants and atomoxetine). For those who were exposed, continuous exposure was assessed in the preceding years to calculate cumulative exposure before the index date. The previous follow-up period ended when a gap of ≥3 months without medication was observed. The 30-day periods of exposure for a given class were defined as the total number of exposed days divided by 30. The medication possession ratio (MPR) was calculated by summing days of drug supplied and dividing by the length (days) of the exposure period.
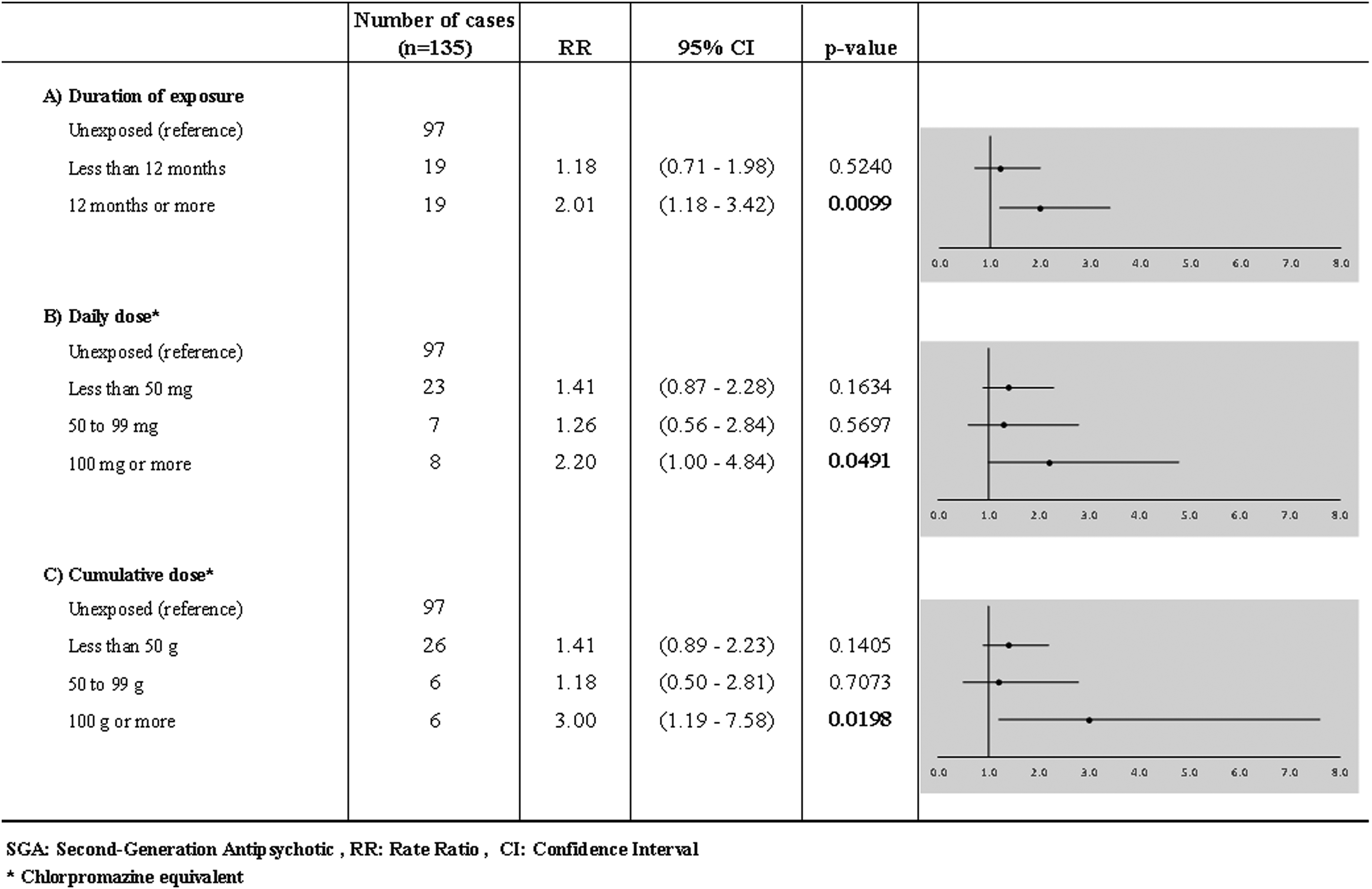
The specific type of SGA antipsychotic dispensed was identified. Exposure to SGA was also stratified in categories in terms of duration (unexposed, <12, ≥12 months), daily chlorpromazine-equivalent 34 dose (unexposed, <50, 50–99, ≥100 mg), and cumulative chlorpromazine-equivalent 34 dose (unexposed, <50, 50–99, ≥100 g). A daily dose of 100 mg of chlorpromazine was considered equivalent to 5 mg of olanzapine, 75 mg of quetiapine, and 2 mg of risperidone. 34
Finally, concomitant use of SGAs with antidepressants, anticonvulsants, or ADHD drugs was evaluated on the basis of 30-day periods. Concomitant use was defined as a period of at least 90 days of overlap between medication classes. A gap of 15 days was permitted between the last day of medication supply and the next fill date (gap of 7 days for the minimal period of 30 days) to account for imperfect adherence and short inpatient stays. The 90-day overlap period was retained since the most stringent definition. 35 Sensitivity analyses were done using minimal concomitant periods of 60 days.
