
Abstract
Background:
Childhood obesity, due to its increasing prevalence, is one of the most challenging problems in public health and prevention. Recent strategies have been implemented to tackle this trend, including school gardening projects. This systematic review analyzes the main elements of school gardening with a specific meta-analysis about its impact on anthropometric parameters.
Materials and Methods:
We searched studies in PubMed, EMBASE, and Cochrane Library on school gardening projects carried out until February 2019 and addressed to children aged 6 to 13 years.
Results:
Thirty-three studies passed the screening selection. Outcomes analyzed were fruits and vegetables consumption/knowledge, nutritional attitudes and behavior, anthropometric outcomes (i.e., BMI, waist circumference—WC) and other outcomes (i.e., blood pressure, science achievement, and physical activity). We performed descriptive analyses of these outcomes and found a general benefit from school gardening projects. We subsequently performed a meta-analysis on anthropometric outcomes, highlighting a significant reduction of both BMI percentile (%) (−1.37%) and WC (−1.30 cm).
Conclusions:
Although more high-quality studies are needed on this topic, along with a greater homogeneity of anthropometric measurements, the results of our article show a modest but positive impact of school gardening projects on anthropometric measures and more generally on children's health.
Introduction
Childhood obesity is a public health priority and its prevalence and economic burden have been steadily increasing worldwide.1,2 The prevalence of childhood obesity ranges between 21% and 24%, affecting about 43 million children.3,4 Evidence shows that childhood obesity is strongly associated with adult obesity and that it is the best predictor of morbidity and mortality in adulthood.5,6 Furthermore, overweight and obese children can experience discrimination, alongside with higher levels of psychological and physical abuse by schoolmates, compared to other children. 7
Public institutions have developed and implemented several strategies to prevent obesity in children, including programs aimed at promoting healthy eating habits through the increase of fruit and vegetable (F/V) intake, improvement of food education, and involvement in gardening activities. 8 Studies have shown that children who learn healthy eating habits at a young age have a higher likelihood to maintain these habits through their life, compared to interventions carried out in adulthood. 9 Other studies reported that family involvement is a key factor for children's eating habit improvement, and school can be a favorable environment to engage children and families. 10 Recent evidence showed that multicomponent programs, including diet and educational activities, are more effective than programs exclusively focused on diet in changing children's eating attitudes. These approaches combine nutritional education programs, possibly with information on seasonality and local agricultural products, school gardening, and promotion of physical activity.11–13
BMI, expressed as weight/height2 (kg/m2), and waist circumference (WC), measured in centimeters, are commonly used to measure anthropometric characteristics and stratify the risk for overweight and obesity in adults and children. 14 BMI and WC are easily obtainable and have proved to be strong predictors of metabolic syndrome, type 2 diabetes, and cardiovascular disease in adults and children.15,16 Yet, the impact of school gardening interventions on anthropometric parameters, which have shown to predict morbidity and mortality in adulthood, has been poorly studied. Previous literature reviews about this topic focused on different outcomes related only to nutritional behavior, dietary intake, and academic achievement. On the contrary, this is the first study focused on covering the gap in knowledge in the scientific literature regarding changes in anthropometric outcomes related to school gardening programs.
We undertook a systematic review (SR) on the impact of school gardening projects on school-aged (6–13 years) children's data about F/V intake and knowledge; science achievement; physical activity levels; blood pressure; and markers in blood samples. We systematically reviewed and meta-analyzed the impact of school gardening projects on school-aged (6–13 years) children's anthropometric parameters, gathering information from experimental studies on BMI and WC changes in after-school gardening interventions. This work can provide clinicians and policy makers with robust evidence on the efficacy of tools aimed at increasing children's knowledge and engagement in practical/educational activities, and ultimately improving their knowledge about healthy habits and lifestyle, and health outcomes.
