
Abstract
Introduction:
Social support for healthy eating can influence child eating behaviors; however, little is known about the impact of social support during family-based behavioral weight-loss treatment (FBT). This study aimed to determine the impacts of both baseline and change in family support on change in child diet and weight during FBT.
Methods:
Children (n = 175; BMI percentile ≥85th; ages 7–11; 61.1% female; 70.9% white) and a participating parent completed 4 months of FBT. Parents were active participants and learned social support-related strategies (i.e., praise and modeling of healthy eating). Child perceived family encouragement and discouragement for healthy eating, child diet quality (via 24-hour recalls), and child weight were assessed pre- and post-FBT.
Results:
Family encouragement for healthy eating increased during FBT, and this increase was related to increases in child healthy vegetable intake and overall diet quality, as well as decreases in refined grains consumed. Low pre-FBT family encouragement predicted greater increases in healthy vegetable intake, greater weight reduction, and greater increases in family encouragement for healthy eating. Family discouragement for healthy eating did not change during treatment nor did it predict dietary or weight outcomes.
Conclusions:
FBT successfully improves family encouragement, which is associated with improvements in child diet. Furthermore, even children who began treatment with low family encouragement for healthy eating show great improvements in dietary intake and weight during treatment. Results suggest that changes in child eating behavior during treatment is influenced by active, positive parenting techniques such as praise of healthy eating rather than negative family support.
Introduction
One in three children in the United States have overweight or obesity, 1 putting them at risk for serious health consequences, including chronic medical diseases (e.g., diabetes, cardiovascular disease, cancer) and psychiatric disorders (e.g., depression, anxiety).2–4 Children with overweight or obesity have a high risk of developing severe obesity in adulthood, 5 which highlights the need for early, effective interventions that address the factors contributing to the disease.
Family-based behavioral weight-loss treatment (FBT) is a highly effective intervention for childhood obesity, with over 30 years of research demonstrating its success.6,7 The intervention also aligns with national recommendations for treatment of pediatric obesity set by the U.S. Preventive Task Force Services. 8 FBT uses a comprehensive, family-centered approach to help parents and children develop useful techniques to change eating behaviors that promote lasting weight loss. Indeed, children show reductions in percent overweight (percent above median BMI based on age and sex) of over 10%,7,9,10 and parents lose an average of 28 pounds. 10 Given the effectiveness of FBT and the increase in its utilization, 11 it is important to determine which intervention components are responsible for family success, as it could inform future efforts to refine and tailor family-based childhood obesity treatments.
One core intervention component that could influence child success is family social support. Throughout FBT, parents learn to support their child's behavior change with positive parenting techniques such as praising their child's healthy behaviors, modeling healthy behaviors, and structuring the home environment to facilitate healthy choices. Family support has been linked to long-term weight outcomes for children in FBT 9 ; however, it remains unknown how family support influences child eating behaviors in FBT. Previous cross-sectional data have shown that high family social support for healthy eating behaviors is linked to children's consumption of healthy foods (e.g., fruits, vegetables, whole grains),12–14 and low family support for healthy eating behaviors is linked to consumption of high-calorie, low-nutrient-dense foods (e.g., soda, pastries).13–15 It is important to determine if family support impacts child eating behaviors for children engaged in FBT, given the evidence that dietary intake changes facilitate weight loss.16–18
Therefore, the first objective of the present study was to determine if changes in family social support during FBT were related to changes in child diet quality and weight change. We hypothesized that family support would increase during treatment, and the increase in family support would be associated with increases in healthy child eating behaviors and decreases in child weight. The second objective was to determine whether baseline (pre-FBT) family social support influenced dietary intake and weight changes during FBT. We hypothesized that children with high pre-FBT family social support would have greater improvements in dietary intake and reductions in weight compared with children with low pre-FBT family social support.
Methods
Overview/Study Design
This study used data collected in a multisite, randomized-controlled clinical trial in St. Louis, MO, and Seattle, WA, that evaluated the effectiveness of continuing weight-control interventions. 7 Before randomization to continuing weight-control interventions, participants were enrolled in an initial weight-loss treatment consisting of 16 sessions of FBT over the course of 4 months. The current study is a secondary analysis using data collected from participants at pre- and post-FBT and before randomization to a continuing weight-control intervention (see Wilfley et al. 7 —Supplement 1 for a complete protocol description).
