
Abstract
Abstract
Objective:
To describe prevalence of healthy lifestyle behaviors (HLBs) between two school-age cohorts of racial-ethnically diverse children.
Methods:
Using two Early Childhood Longitudinal Study cohorts (ECLS-K 1999 and 2010), we compared percentage change in HLBs (sleep, physical activity, screen time, and family meals) by child weight groups and within racial-ethnic groups. Weight groups of interest included healthy weight (HW; BMI 5th–84th percentile), overweight (OW; ≥ 85th–94th), obese (OB; ≥ 95th–99th percentile), and severely obese (SO; ≥ 99th percentile).
Results:
OW children within the 2010 cohort reported greater percentage change (range: 2.0%–15.1% increase) in HLBs, whereas HW children demonstrated lower percentage change (range: −6.2% to 8.7% increase). OB and SO children showed significant lower percentage change in reducing screen time (range: −11.0% and −12.7%, respectively). HW Latino children demonstrated the least favorable trends with overall declines noted for 4/5 HLBs. Screen time was noted to have the greatest degree of favorable change (2%–14%) across weight groups, whereas adequate sleep duration demonstrated the lowest favorable percentage change (2%–2.8%).
Conclusion:
Fewer HW and OB children were participating in recommended HLBs compared with OW children in 2010. Recent health campaigns may have helped providers prioritize the identification and counseling of OW children, yet our data suggest that we may be neglecting the role of HLB counseling in OB and HW children. Continued analysis on the social determinants that impact HLBs in school-age and HW/OB minority children should inform how we can best tailor counseling and messages in the coming decades.
Background
Past recommendations on pediatric healthy lifestyle behaviors (HLBs) to address and prevent childhood obesity were previously grounded in adult lifestyle recommendations that were often broad and nonspecific (i.e., “eat less, exercise more”).1,2 More recently, an evidence-based approach to pediatric HLBs has not only yielded positive clinical outcomes across pediatric age groups3–5 but has additionally supported a standardized approach toward what behaviors clinicians, policymakers, and families should be encouraging. The most recent American Academy of Pediatrics Nutrition Committee statement indicated the following as HLBs that promote healthy weight in children: (1) having breakfast on a daily basis, (2) having dinner as a family at least 5 days per week, (3) participating in regular physical activity, (4) having a minimum number of hours of sleep per night, and (5) limiting screen time to <2 hours per day. 6 How children and families have engaged in these HLBs has not previously been described over the course of the obesity epidemic yet. Such an analysis could support their role in predicting child weight outcomes as well as reflect opportunities in how health care professionals (HCPs) are broadly messaging HLBs.
HLBs are related not only to preventing pediatric obesity, but additionally related to promoting healthy weight (HW) in children. Recent study has demonstrated that among a racial-ethnically diverse sample of school-age children, nearly 70% of children were able to maintain a healthy weight (BMI 5th–84th) between the K-5th grade intervals after controlling for other individual factors. Moreover, long-standing racial-ethnic disparities relative to prevalence of overweight and obesity were not observed within the HW category. Although Asian girls were found to have the greatest likelihood of maintaining a healthy weight during this developmental window, white, black, and Latino children were noted to have comparable rates of HW. 7 These data prompt a new set of questions as it relates to HW children that could inform our understanding of how HLBs influence weight risk. For example, what distinguishes HW minority children as it relates to the HLBs they engage in? Is weight risk related to the degree of HLB engagement among minority groups? Are HLBs different among child weight groups? Because lifestyles are heavily influenced by social determinants (neighborhood, food access, and local resources), a focus on HLB variability across racial-ethnic groups could further elucidate strategies in addressing known inequities. Nelson et al. recently demonstrated improved BMI outcomes among low-income black children receiving a lifestyle-focused intervention over their white counterparts suggesting that inequities can be successfully addressed. 8 Thus, a continued focus on HLB variability is important to continue tailoring interventions. Furthermore, a focus on HW children, or children with potential resilience to obesity, and how HLBs are associated could be an as yet untapped clinical and socioecological approach to a pervasive public health problem.