Sociodemographic and Clinical Characteristics
We recorded gender, age, demographic region, and welfare status at the index date. Non-ASD neuropsychiatric disorders (ICD-9 295–298; 300–319; 345) diagnosed within the year preceding the index date were evaluated. These disorders included schizophrenia (ICD-9 295), mood disorders (ICD-9 296; 311), anxiety disorders (ICD-9 300), conduct disorders (ICD-9 312–313), ADHD (ICD-9 314), delays in development (ICD-9 315), intellectual disability (ICD-9 317–319), and epilepsy (ICD-9 345). The characteristics of cases stratified according to SGA exposure (unexposed, <12, ≥12 months) were evaluated.
Data Analysis
Descriptive analyses of sociodemographic and clinical characteristics, as well as exposure to psychoactive drug classes, were conducted for cases (obesity) and controls (no obesity). We replicated these descriptive analyses among cases stratified in categories of SGA exposure (unexposed, <12, ≥12 months). Conditional logistic regressions were used to measure the association between obesity and sociodemographic/clinical characteristics as well as the exposure to psychoactive drug classes. Rate ratios (RRs) and 95% confidence interval (CI) were calculated. The categories of duration of exposure to SGAs (unexposed, <12, ≥12 months), as well as exposure to daily chlorpromazine-equivalent 34 dose (unexposed, <50, 50–99, ≥100 mg), cumulative chlorpromazine-equivalent 34 dose (unexposed, <50, 50–99, ≥100 g), and concomitance with antidepressants, anticonvulsants, or ADHD drugs were also analyzed using conditional logistic regression. In all these analyses, unexposed subjects were selected as the reference category.
A two-tailed p-value <0.05 was considered significant. All statistical analyses were performed using SAS software, V.9.4 (SAS Institute, Cary, NC). The study was approved by the Research and Ethics Committee of the University of Montreal.
Results
We identified a cohort of 5369 ASD individuals between January 1993 and May 2011. A total of 135 cases of obesity were identified and matched to 1350 controls. The prevalence of obesity among our sample was 2.5%. Table 1 presents the sociodemographic/clinical characteristics and exposure to SGAs before the index date for cases and controls. The mean age was 10.3 years (standard deviation = 3.8), and 77% were males. The other characteristics were well balanced between both groups.
Sociodemographic/Clinical Characteristics and Exposure to Second-Generation Antipsychotics
Chlorpromazine equivalent.
ADHD, attention deficit and hyperactivity disorder; Q1, first quartile; Q3, third quartile; SD, standard deviation; SGAs, second-generation antipsychotics.