FBT targets improvements in diet and activity behavior. The Traffic Light Diet 19 is used as an easy system to help families improve diet by consuming fewer servings of “Red” foods (nutrient-poor, high-calorie foods and drinks such as cookies, pastries, and sugar-sweetened beverages [SSBs]); consuming more servings of “Green” foods (nutrient-dense, low-calorie options such as fruits and vegetables); and sticking to daily calorie goals. Parent support for healthy eating is also a treatment target. A participating parent is actively engaged in treatment by working toward his/her own behavioral and weight-loss goals and learning parenting techniques that support the child's eating behavior changes, such as modeling healthy eating behavior, using positive reinforcement (e.g., praise vs. nagging/criticizing), and modifying the home environment to facilitate healthy food choices. FBT also recommends that all family members (e.g., both parents and siblings) participate indirectly by supporting healthy changes in the family's lifestyle.
Participants
Children (ages 7–11 years) with overweight or obesity (BMI ≥85th percentile for age and sex) who had at least one parent with overweight or obesity (BMI ≥25 kg/m2) were recruited, and a designated parent participated with the child. Participants were excluded if they were in another weight-control program, had psychiatric conditions that would interfere with treatment, were taking medication that affected their weight, had low English comprehension, and/or had a physical condition that would prevent them from doing physical activity or consuming a healthy diet as recommended by the treatment. Parents signed a written informed consent form, and children signed a written assent form. The study was approved by the Institutional Review Board at each site (Washington University School of Medicine in St. Louis and Seattle Children's Research Institute). The sample for the present study is limited to the eligible 175 children who completed FBT and all pre- and post-FBT measures required for analyses.
Measures
Demographic questionnaires were completed pre-FBT. All other measures were assessed pre- and post-FBT.
Demographics
Parents reported their marital status and education and their child's age, sex, race/ethnicity, and the family's annual household income. Annual household income was reported categorically ranging from 1 (under $9,999) to 11 (over $100,000).
Weight change
Researchers measured child weight and height with light clothing and shoes removed. Percent overweight (i.e., percentage that the child's BMI is above the median BMI for his/her age and sex) and BMI z scores were calculated using the Centers for Disease Control growth charts. 20
Social support
The Social Support and Eating Habits Survey (SSEH) assessed the child's perceived social support for healthy eating. The SSEH has demonstrated criterion and discriminant validity for adult samples, 21 and the version that we use in the present study has been successfully modified for child samples, including children ages 7–11.22,23 The subscales used to analyze positive and negative family social support were family encouragement (α = 0.75) and family discouragement for healthy eating (α = 0.72), each assessed with five items. Encouragement for healthy eating is an action that supports children to eat healthy foods or not eat unhealthy foods. Family discouragement (i.e., “negative support”) for healthy eating is an action that supports children to eat unhealthy foods or not eat healthy foods. For all items, children rated how often a given eating-related situation occurred with their family, using a five-point scale (1 = never to 5 = very often). Example items for family encouragement for healthy eating are “my family complimented me on changing my eating habits (‘Keep it up’)” or “helped me not to eat ‘unhealthy foods’ (cake, salted chips) when I'm wanting to do so.” Examples of family discouragement items are “my family ate high-fat or high-salt foods in front of me,” “got mad when I asked them to eat low-salt, low-fat foods,” or “brought home foods I am trying not to eat.” Responses were summed for each subscale separately; scores could range from 5 to 25, with higher scores indicating greater frequency of encouragement or discouragement for healthy eating.
Eating behavior
To measure child eating behavior, expert interviewers conducted three telephone-administered 24-hour recalls using the Nutrition Data System for Research nutrient calculation software. 24 The recalls were collected on nonconsecutive random days within 2 weeks, and because dietary intake changes throughout the week, 25 recall days included at least one weekday and weekend day. Parents reported on the child's dietary intake for the previous day. The child also contributed if he or she was available, as using both parent and child reports improve the recall's completeness.26–28 Parent-reported 24-hour recalls of child dietary intake have been validated against the doubly labeled water method for measuring child dietary intake. 24 Interviewers followed standard protocols to ensure complete and accurate food recalls, including the multiple-pass method, 25 and participants were provided the Posner two-dimensional food portion visual aid 24 to use during recall. After averaging assessments from all three recall days, total servings of fruits (excluding juices), healthy vegetables (excluding fried and/or starchy vegetables), refined grains, and SSBs were calculated. Fruits and vegetables were specifically analyzed because they were heavily targeted in the intervention as “Green” foods to increase in the Traffic Light Diet. 19 Refined grains were analyzed because many of the “Red” foods that the intervention aimed to decrease were refined grains (e.g., cookies, pastries), and SSBs were also targeted as “Red” items to decrease. The Healthy Eating Index-201529 was calculated to provide a general metric of diet quality. HEI-2015 scores range from 0 to 100, with greater scores indicating greater adherence to USDA eating recommendations. 29
Data Analysis
Residual diagnostics were evaluated for each model using histograms, normal P-P plots, and plots of standardized residuals against predicted values. Logarithmic and reciprocal transformations were applied to data with non-normal residual distributions (i.e., SSB, fruit, and healthy vegetable consumption). In all models, child age, sex, race, and ethnicity; parent marital status and education; and family annual household income category were tested as potential covariates. Child percent overweight was also tested as a potential covariate in models relating to dietary outcomes. Because no variables were significant covariates, all models were run without covariates.