Using two nationally representative samples of children from the Early Childhood Longitudinal Study Kindergarten cohort (ECLS-K 1999 and ECLS-K 2010), a retrospective analysis of both child weight outcomes and healthy lifestyle behavioral changes among a racial-ethnically diverse population of school-age children was possible. Our primary objective was to determine the change in five distinct HLBs (physical activity, bedtime, breakfast intake, family meals, and screen time) between the cohorts for different weight groups. These behaviors were selected as index HLBs secondary to strong behavioral alignment with the “5-2-1-0” pediatric healthy lifestyle campaign endorsed by the American Academy of Pediatrics (AAP) (targeting sleep, fruits/vegetable servings, activity time, and sugary beverages, respectively) 9 Recently, this model has been revised to “9-5-2-1-0” 10 reflecting an added recommendation for sleep duration (9 hours) in light key studies correlating increased risk for overweight with shortened sleep duration.11,12 Although sugary-beverage intake was not assessed by ECLS-K surveys, family meals frequency specific to breakfast and dinner were assessed and subsequently included in our analysis and prior study has demonstrated the protective role of regular family meals against obesity onset. 13 This HLB comparison will provide needed insights into what key behaviors have changed in 10 years among children in all weight categories with a particular focus on HW children. A secondary objective of this study is to report changes in the prevalence of HLBs between racial-ethnic groups. Such a comparison will help understanding of how race-ethnicity as a distal health determinant impact HLBs more proximally among minority children. This targeted racial-ethnic behavioral analysis may inform how to tailor health messages to at-risk populations in the coming decades.
Methods
We used data on kindergarten participants from the ECLS-K cohort of 1999 (n = 21,409) and 2010 (n = 17,038), a nationally representative sample of U.S. children designed and conducted by the National Center for Education Statistics (NCES). The multistage probability sampling design included counties/groups of counties as the primary sampling units, schools within the counties as secondary sampling units, and students within schools as tertiary sampling units. 14
Age, Race-Ethnicity
Child age was reported as a continuous variable with mean age reported in the initial spring waves of data collection for both cohorts. Children were categorized as non-Hispanic white, non-Hispanic black, Latino, and Asian per parent report. An additional category, “other race,” was included and represents children of more than one race, Native Hawaiians/Pacific Islanders, and American Indians/Alaskan Natives.
Child Weight Categories
Participants with complete weight and height assessments available in their kindergarten year of spring 1999 and 2010 were included. As in prior studies using ECLS data, children with biologically implausible height/weight measurements were excluded (i.e., children who had heights decrease on subsequent waves or children with weight gain >20 lbs. per year). 7 This resulted in an exclusion population of 2.5%, or 241 participants. Age-gender-specific BMIs were calculated using reported height/weight with Epi Info 3.5 software. Child BMI was then used to stratify children into weight categories according to Centers for Disease Control definitions: underweight (BMI <5th percentile, healthy weight (BMI 5th– < 85th percentile), overweight (≥85th BMI <95th percentile), obese (BMI ≥95th– < 99th), and severely obese (BMI ≥99th percentile). 15
Healthy Lifestyle Behavioral Variables
Child health
Because HLBs of interest were reported by parents, we thought it was important to assess perceived child health status in combination with understanding parental report of behaviors. This was included given that past study has demonstrated that parental perception of child health is correlated with weight status as well as report of diet and activity. In addition, the report of child health, weight status, and behavior varied among minority populations. 16 Comparing changes in parental perceptions of health between cohorts could shed light on health message changes that occurred within the 10 year interval.
Parents were asked to rate their child's health on a 5-point Likert scale from “Poor” to “Excellent.” This variable was utilized as originally structured (categorical variable) by ECLS-K for our analysis.
Family breakfast and family dinner frequency
Consumption of breakfast has long been associated with positive weight outcomes. Similarly, children who engaged in frequent family dinners (5–7 days) have been found to promote good nutritional health and HW status in children. 13 Family meal frequency was measured in days per week (0–7) for both breakfast and dinner. Number of days per week each meal was consumed as a family was grouped into the following categories for each variable: 0–2 days, 3–4 days, and 5–7 days.
Physical activity
The AAP and American Heart Association recommend children get 60 minutes of physical activity every day to promote optimum health. 6 Parents were asked to determine the number of days in a typical week their child got exercise that caused rapid breathing, perspiration, and a rapid heartbeat for 20 continuous minutes or more. Responses were categorized into 0 days, 1–2 days, 3–4 days, and 5–7 days.
Sleep
Sleep, or lack thereof, is a known modifiable risk factor related to obesity in addition to other health outcomes.4,17 Sleep duration was calculated from the parent responses to two questions: “About what time does your child usually go to sleep on a weeknight?” and “About what time does your child usually wake up on a weekday?” Identical questions were asked related to weekend sleep habits. Weekday and weekend sleep duration were summed and divided by 7 to reflect hours slept per night throughout the week. Sleep duration time was dichotomized to reflect whether the participant did or did not receive the recommended 10 hours or more of sleep per night as designated by the AAP. 6
Screen time
Prolonged screen-time habits are strongly associated with poor nutritional habits, decreased levels of physical activity, and unhealthy weight status. 18 Parents/caregivers were asked to estimate the number of hours their child watches TV during both weekdays in the morning (before 8AM), midday/after school (between 3PM and dinner time), and evening (after dinner time). In addition, weekend TV viewing habits were asked in a similar manner. Weekday and weekend TV viewing times were summed and divided by 7 to obtain daily TV-viewing hours, which was then dichotomized to reflect whether children achieved or exceeded the recommended 2 hours or less of screen time.