Materials and Methods
Search Strategy
Databases and search criteria
We performed a systematic search and review according to PRISMA guidelines. 17 We searched primary (PubMed, EMBASE™) and secondary (Cochrane Library) electronic databases to identify relevant studies for the period between January 1946 and February 2019. We developed a specifically designed search string for this purpose: [(school garden* OR school gardening) AND (obes* or overweig* OR obesity OR overweight)]. We searched gray literature for other documents and performed a hand search of key journals, professional organizations' websites and guideline clearing houses. Moreover, we scanned reference lists of selected articles to find additional articles. We applied snowball (such as pursuing references of references and electronic citation tracking) and hand search techniques (such as scanning reference lists of selected reviews, primary articles and textbooks, and scanning for other documents in selected journals and guideline clearing houses) to the search strategy previously described. 18
Patients, interventions, comparators, and outcomes question
The following patients, interventions, comparators, and outcomes (PICO) question addressed our primary search objective through the following search terms: (P) children attending school, aged 6–13 years, (I) school gardening projects for obesity prevention, (C) only nutritional education or no intervention, and (O) postintervention anthropometric measures, F/V knowledge, F/V consumption, and other outcomes such as blood pressure, science achievement, physical activity levels, and blood samples about metabolic syndrome markers.
Study Selection
Design
We included randomized controlled trials (RCTs), quasi-experimental, and observational studies whose primary intervention consisted in school gardening projects for primary school students (age range between 6 and 13 years). We excluded studies about preschool-aged children and adolescents. We included any outcome concerning anthropometric measurements, F/V consumption or knowledge and other outcomes such as blood pressure, science achievement, physical activity, and blood samples about metabolic syndrome markers. We excluded protocols as well as systematic or narrative reviews. We included in the meta-analysis only RCTs and quasi-experimental studies.
Data selection and extraction
Two reviewers (A.R. and D.G.) independently identified potentially eligible studies from title and abstract reading. The same authors assessed full texts of relevant studies included and consulted the references of the previously published primary and secondary articles to search for additional relevant articles. We resolved any disagreement through discussion and reaching a consensus between the two readers. When we did not reach any consensus, we requested an opinion of a third author (A.U.), which acted as an “in blind” final arbiter.
We used the same methodology for data extraction performed independently by two reviewers (A.R., D.G.), with the supervision of a third author (D.T.). We analyzed data using Microsoft Office Excel 2013 (Microsoft Corporation) and Stata (StataCorp. 2013. Stata Statistical Software: Release 13. College Station, TX: StataCorp LP).
Interventions
We included school gardening projects that involved gardening activities (with/without a nutritional education program). We excluded projects only based on theoretical lessons or on other activities that did not include school gardening. We considered interventions performed during school hours, after-school hours, or during summer school camps. We included any type of intervention addressed to scholars and those carried out in different school groups and with different components. We excluded interventions developed only in community gardens settings (i.e., addressed to the whole community) without a specific involvement of the schools.
Study Quality Assessment
We used the Cochrane Tool for Quality Assessment and the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) to assess study quality of the experimental and observational original studies included in this SR.
The Cochrane Tool allows analyzing seven bias groups: sequence generation and allocation concealment (both within the domain of selection bias or allocation bias), blinding of participants and personnel (performance bias), blinding of outcome assessors (detection bias), incomplete outcome data (attrition bias), selective reporting (reporting bias), and an auxiliary domain, “other bias.” 19 For each bias group, it is possible to assign a value of “high,” “low,” or “unclear” risk of bias when it is not specified if a specific bias is present or not. Every bias judgment helps to assign a global assessment to every RCT according to the Agency for Health care Research and Quality (AHRQ) standards (good, fair, and poor). 20
The STROBE statement is a 22 items tool specifically designed to evaluate observational studies quality. 21 Items are associated with the different sections of an article, such as title and abstract (item 1), introduction (items 2 and 3), methods (items 4–12), results (items 13–17), discussion (items 18–21), and other information (item 22 on funding). Eighteen items are identical for the three different study designs, while four (specifically items 6, 12, 14, and 15) are differentially designed for each study type (i.e., cohort or case control).