Paired-samples t-tests examined the change in support, eating behaviors, and weight during FBT. Multivariate repeated-measures general linear models, with time from pre-FBT to post-FBT as the within-subjects factor, tested the relationship between change in dietary and weight variables and change in social support. Repeated-measures general linear models, with time from pre-FBT to post-FBT as the within-subjects factor, evaluated how pre-FBT support was related to the change in dietary intake and weight from pre- to post-FBT. Least significant difference post hoc analyses were conducted for models with significant time-by-change in diet interactions. An alpha level of p < 0.05 was set to determine significance, and SPSS version 25 was used for all data analyses (SPSS Inc., Chicago, IL).
Results
Sample Characteristics
Baseline descriptive statistics of the participating children (N = 175) and parents (N = 175) are reported in Table 1. Participating children had a mean age of 9.5 (SD = 1.3) years; the majority were female (61.1%), white (70.9%), non-Hispanic (89.7%), and from a household with an annual income of ≥$60,000 (68.0%). Child BMI z score ranged from 0.99 to 2.85, with a mean of 2.17 (SD = 0.39). When comparing our sample of children who completed FBT with those who did not complete FBT, we found no statistically significant differences across child gender, age, race, ethnicity, BMI z score, household income, or baseline family support (p's > 0.05).
Baseline Sample Characteristics
One family chose not to report.
Changes in Social Support and Diet from Pre- to Post-FBT
See Table 2 for means and test statistics for social support, eating behaviors, and weight. Pre-FBT family encouragement and discouragement were significantly correlated with post-FBT family encouragement and discouragement, respectively (r's = 0.19–0.34, p's < 0.01). Child reports of family encouragement of healthy eating increased from pre- to post-FBT [t(171) = −7.10, p < 0.001]. Not unexpectedly, post hoc independent-samples t-tests revealed that children with low pre-FBT family encouragement demonstrated greater increases in family encouragement from pre- to post-FBT (M = 6.6, SD = 5.4) than children with high pre-FBT family encouragement [M = −0.6, SD = 5.4, t(170) = 8.59, p < 0.001]. Child BMI z score decreased from pre- to post-FBT [t(173) = 15.64, p < 0.001].
Paired-Samples T-Tests for Social Support, Eating Behavior (Daily Averages), and Weight from Pre- to Post-Family-Based Behavioral Weight-Loss Treatment (n = 175)
Changes in dietary and weight outcomes that were previously reported from this trial, including reductions in SSB intake and increases in fruit and healthy vegetable intake,16–18 use slightly different samples, based on which participants completed measures needed for analyses, and therefore, means reported in Table 2 differ slightly from previously reported means.
Means in bold are significantly different from pre- to post-FBT.
FBT, family-based behavioral treatment; SD, standard deviation; SSB, sugar-sweetened beverage.
Overall, child diet quality increased from baseline to post-FBT. HEI-2015 scores significantly increased from pre- to post-FBT [t(173) = 7.09, p < 0.001]. Correspondingly, significant changes in dietary intake from pre- to post-FBT for specific food groups were observed, including increases in healthy vegetable [t(173) = 3.02, p < 0.01] and fruit [t(173) = 8.67, p < 0.001] intake. Refined grain consumption decreased from pre- to post-FBT [t(173) = −4.90, p < 0.001], and SSB intake decreased as well [t(173) = −7.56, p < 0.001].
Associations between Baseline Social Support and Change in Dietary Intake and Weight
The interaction between time and pre-FBT family encouragement was significant for change in healthy vegetable intake and change in weight. Children who started with high family encouragement had less increase in healthy vegetable intake [Wilks' Lambda = 0.97, F(1, 171) = 4.92, p < 0.05] and less decrease in BMI z score [Wilks' Lambda = 0.98, F(1, 171) = 4.10, p < 0.05] compared with those who started off with low family encouragement. See Figure 1 for a graph of pre- and post-FBT healthy vegetable servings and weight for children with low and high pre-FBT family encouragement of healthy eating (defined using a median split). Dietary and weight change models with family discouragement were nonsignificant.