Statistical Analysis
The age of the study group was summarized with mean and standard deviation (SD), whereas the gender and race were summarized with counts and percentages. Prevalence of each weight group and HLBs were calculated with their corresponding 95% confidence intervals (CI) for each racial/ethnic group. We compared changes in HLB prevalence within weight groups (healthy weight [HW], overweight [OW], obese [OB], and severely obese [SO]). We further stratified change in HLBs by racial-ethnic groups within each weight category. Percentage change in HLBs between 1999 and 2010 was visually graphed (Figs. 1–4) to demonstrate percentage change by associated behaviors. As both cohorts implemented similar population study designs and research instruments, a robust comparison of child weight categories, racial ethnic groups, and HLB variables was possible. We identified a threshold of 2% as clinically significant change after conferring with general pediatricians within our institution to better target clinically meaningful or observable changes within a large data set.
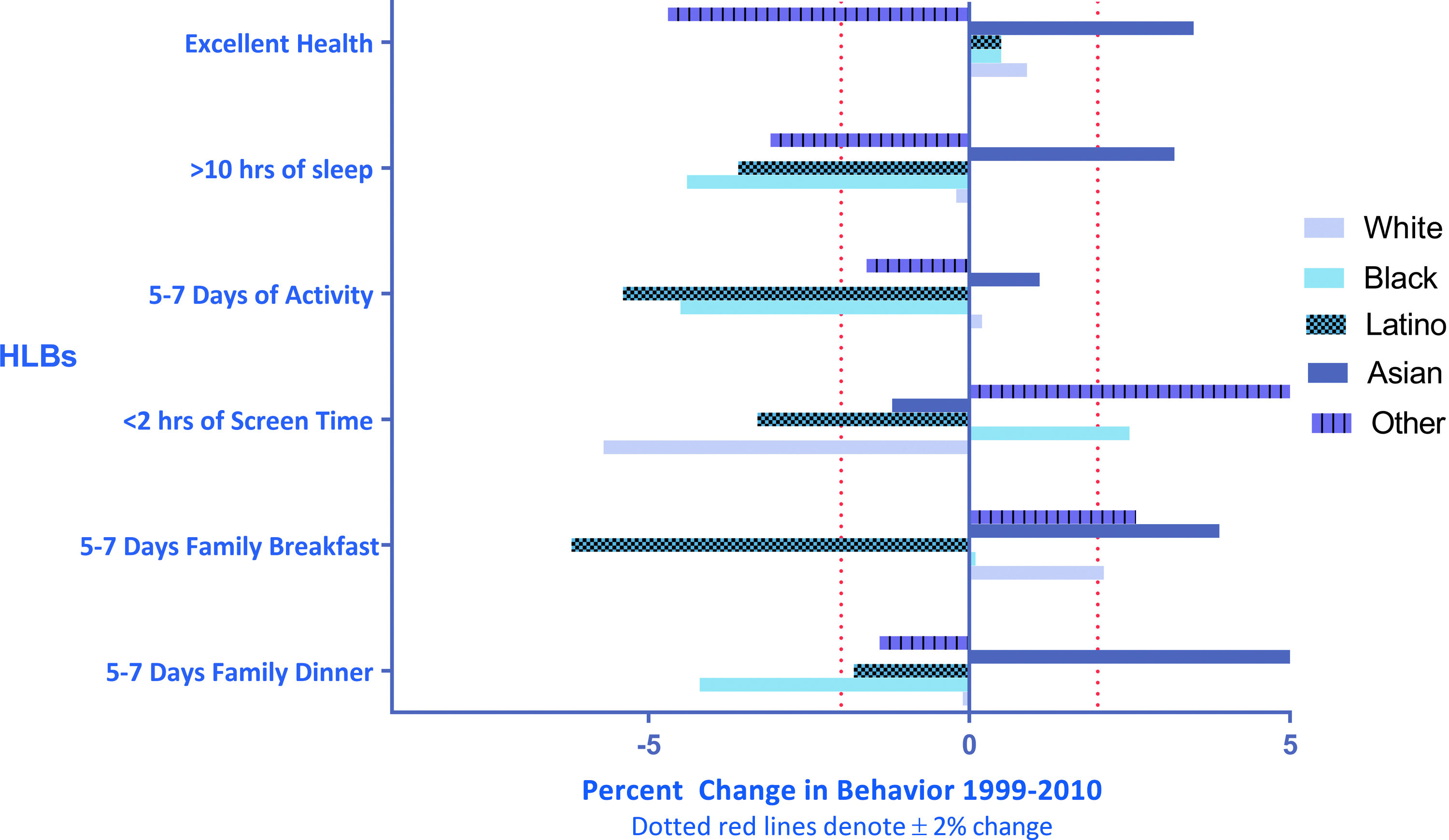
HLB change. Healthy weight children (BMI ≥5th and ≤85th percentile). Stratified by racial-ethnic group. HLB, healthy lifestyle behavior. Color image is available online.