STROBE does not provide a scoring stratification. As a general rule, the higher the score, the higher the quality of the study. We hence created three score thresholds corresponding to three levels of quality: 0–14 as poor quality, 15–25 as intermediate quality, and 26–33 as good quality of the study.
Statistical Analysis
We described the main descriptive characteristics of the studies in the SR, focusing on the following key-points: country, study design, type, duration and time of intervention, and outcomes. Subsequently, we performed a meta-analysis on the anthropometric measures that were analyzed by the included studies: BMI, BMI percentile (BMI%), BMI z-score, WC, and diastolic and systolic blood pressure. We decided not to analyze quantitatively F/V intake or knowledge or school/academic performances since we found very heterogeneous and inconsistent measurements. We compared values between intervention and control groups in those studies, which investigated these parameters both pre- and postintervention.
We analyzed statistical heterogeneity to define if it was feasible to sum the results of the different studies considered eligible for the meta-analysis. We studied heterogeneity by the used graphic funnel plots and by calculating the I2 statistic, which represents the percentage of the variance in effect estimates that is caused by heterogeneity rather than by sampling bias (chance). An I2 statistic greater than 50% was considered significantly heterogeneous.
Where the number of studies was less than five or studies were substantially heterogeneous, we utilized a random-effects model in accordance with the Cochrane Handbook for Systematic Reviews of Interventions. 22 We followed the method of DerSimonian and Laird to compute the random-effects estimates for the corresponding statistics. 23 If standard deviation was available for all the studies, we calculated the standard error and the variance for the meta-analysis. We chose to use the forest plots to show graphically effect estimates with 95% confidence intervals (CIs) for individual trials and pooled results. We carried out meta-analyses using Cochrane's RevMan (Version 5.3. Copenhagen: The Nordic Cochrane Centre, The Cochrane Collaboration, 2014).