The proportion of individuals with a prior exposure to SGAs was higher in cases (28.2%) compared with controls (20.8%). Cases had a higher proportion of individuals having used SGAs for ≥12 months (14.1%) compared with controls (7.7%). The proportion of individuals using the highest daily and cumulative doses was also greater in cases than in controls. Among SGA users, 41.1% were also concomitantly taking another psychoactive drug class (antidepressants, anticonvulsants, or ADHD drugs). Concomitant use of SGAs and antidepressants was more frequent in cases (7.4%) than in controls (3.6%). A similar trend was seen with concomitant ADHD drug use (cases: 5.9% vs. controls: 3.8%). The exposure to psychoactive drug classes before index date is presented in Table 2. Around 40% of both cases and controls received at least one dispensation of psychoactive drugs before index date. The average length of exposure to SGAs among users was longer in cases (13.4 months) than in controls (9.8 months). The MPR was at least 60% for all classes except for anxiolytics (<30%).
Exposure to Psychoactive Drug Classes before Index Date
MPR, medication possession ratio.
The sociodemographic and clinical characteristics of cases stratified by category of duration of exposure to SGAs are presented in Table 3. Compared with those unexposed to SGAs, there was a higher proportion of females and of individuals on welfare in the exposed groups. Other neuropsychiatric disorders were present in 29.9% of individuals unexposed to SGAs, in 57.9% of individuals exposed <12 months, and in 68.4% of individuals exposed ≥12 months.
Sociodemographic and Clinical Characteristics at Index Date among Cases According to the Exposure to Second-Generation Antipsychotics
None of the sociodemographic/clinical characteristics was significantly associated with the occurrence of obesity (Table 4). Among the different psychoactive drug classes, use of SGAs (RR: 1.05, 95% CI: 1.02–1.07) and antidepressants (RR: 1.06, 95% CI: 1.01–11) increased the probability of developing obesity by 30-day exposure (univariate analyses). Only SGAs (RR: 1.04, 95% CI: 1.01–1.07) remained significant in multivariate analysis combining all drug classes (Table 5).
Association between Obesity and Sociodemographic/Clinical Characteristics
CI, confidence interval; RR, rate ratio.
Association between Obesity and Exposure to Psychoactive Drugs
Bold indicates statistical significance (p < 0.05).