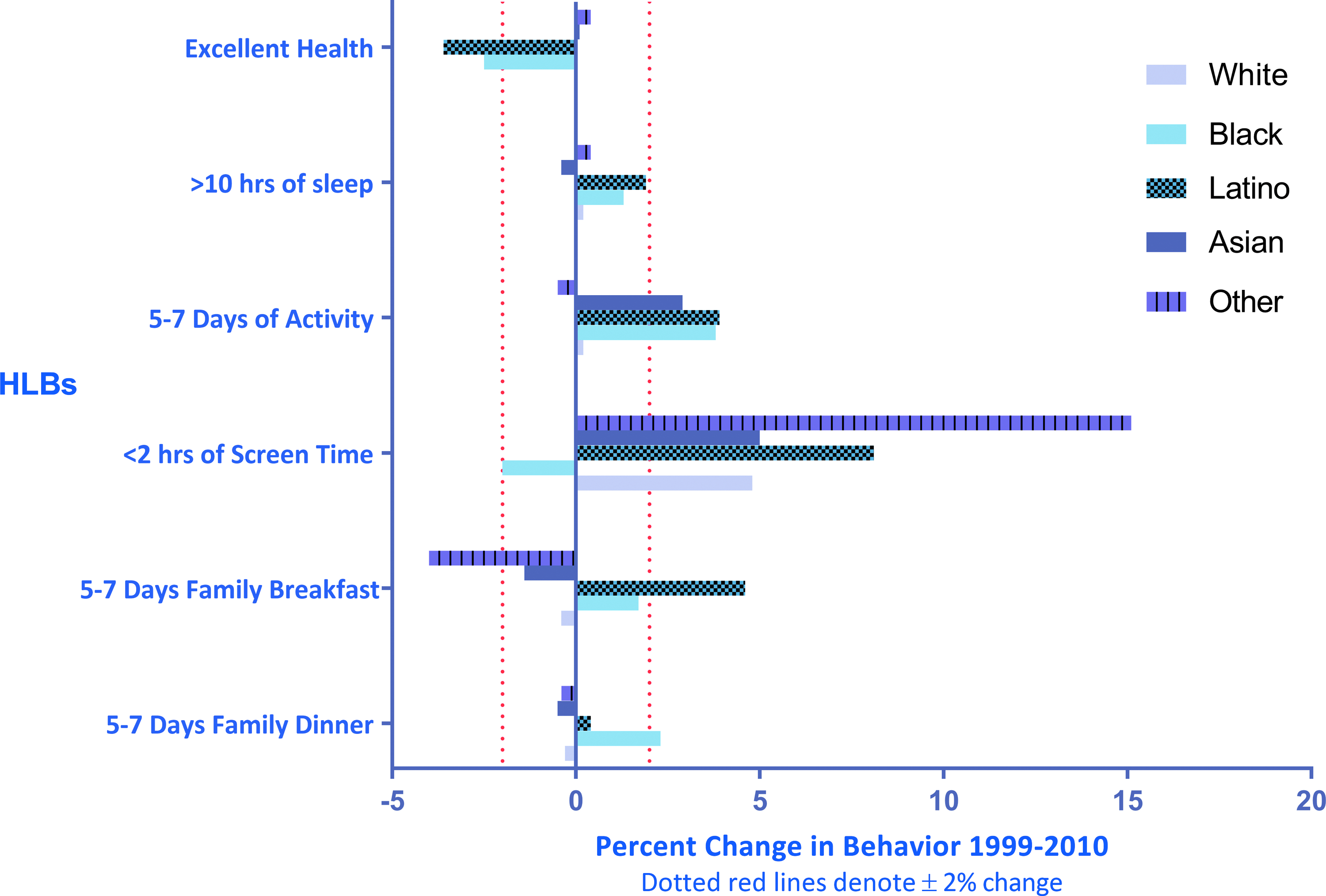
HLB change. Overweight children (BMI ≥85th and ≤95th percentile). Stratified by racial-ethnic group. Color image is available online.