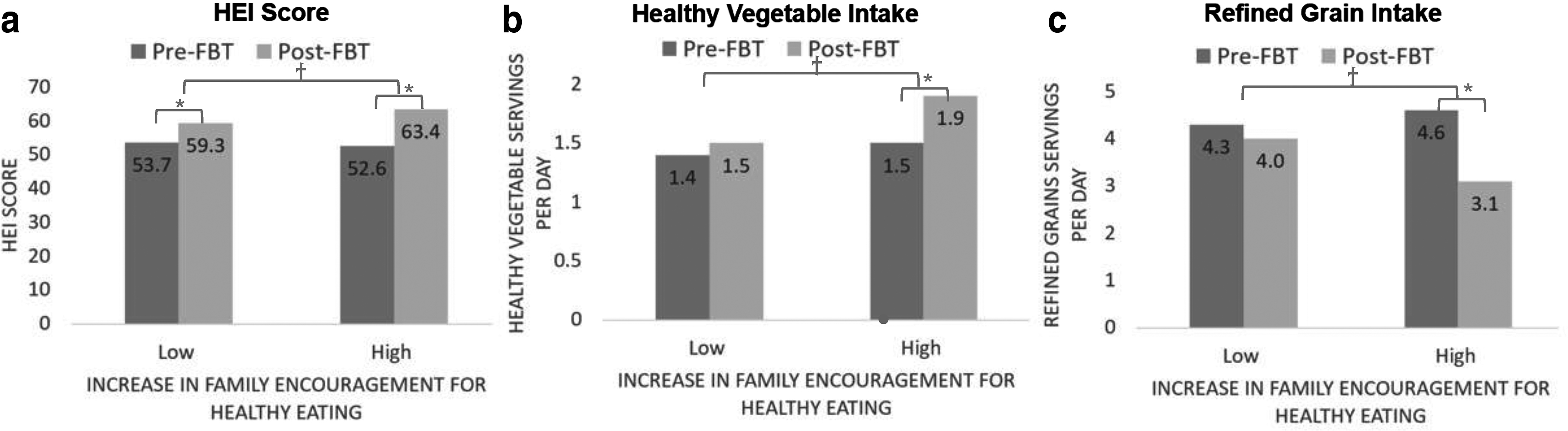
Associations between Change in Social Support and Change in Dietary Intake and Weight
The interaction between time and family encouragement for healthy eating was significant for HEI-2015 [Wilks' Lambda = 0.96, F(1, 168) = 7.31, p < 0.01], healthy vegetables [Wilks' Lambda = 0.96, F(1, 168) = 7.87, p < 0.01], and refined grains [Wilks' Lambda = 0.91, F(1, 168) = 16.45, p < 0.001]. Post hoc analyses demonstrated that children who had a greater increase in family encouragement for healthy eating from pre- to post-FBT had greater increases in HEI-2015 scores and healthy vegetable intake, as well as greater decreases in consumption of refined grains (Fig. 2). There were no significant interactions between time and family discouragement of healthy eating for any diet or weight variables or between time and family encouragement of healthy eating for weight change.
Discussion
The objective of the present study was to explore the relationship between family support and child dietary intake and weight change during FBT. From pre- to post-FBT, family encouragement for healthy eating increased significantly, and as hypothesized, increases in family encouragement for healthy eating were related to increases in overall child diet quality. In FBT, parents are active participants in treatment who learn parenting strategies to encourage their child's healthy eating (e.g., praise). Our findings align with previous research that also demonstrated the positive impact of parenting techniques on child dietary intake during weight management interventions.30,31 Overall, results emphasize that the FBT components that work to increase family encouragement for healthy eating are important for improving child diet.
Notably, children that began FBT with low encouragement for healthy eating still experienced improvements in diet quality and reductions in weight during treatment. Children with low pre-FBT family encouragement started the treatment with lower healthy vegetable intake but were able to increase their vegetable intake to about the same level post-FBT as children with high pre-FBT family encouragement for healthy eating. Children with low pre-FBT family encouragement also demonstrated greater reductions in BMI z score than children with high pre-FBT family encouragement. Finally, children with low pre-FBT family encouragement also had greater increases in family encouragement during FBT than did children with high pre-FBT family encouragement. This suggests that FBT can effectively improve child diet and weight status regardless of the child's level of family encouragement before intervention, and the parental support components of FBT may be particularly helpful for those with low baseline family support.