Results
Search Findings
Our search yielded 203 studies (133 by databases browsing, 4 by hand search, and 66 from other SR bibliography), 33 of which were appropriate for review,24–56 and 5 for meta-analysis.26,27,29–31 We excluded 140 studies, which did not meet the eligibility criteria or were duplicated. Figure 1 shows the flowchart with the study selection process.
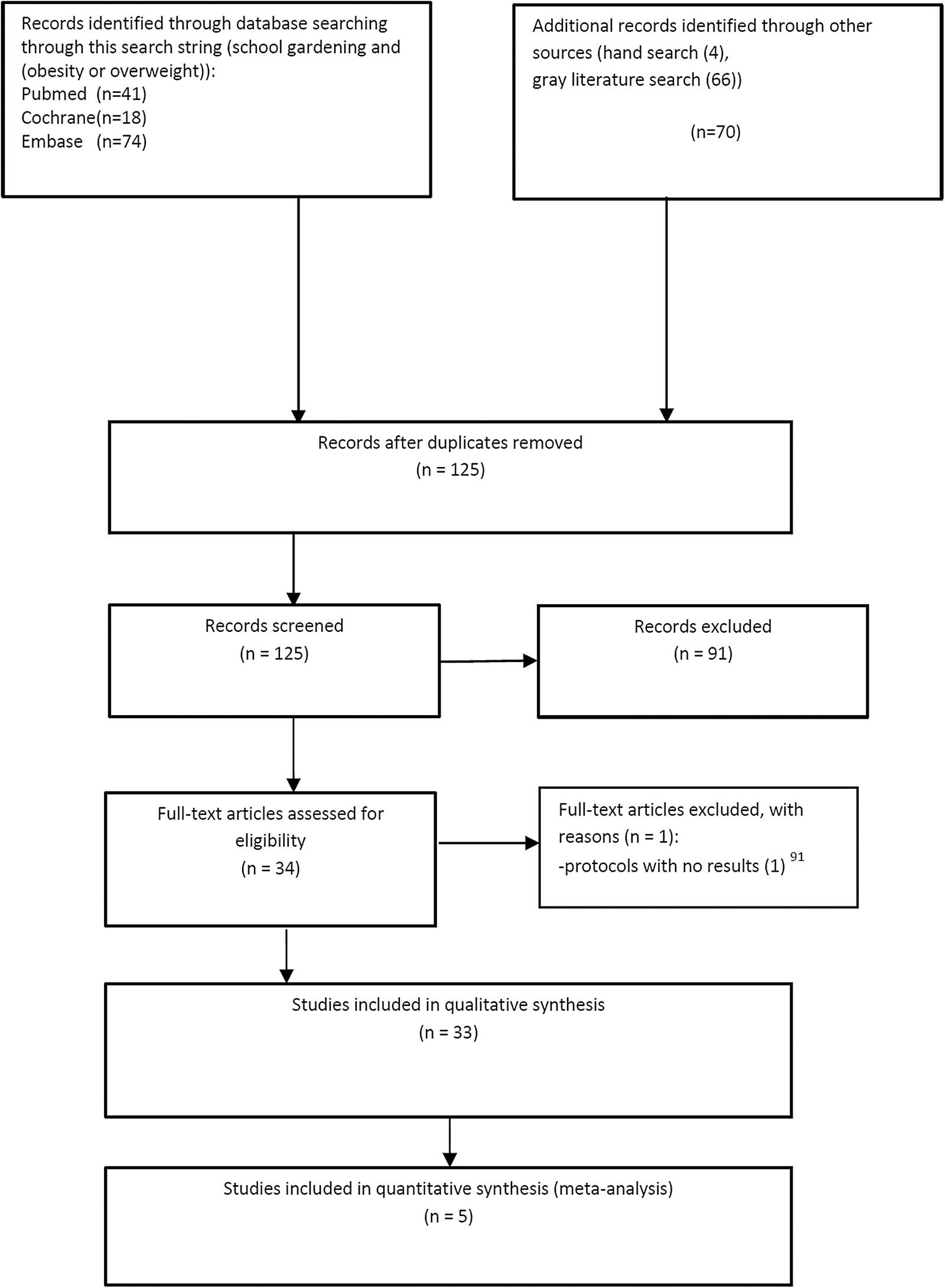
PRISMA flow diagram, which shows the process for studies selection. Flowchart designed according to: Moher et al. 17
Characteristics of the Included Studies
The geographic origin of the studies was United States (n = 25, 75.8%),24–27,30–34,36–39,41,44–46,48–51,53–56 Australia (n = 3, 9.1%),35,42,52 United Kingdom (n = 2, 6.1%),28,40 Portugal (n = 1, 3%), 29 Netherlands (n = 1, 3%), 47 and Canada (n = 1, 3%). 43 Time interval for the school gardening program ranged between 2.5 months 35 and 2 school years.31,53
The intervention sessions lasted approximately an hour each week, with the shortest length reported of 20 minutes44,45 and the longest of 3 hours for week. 35 Sample sizes were heterogeneous and ranged between two classrooms (about 30 students) 38 and multiple campus schools (about 3000 students). 31
The interventions took place in different settings and timings: school hours (n = 25; 75.8%),24–26,28,29,31–36,39,40,42,43,47–56 after-school (n = 5; 15%),27,30,37,38,45 summer school camps (n = 2; 6.1%),44,46 and either during school hours or after-school (n = 1; 3.1%). 41 Twenty-seven (81.8%)24–28,30–34,37,39–48,50,52–56 school interventions were designed for a single group of students, while in the remaining six studies (18.2%) 29,35,36,38,49,51 the students were divided in two groups: one implementing theoretical lessons only and one with an intervention including both theoretical lessons and practical gardening activities.