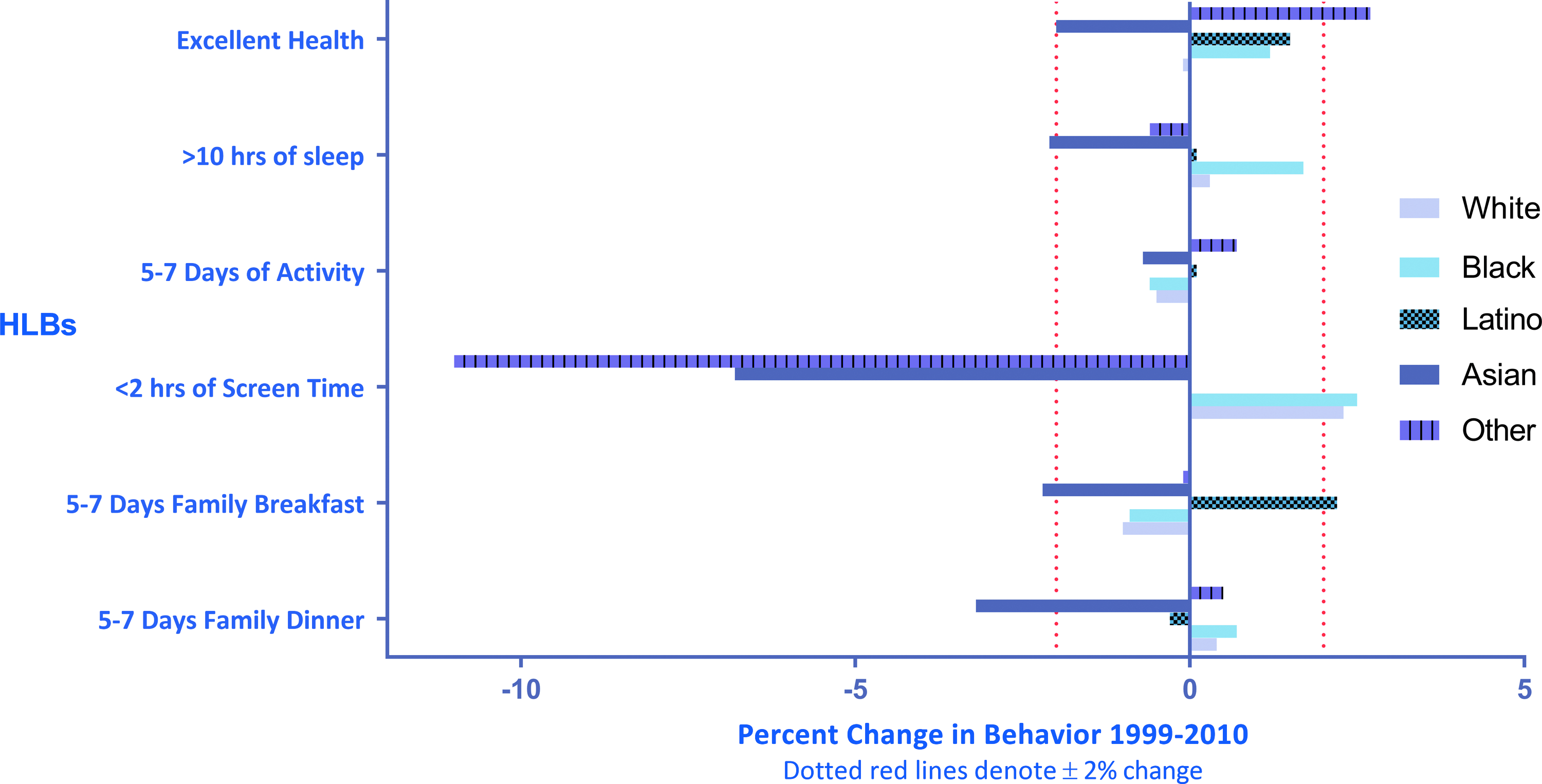
HLB change. Obese children (BMI ≥95th and ≤99th percentile). Stratified by racial-ethnic group. Color image is available online.