Compared with unexposed individuals, exposure to SGAs for ≥12 months increased significantly the likelihood of obesity (RR: 2.01, 95% CI: 1.18–3.42) (Fig. 1A). A higher risk of obesity was also observed in individuals who received a chlorpromazine-equivalent daily dose of ≥100 mg (RR: 2.20, 95% CI: 1.00–4.84) (Fig. 1B) as well as those who received a chlorpromazine-equivalent cumulative dose of ≥100 g (RR: 3.00, 95% CI: 1.1.9–7.58) (Fig. 1C). Risperidone was the most commonly used SGA (in 81.6% of cases and 73.3% of controls) (Table 6). Olanzapine and quetiapine were the two other SGAs used in <15% of cases and controls.
Association between obesity and use of second-generation antipsychotics.
Type of Dispensed Second-Generation Antipsychotic among Exposed Cases and Controls
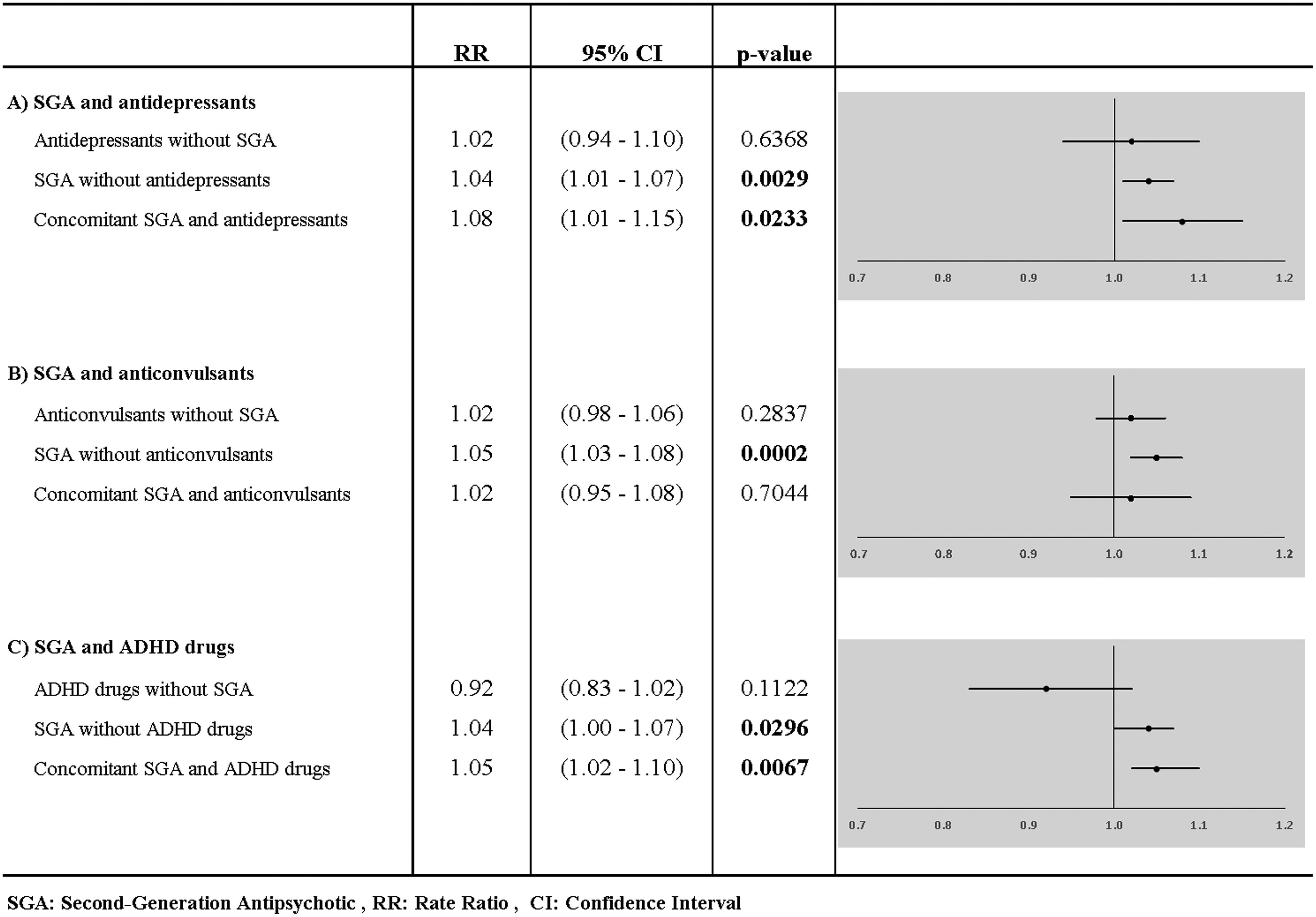
Compared with unexposed individuals, concomitant antidepressant use with SGAs (per 30-day exposure) increased the probability of obesity (RR: 1.08, 95% CI: 1.01–1.15) slightly more than that observed in SGA only users (RR: 1.04, 95% CI: 1.01–1.07) (Fig. 2A). Concomitant ADHD drug use with SGAs also had a greater likelihood of obesity (RR: 1.05, 95% CI: 1.02–1.10) (Fig. 2C), whereas anticonvulsant concomitant use did not influence the occurrence in a significant manner (RR: 1.02, 95% CI: 0.95–1.08) (Fig. 2B). Sensitivity analyses using concomitant periods of 60 days presented very similar results (data not shown).
Association between obesity and use of concomitant medication (second-generation antipsychotics with other psychoactive drug classes).
Discussion
This nested case–control study evaluated the association between obesity and different putative risk factors while also exploring the SGA's dose–response curve in a sample of AS youth identified in the Quebec public Healthcare database. Among the different sociodemographic, clinical, and pharmacologic factors evaluated, only SGAs (RR: 1.04, 95% CI: 1.01–1.07) increased the probability of obesity in multivariate analysis. Psychoactive polypharmacy also had an impact as concomitant antidepressant (RR: 1.08, 95% CI: 1.01–1.15) and ADHD medication (RR: 1.05, 95% CI: 1.02–1.10) users had a greater likelihood of obesity.
The higher risk observed in our sample of SGA users is in accordance with some previously published studies25–27 but in contrast with others.12,20 The inconsistent reported impact of psychoactive medication on obesity might be explained by the different data sources and various study designs employed. Furthermore, only a subset of studies report samples large enough to evaluate the potential impact of different psychoactive medication classes on the occurrence of obesity.