Four studies26,31,41,53 described multicomponent interventions which integrated nutritional lessons and school gardening practice with other activities such as physical activity promotion, cooking class workshops, school menus implementation with healthy foods, and educational farms guided tours with the classes. In two studies, due to different schools facilities, not all students included in the educational programs were exposed to the intervention components in the same way.41,53 We included in the SR: 6 RCTs (18.2%),24–29 17 observational studies (51.5%),40–56 and 10 quasi-experimental studies (30.3%).30–39
Also of note, in two studies authors adopted the same study design, but reported different outcome results in each study.24,25 Twenty-three studies (69.7%) had a control group,24–27,29–37,39–42,47,49,51,52,55,56 while 10 studies (30.3%) did not.28,38,43–46,48,50,53,54 In one study, the two intervention groups had the same components, but were carried out by different staff members (university staff vs. school teachers). 28
Only four studies monitored research outcomes after the intervention, with a follow-up period of 1 month, 35 6 months,28,36 and 1 year, 47 respectively. One quasi-experimental study, conducted by Hollar et al., consisted of two cohorts in two different school years. 31 Therefore, we carried out the analyses considering school years separately. In the latter study, the authors investigated outcomes on the whole cohort study and a subgroup of low-income children accessing free/reduced price meals. Authors of a similar study analyzed subgroups containing overweight/obese children, and the pre–post intervention analyses were conducted both on the entire sample and on the subgroup. 30
Characteristics of the Outcomes Assessed
We found outcomes related to three main categories: F/V consumption/knowledge and nutritional behavior in 27 studies out of 33 (81.8%),24,26–28,30,32,34–54 anthropometric measures in 6 studies out of 33 (18.2%),26,27,29–31,40 and other outcome measures (i.e., physical activity, academic performance, blood pressure, and laboratory assessments like glucose, cholesterol, and triglycerides) in 11 studies out of 33 (33.3%).25–27,29–31,33,35,45,55,56 Out of 33 studies, 8 studies (24.2%) analyzed more than a single outcome category.
F/V-Related Outcomes
The outcomes related to F/V dietary habits were the following: F/V consumption, F/V knowledge, F/V dietary attitudes and behavior, and F/V home availability. In six study protocols, parents' collaboration was required to assist children to complete home food diary 28 or to fill out questionnaires about family demographic and family nutritional choices.26,34,42,44,53 Five studies focused on outcomes related to vegetables only (i.e., vegetable knowledge or intake) in school gardening implementation projects.32,39,45,47,54
F/V Intake
Twenty studies analyzed F/V consumption through different methods: questionnaires (n = 12; 60%),26,27,30,34,37–43,45 food diary measuring food habits (compiled at home and/or at school: n = 5; 25%),28,35,48,49,53 and direct observation in the lunchrooms (n = 3; 15%).32,51,54 In six schools, during the intervention, lunchroom menus were implemented with locally produced salads or vegetables or either vegetables harvested in school gardens.26,32,39,41,51,54 Five studies observed a positive impact of school gardening on combined F/V intake.34,40,41,49,53 Five studies measured an increased vegetable consumption,32,39,45,51,54 while one study observed a reduction of vegetable consumption in the intervention group although the reduction was stronger in the control group. 27 Three studies27,30,49 showed an increase of fiber intake. Furthermore, one study found an increase of vitamin A and vitamin C intake through the results of F/V food diary. 49 Finally, in one study, the parental questionnaire analyses showed a positive significant relationship between the implementation of the intervention and the amount of F/V cooked at home. 34
F/V Knowledge
Seventeen studies examined F/V knowledge. Questionnaires assessed children's knowledge of basic nutritional principles26,28,34–38,41,43,46,47,50,51,53 or capacity for F/V identification26,39,47,52 or capacity to describe food. 42 Furthermore in two studies, questions concerned knowledge of locally grown F/V.41,52 In 13 studies, the authors reported a knowledge increase26,28,35,36,39,41,43,46,47,50–53 in the intervention vs. the control group after the implementation of gardening projects, while the remaining studies did not show significant differences among groups.