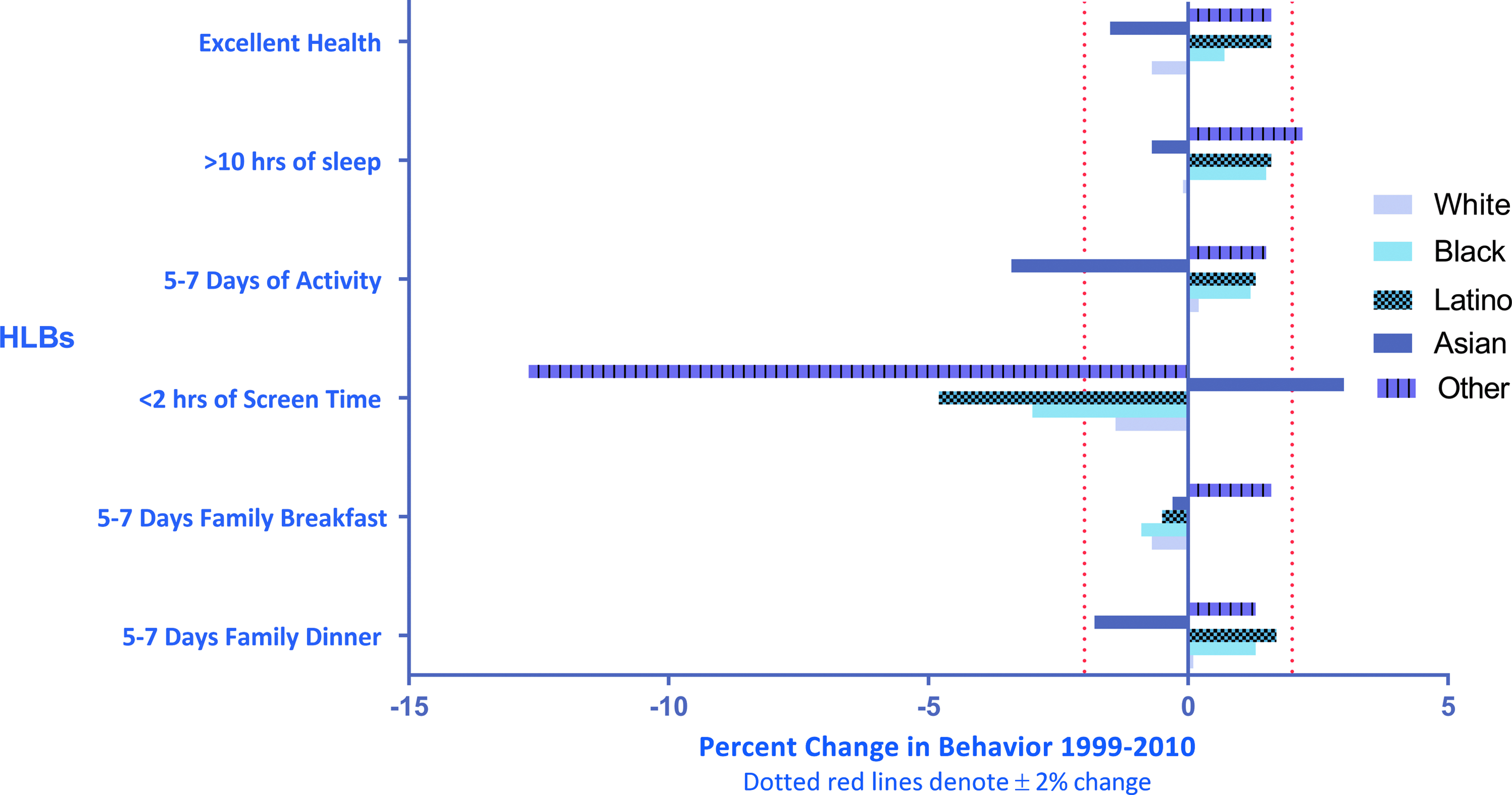
HLB change. Severely obese children (BMI ≥99th percentile). Stratified by racial-ethnic group. Color image is available online.
Owing to the multistage probability sampling and the explicit oversampling of Latino Asian and Pacific Islander children, estimates of prevalence in the study were weighted using design variables provided by the NCES to make population inferences from this sample. This study was approved by the Johns Hopkins University School of Medicine Institutional Review Board. All statistical analyses were performed using SAS v 9.4 (SAS institute, Cary, NC) and SPSS v 23 (IBM Corp. Released 2015. IBM SPSS Statistics for Windows, Version 23.0. Armonk, NY: IBM Corp).
Results
Cohort-specific demographic characteristics are shown in Table 1. The mean age in both cohorts was 74 months (6.2 years) for both males and females. Regarding racial-ethnic distributions, the proportion of children reported as Latino, Asian, and other race were higher (6%, 1.6%, and 1.1%, respectively) in 2010 than in 1999. These changes were an intended ECLS-K sampling outcome.
Demographic Characteristics of ECLS-K Cohort Study Participants
The prevalence of weight-specific categories is reported in Table 2. In 2010, 16.1% of the sample qualified as overweight, whereas 8% of children were OB and 6% SO. Among males in the 2010 cohort, the prevalence of HW showed a clinically significant decrease (71.0%–68.4%). Black children were observed to have a lower prevalence of overweight (2.8% decrease) yet demonstrated an increase in obesity (3.0%). A similar increase was also observed among children of other race (2.8% increase in obesity). Latino and other race children had a significant decrease in the prevalence of healthy weight (2.1% and 3.9% decrease, respectively). Asian children were noted to have a significant decrease in the prevalence of severe obesity (2.2% decrease). A summary table of HLBs trends is also provided (Table 3).
ECLS-K 1999 and 2010 Weight Distributions by Racial-Ethnic Group
Denotes ≥2% change in prevalence.
Directional Change in Healthy Lifestyle Behaviors
NSD, no significant difference observed.
Change in HLBs: Healthy Weight Children
Among HW children, the prevalence of parents reporting their index child as having “excellent health” increased significantly for Asian children (3.5%) but decreased by 4.7% for children reported as other race (Fig. 1). Black and Latino children had significant drops in the reported frequency of participating in 5–7 days of physical activity (4.5% and 5.4%, respectively). Similarly, Latino HW children were the only group to have a significant decrease in the frequency of family breakfasts (6.2% decrease) compared with other groups that showed improvements in this behavior. Black children were observed to have significant declines in the frequency of family dinners (4.2% decrease), whereas Asian HW children were noted to have an increase in this behavior (5.5%).