Unlike family encouragement, family discouragement of healthy eating did not change significantly during FBT (means of 9.9 ± 3.9 and 10.3 ± 4.4 for baseline and post-FBT, respectively, on a scale from 5 to 25). The finding that family discouragement began low and did not change in FBT is consistent with a previous trial. 32 One explanation for this finding is that FBT did not specifically focus on family discouragement of healthy eating as the treatment primarily targets increasing family encouragement (e.g., giving praise, modeling healthy behavior) vs. reducing family discouragement (e.g., teaching targeted conflict resolution strategies for family disputes regarding food choice). However, FBT does address reducing family discouragement to some extent. For example, the treatment teaches parents to avoid modeling unhealthy eating behaviors and bringing unhealthy foods in the home. Another possible explanation is that because the average family discouragement scores are close to the lower range of possible scores, the lack of change in family discouragement represents a floor effect. Interestingly, changes in child eating behaviors were not related to baseline or change in family discouragement for healthy eating. These results suggest that improvements in child dietary outcomes are associated with the presence of encouragement and not the lack of discouragement. The power of family encouragement such as praise and active guidance in improving child diet is consistent with previous literature.14,33,34
There are limitations to this study that warrant discussion. First, given that all participants received the same treatment, there was no comparison group with which to examine whether the changes in social support and diet resulted from FBT as opposed to other factors, such as the passage of time. However, the repeated-measures design strengthens our conclusions, and it is unlikely that family support for healthy eating behaviors among children in our study would have improved without the targeted FBT intervention, especially in this relatively short time period (16 weeks). In addition, while conclusions of causal inference cannot be made between social support and dietary intake, the examination of social support's impact on changes in diet quality bolsters the findings, as most of the literature regarding social support and youth dietary intake is cross sectional. 14 It also may be more likely that children who begin treatment with lower social support have greater increases in social support across treatment because they have greater capacity to increase social support than do children with already higher social support; however, the findings related to changes in social support, as they relate to changes in diet, are still robust.
Moreover, given the demographics of the current sample, research with more racially, ethnically, and socioeconomically diverse samples is needed before determining the generalizability of these findings. Finally, while the validated measure of family support in this study allowed examination of different types of family support (i.e., encouragement vs. discouragement), the measure did not allow examination of within-family influences. For example, a child may have a supportive parent and an unsupportive sibling, but these family members are not considered separately in the measure. Therefore, there is a need for the development of measures of social support that can account for the potential variability in support from different family members that can help clinicians better tailor interventions.
Despite these limitations, the present study has several strengths and addresses multiple gaps in the literature regarding social support and child eating behaviors. This study critically evaluated social support in the context of a weight management intervention, which is limited in the existing literature, 35 and the findings may be used to inform treatment. For example, because family encouragement for healthy eating was related to eating behavior changes and family discouragement for healthy eating was not, treatments should work to increase the positive parenting strategies rather than decrease the negative strategies. In addition, while previous research has explored the impact of family support on weight outcomes in FBT,9,22 this study is the first to examine the impact of baseline family support and changes in family support on changes in eating behaviors during FBT.
In conclusion, this study reinforces the idea that family social support, particularly encouragement for healthy eating, influences child dietary changes during FBT. More work is needed to understand the relative impact of other social influences, such as peer support, on FBT outcomes. Also, although we did not find parent- and household-related variables to be significant covariates in this research, it is possible that more nuanced measures, such as household size or adjusting income based on median income for each family's zip code, may relate to family support during treatment, and future research could explore this. Finally, as this study only examined short-term treatment outcomes, future studies should investigate the impact of family encouragement on long-term treatment outcomes. Specifically, future research is needed to determine if parents maintain the increased family encouragement and whether or not the positive effects of family encouragement persist. Given the strong association found between positive family support and child eating habits, interventions should work to optimize and maintain family support to promote behavior change for children with overweight and obesity.
Clinical Trials Registration
Childhood Obesity Treatment: A Maintenance Approach (COMPASS), ClinicalTrials.gov Identifier: NCT00759746.
Footnotes
Funding Information
This work was supported by the Eunice Kennedy Shriver National Institute of Child Health and Human Development (R01 HD036904) and the National Heart, Lung, and Blood Institute (T32 HL130357).
Author Disclosure Statement
No competing financial interests exist.