In accordance with our study, Shedlock et al., in a larger sample size study, with similar median age (10.42 years) also found that antipsychotic use without distinction was associated with obesity in AS youth. 27 This study, which also took into account duration of treatment (median antipsychotic days of 330) of different psychoactive medication classes, showed an increase of the obesity risk by 16% for each 33 days of antipsychotic use. Analysis also showed that mood stabilizers, anticonvulsants, and SSRIs were associated with obesity. However, this study only adjusted for psychoactive medication polypharmacy and no other potential confounders such as age or gender. In our nested case–control study, AS individuals were matched for age, gender, and follow-up duration. Although conducted on a much smaller sample, our study yielded a more conservative but still significant impact of SGAs per 30-day exposure, with those exposed ≥12 months seeing their risk of obesity double.
Our study further highlights that not only duration but also SGA dose intensity may have a role to play with the risk of obesity tripling in those having a cumulative chlorpromazine-equivalent dose of ≥100g. The proportion of individuals exposed to SGAs was higher in obesity cases where longer average duration of use and greater chlorpromazine-equivalent daily and cumulative doses were observed compared with controls. Very little data exist on the long-term effects of SGAs in children on the AS. 36 The results of our study highlight the need for careful evaluation of the indication, benefit, and risk associated with these agents while also ensuring proper monitoring and management of untoward weight gain to avoid further cardiometabolic complications. 37
Our results differ from those of de Vinck-Baroody et al. who found no association between obesity and SGAs in multivariate analysis using data collected on children enrolled in the ATN registry where medication use was reported by parents at the time of the initial ATN visit. 20 The mean age (6.45 years) of the children included in their sample was, however, lower than that reported in our study, which may explain the lack of association. According to the authors, it is possible that an older sample of children with ASD might have exhibited a relationship between weight and antipsychotic use, because only 6.1% of their sample reported atypical antipsychotic use.
Interestingly, another study using ATN published by Lake et al. reported that although no association was found in younger children (2–11 years), older SGA-treated children (12–17 years) had ∼3.8 times the risk of being obese. 25 This last study is in alignment with results from Dempsey et al., where children with AS treated for a mood disorder comorbidity with antipsychotics, lithium, or anticonvulsants had nearly twice the odds of being obese. 26 As for studies based on administrative data, Broder-Fingert et al. report no association between obesity and antipsychotic use. 12 However, antipsychotic prescription in the sample was very low (1.5%), which according to the authors may probably be underpowered to detect a difference. Also, as this study was based on prescription data and not pharmacy records, no adjustment could be made for length of treatment.
With respect to other psychoactive drugs, although in our study antidepressants showed an association with obesity in univariate analysis, this was not maintained in the adjusted model for use of other psychoactive drug classes. Depending on the molecule, SSRIs have shown variable association with weight disturbances, whereas mirtazapine, a noradrenergic and specific serotonin antidepressant, is known to cause increased appetite and weight gain. 11 Mood stabilizers such as lithium and some anticonvulsants such as valproic acid have also been associated with weight gain, 11 whereas ADHD medications use is thought to decrease appetite. 4 The low frequency of antidepressants, anticonvulsants, and ADHD drug use in our sample prevented further analysis by specific medication type, and may not have been powered to show an effect among cases. However, using either antidepressants or ADHD drugs concomitantly with SGAs still presented an increased risk of obesity (per 30-day exposure), which is also in alignment with the findings of Hill et al., 14 where obese children were prescribed a higher number of psychoactive drugs that healthy weight children.