The prevalence of HW children reporting <2 hours of screen time decreased significantly among white and Latino children (5.7% and 3.3% decrease, respectively). The prevalence of children reporting >10 hours of sleep decreased for HW black, Latino, and other ethnicity children (4.4%, 3.6%, and 3.1%, respectively).
Change in HLBs: Overweight Children
OW black and Latino children were noted to have a decrease in the report of “excellent health” for the study period (2.5% and 3.6%, respectively) (Fig. 2). Black Latino and Asian OW children were noted to have significant increases in the report of 5–7 days of physical activity (3.8%, 3.9%, and 2.9%, respectively).
Improvements in screen time were observed among all OW racial groups with the exception of black children. The magnitude of change was quite variable with the greatest reported change noted among Latino (8.1%) and other race children (15.1%). OW Latino children were the only racial ethnic group that had significant increase in the frequency of family breakfasts (4.6%), yet other race children were observed to have a significant decline (4% decrease). Black overweight children were the only group noted to have significant increases in the report of family dinners (2.1%).
Change in HLBs: Obese and Severely Obese Children
Obese Asian children were noted to have a 2% decline in parental report of excellent health, whereas other race obese children were noted to have a 2.7% increase (Figs. 3 and 4). Report of appropriate physical activity declined only for SO Asians (3.4% decrease) Recommended screen time decreased for OB Asians (6.8%) and other race children (11.0%) yet increased for obese black children (2.5%). In contrast, recommended screen time for SO children decreased for all race/ethnic groups except Asian children (3% improvement). Appropriate sleep duration declined among OB Asian children but improvement for SO Asian children (2.2%).
OB Asian children demonstrated declines in the report of breakfasts and family dinners, yet OB Latino children showed a 2.2% improvement. No significant changes in breakfast or dinner consumption were noted among SO children.
Discussion
Compared with OW children in 1999, a larger proportion of OW children engaged in the indexed HLBs in 2010. Conversely, fewer HW children engaged in key HLBs in 2010 than in the prior cohort. These paradoxical findings, noting favorable HLB change among OW children while observing concerning trends in HW and OB children, may reflect several contextual factors, including parent and HCP interactions. HCPs (e.g., school nurses, pediatricians, and practitioners) remain a primary source of healthy lifestyle recommendations for preschool and school-age children. 19 Because screening and assessment for OW and OB children require that the child meet or exceed ≥85th BMI threshold to be considered at-risk, we hypothesize that HLB messaging from HCPs may have only been disproportionately relayed to OW/OB children. More robust screening resulted subsequent to the recommendation of universal screening guidelines in 2007,6,20 making it more likely that OW children in the 2010 cohort received greater attention to HLB counseling than children in the earlier cohort. This finding is supported by recent study demonstrating that provider attitudes regarding screening and management of children with obesity has steadily improved since 2010 21 although still remains largely underutilized. 22 Thus, from the clinical provider perspective, it is possible that more BMI-focused screening efforts launched just before the 2010 resulted in HCP response bias to the “BMI red flag” and prompted more discussion surrounding HLB behaviors. Similarly, more providers may have been more willing to endorse HLB messages as more neutral lifestyle suggestions among OW or “not yet obese” children with the false assumption that behavioral change was more likely within this weight group.
Although HCP screening efforts have improved for the past 10 years, challenges remain surrounding initiating unbiased and open conversations with parents of at-risk young children.23,24 Many children with obesity encounter significant biases where some HCPs are known to feel negatively about their role in supporting patients and families. 25 Provider reluctance to deliver more formalized lifestyle plans is a known outcome of unaddressed HCP biases. 26 Thus, the declines in HLBs reported among OB and SO children in this study may reflect long-standing cultural challenges surrounding how HPCs perceive children and families with obesity as well as what they perceive their role in addressing this health issue. Other health care setting barriers, including lack of clinical time for focused counseling, concerns regarding lack of reimbursement as well as lack of access to key ancillary staff, are frequently reported barriers. These formidable system-level issues have more recently been targeted in clinical practice where hopeful trends are being observed. 27 Still, it is important to note the potential gaps in past screening and health counseling efforts these data may reflect.
We also observed that OB and SO children had higher rates of “excellent health” reported in the 2010 cohort suggesting that parental lack of perceived health risk may correlate to fewer reported HLBs. Some of the observed HLB declines may thus relate to an interaction between lack of perceived health risk and the extent of counseling that occurred. In fact, campaigns such as Let's Move and 5-2-1-Almost None were early in their dissemination 28 with Campbell et al. showing low parental awareness of these messages in 2009. These temporally related findings suggested that parents within the 2010 cohort were minimally exposed to these broader national health campaigns.
Among the five HLBs assessed, we observed that the behavior with the greatest degree of change to be amount of screen time reported across weight groups. Although changes occurred bidirectionally, this HLB was observed to have consistent favorable change across weight and minority groups. These data indicate that families may find this HLB more actionable at the individual or family level. In past study, screen time has been correlated to parenting style, 29 type of child care utilized, and the presence of screens within bedrooms. 30 With various options and tactics by which to decrease screen time, greater opportunities for both counseling and success may be reflected in our findings. Certainly, a continued emphasis on this behavior at various levels could result in continued favorable momentum across racial-ethnic groups in the coming decade.
Sleep duration >10 hours was the HLB with the lowest magnitude of change reported with only two groups (HW Asian and SO other-race children) demonstrating favorable changes. In fact, we unexpectedly noted that several groups of HW children had significant declines in the amount of reported sleep (black, Latino, and other groups). Our findings relative to screen time and sleep may validate the extent to which interventions during the study period targeted these behaviors. That is, during 1999–2010 there were several HLB campaigns targeting screen time (Let's Move and 5-2-1-Almost None) but very few campaigns targeting developmentally appropriate and adequate sleep. Recently, a variety of interventions have focused on the weight–sleep relationship4,31,32 and new healthy messaging campaigns (9-5-2-1-Almost None) now include sleep as a lifestyle behavioral target. However, the observation that HW children were the groups least likely to demonstrate change in this behavior prompts a refocus on sleep-hygiene among all children in this age group—not simply those with weight issues—as a primary preventive strategy.
Finally, several racial-ethnic differences in HLB engagement were noted. For example, OB Asian children demonstrated declines across all HLBs compared with their racial-ethnic counterparts with the highest magnitudes changes noted related to increased screen time. Identifying the social determinants that might correlate to this finding is an important health equity strategy (i.e., parenting practices, neighborhood environment, and school environment). Similarly, HW Latino children were noted to have significant decreases in four out of five HLBs (sleep duration, daily activity, screen time, and family breakfast). Although declines in HLBs were noted among other HW children, these concerning trends were particularly evident among Latino and black children. Not surprisingly, disparities in HLB engagement among HW children mirror the well-known disparities observed in obesity prevalence such that targeting HLB trends could have favorable epidemiological impacts as it relates to reducing inequities in weight risk.
Past research indicates that parents of minority children are highly receptive to receiving weight-focused guidance from their pediatrician. 33 If HW children remain untargeted within our current screening practices and if key HLBs are not correlated to the child's healthy weight by providers and parents, it is unlikely that families will recognize the value of these behaviors in the child's life course. Continuing a discussion of what is going right for HW children is clearly of value as it relates to forming lasting healthy lifestyle habits. Continuing to rely on the traditional “BMI red flag” to engage children in families in lifestyle counseling, particularly among HW minority children, may perpetuate the same observation in HLBs and weight trends in the coming decades. Potential next steps regarding HLB counseling might include campaigns focused on having HCPs, child care centers, and school nurses engage in HLB discussions specifically among HW kids as a primary prevention obesity strategy.
The strengths to our analysis include the use of two nationally representative data sets of child cohorts separated by a consecutive 10-year time frame. The ECLS-K study design oversampled minority children allowing us to have robust samples to compare behavioral trends between minority groups. The depth of behavioral surveys provided within the data set are also a strength allowing for an accurate comparison between both cohorts. An analysis within this unique window of time provides an opportunity for us to derive some potential “lessons learned” as it relates to key child weight groups as well as at-risk minority groups.
Limitations to our study include the possibility of finding serendipitous behavior changes between cohorts due to the large sample. We identified a 2% change threshold as metric by which to decipher random change versus clinically meaningful change; however, this threshold may still be an overestimate of significant behavior change between groups. In addition, behavior variables were based on parental report, which may be affected by recall bias as well as reporting bias. Still, the consistent interview methodology of ECLS-K and using validated survey instruments may have helped reduced the likelihood of bias.
Conclusions and Implications
Recent health campaigns may have appropriately supported prioritization and identification of OW children by HCPs, yet we should not neglect the role of HLB counseling in obese and HW children. Continued disparities among Latino and other minority children may correlate to missed counseling opportunities in early childhood when healthy weight is achieved. Lifestyle messaging for HW minority children should thus be considered a primary prevention target for future obesity campaigns as should strategies related to engaging parents of children in all weight categories in appropriate sleep behaviors. Similarly, continued analysis on the social determinants that impact HLBs in school-age, HW, and OB minority children should inform how we can best tailor counseling and messages to make health behavior change more salient and ultimately more feasible.
Footnotes
Author Disclosure Statement
No competing financial interests exist.