As for the sociodemographic and clinical characteristics evaluated in our study, none of the other neuropsychiatric diagnoses, including intellectual disability, was associated with obesity, which was consistent with some previous work.20–22 Youth with significant symptoms of depression or anxiety, however, had 1.5 times the odds of being obese, according to Dempsey et al. 26 Although mental health conditions such as ADHD and depression have been associated with obesity in non-AS children, it is possible that the risk of obesity associated with AS was already strong in our sample and obscured any additional impact of these concomitant disorders. Similarly, socioeconomic status had no impact in our sample, which is consistent with a number of other studies21–23 but not all.13,14
The nested case–control design used in this study allows simple matching of controls with cases on the basis of multiple confounding covariates and provides efficient accounting of multiple time-dependent variables. 38 As an example, the various other neuropsychiatric disorders measured in our study were overall well balanced between cases and controls. Nevertheless, the presence of unmeasured confounding is still possible. Longer duration, higher SGA doses, and psychoactive polypharmacy could be reflective of greater autism severity, a variable that was not available in our study. The impact of autism symptoms and severity on obesity is equivocal with some studies reporting an association20,26 and others not.21–24 Race/ethnicity is another factor unavailable in our data set. Once again, this variable has been linked with obesity in AS children in some13,14 but not all12,21,26 studies evaluating the predictive value of this factor. Although matching within a cohort of autistic children could have, to some extent, controlled for some of the characteristics inherent to autism such as common behaviors related to food and physical activity, variations between individuals and familial environment/factors could not be accounted for. For example, obesity status of parents and siblings has been found to be strong predictors of obesity in AS children. 26 Several of the obesity cases included in our sample were not using any psychoactive medication, indicating that, indeed, other risk factors are at play.
One important strength of this study is that it is based on comprehensive medicoadministrative databases, which allow robust analysis of real-life medication use. Compared with methods such as interviews or questionnaires, using computerized administrative databases avoids recall bias and allows capturing of drug history over long periods. Nonetheless, our population-based study has some limitations inherent to the analysis of administrative databases. First, the diagnostic information in the RAMQ administrative database was not validated for AS. It is, however, recognized that although health service databases cannot identify all cases of AS, those that they contain are generally valid.39,40 The requirement of two or more diagnostic ASD codes also limits the potential for misclassification. 32
Furthermore, obesity was identified using ICD-9 codes, and not actual weight and height measurements. Coding by physicians at this level could be subjective, and does not provide any information on obesity severity or overweight status. Children using psychoactive medications may be more systematically monitored by physicians for their weight because of the known impact of some of these medications, including atypical antipsychotics. However, this bias would be nondifferential since in our study, both cases and controls may be users of psychoactive medication. Moreover, based on practical experience, severe weight variations would need to be present for obesity to be coded by treating physicians in their claims. This may explain the low prevalence of obesity diagnosis found in our sample, which is a limit inherent to the use of administrative databases. It is also possible that obesity present in controls not using SGAs could have been missed due to less stringent monitoring of these children, which would have biased our estimate toward the null.
Second, documented claims for filled prescriptions in the database do not guarantee the actual consumption of a medication. The high MPR seen in drug users of several classes would, however, suggest that these medications are being actively renewed and therefore taken. Third, as mentioned previously, the small sample for certain drug exposures prevented more detailed analysis and may have been underpowered to detect a significant difference. Also, a number of sociodemographic and clinical factors that may have an impact on obesity were not available. Finally, this study excluded individuals with private medical insurance, which may introduce selection bias, as those individuals may exhibit different lifestyle habits, leading to differential drug use.
Conclusion
Several factors may indeed contribute to the development of obesity in AS youth. Treatment with psychoactive medication and polypharmacy, especially with SGAs, may be an aggravating factor in an already susceptible population. Longer and higher SGA exposure increased the risk of obesity in our sample. Further research is needed to better assess long-term impacts of SGAs, and promote optimal use and interventions to mitigate potential associated cardiometabolic risks in AS youth.
Footnotes
Acknowledgments
We thank collaborators from the RAMQ for assistance with the data. We are grateful to the Commission d'accès à l'information du Québec for authorizing the study. Drs. Perreault and Mottron have a National Research Award from the Fonds de recherche du Québec-Santé. Mr. Dorais served as the statistical expert for this research. This study was supported by the Réseau québécois de recherche sur les médicaments.
Author Disclosure Statement
Drs. Perreault, Ben Amor, Ilies, Mottron, Tarride, and Mr. Dorais report no biomedical financial interests or potential conflicts of interest. Ms. Croteau is employed by Pfizer Canada and has direct ownership of stock from Pfizer, Inc. This article was prepared as part of Ms. Croteau's studies toward a PhD degree from University of Montreal.