F/V Dietary Attitudes and Behaviors
Twenty studies analyzed F/V dietary attitudes and behaviors related to intentions, attitudes, norms, and perceived behavioral control. Outcomes were related to general nutrition and F/V consumption,40,44,46,47,52,53 F/V preferences,26,35–39,41,43,44,46–48,50,51,53 “willingness to try new F/V,”28,34,35,39,42,51,52 and gardening self-efficacy.37,41,44,52 The nutritional behavioral attitudes had a positive impact in two studies.40,44 Four studies found a significant improvement in “willingness to try new F/V” outcomes in the intervention group34,35,39,42 while other two studies showed a negative association, but only related to new type of fruit consumption.28,52 F/V preference increased after intervention in two studies,50,51 while preference for only vegetables increased in six studies35,36,39,44,47,48 and preference for only fruit in a single study. 43
In five studies, an improved self-reported preference for healthy F/V-based snacks instead of unhealthy foods was found.34,35,48,50,52 In one study, gardening self-efficacy was found significantly different in intervention vs. control group. 41 Two studies researched F/V home availability,24,44 but only one study observed an increase in F/V presence at home, especially for low-fat vegetables. 24
Anthropometric Outcomes
Studies that included analyzing anthropometric outcomes used nine different anthropometric measures: absolute BMI, BMI%, BMI z-score, weight z-score, weight, waist to height ratio, WC, body fat %, and height. Five out of six studies (83.3%) used multiple anthropometric measurements. A significant absolute BMI reduction was found in one study, 30 although the authors observed a change in measure in the overweight/obese subgroup only. Hollar et al. 31 found a significant BMI% reduction in the second year of follow-up only, while at the first year, it was not significant. In the latter study, a significant BMI z-score and weight z-score reduction related to the low-income children subgroup was found. The results of other two studies showed a significant reduction in BMI z-score: in one study, the BMI z-score reduction was associated with a WC reduction, 27 while in the second study, the BMI z-score improvement was associated with a BMI% and waist to height ratio reduction. 26
Other Outcomes
Other outcome measures considered in the studies were physical activity (n = 2; 18.2%), measured by questionnaires,25,45 direct observation and use of accelerometers, 25 skills in school subjects (n = 5; 50%), including science,26,33,55,56 math,31,55 and reading, 31 and other laboratory measures (n = 4; 40%),27,29–31 that is, glucose, triglycerides, total cholesterol, high-density lipoprotein, and low-density lipoprotein, insulin (fasting blood samples), blood pressure, Homeostatic Model Assessment of Insulin Resistance (HOMA index), urinary sodium, and urinary creatinine. Finally, in one study 29 authors estimated salt intake from 24-hours urinary sodium excretion, while other authors measured the quality of school life, through a survey about student attitudes toward school, learning, and teachers and about other students' relationships. 35
Physical activity increased in the intervention groups in both studies that analyzed it.25,45 Two studies found an increase in science achievement scores,33,56 while math scores improved in another study, 31 specifically in the low-income children subgroup. In one last study, math skills upgraded in the control group compared to intervention group. 55 Two studies observed a significant reduction of blood pressure,30,31 while other laboratory measures (i.e., blood and urinary samples) showed no significant results in two studies.27,29 Authors observed reduced salt intake after intervention, 29 while quality of school life showed no significant changes. 35 Table 1 shows the characteristics of the studies included in this SR, classified according to the three main outcomes explained in the text.
Characteristics of the Included Studies
BMI%, BMI percentile; CTR, control; F/V, fruits and vegetables; HDL, high-density lipoprotein; INT, intervention; LDL, low-density lipoprotein; n/a, not available; RCT, randomized controlled trial; WC, waist circumference.
Quality Assessment
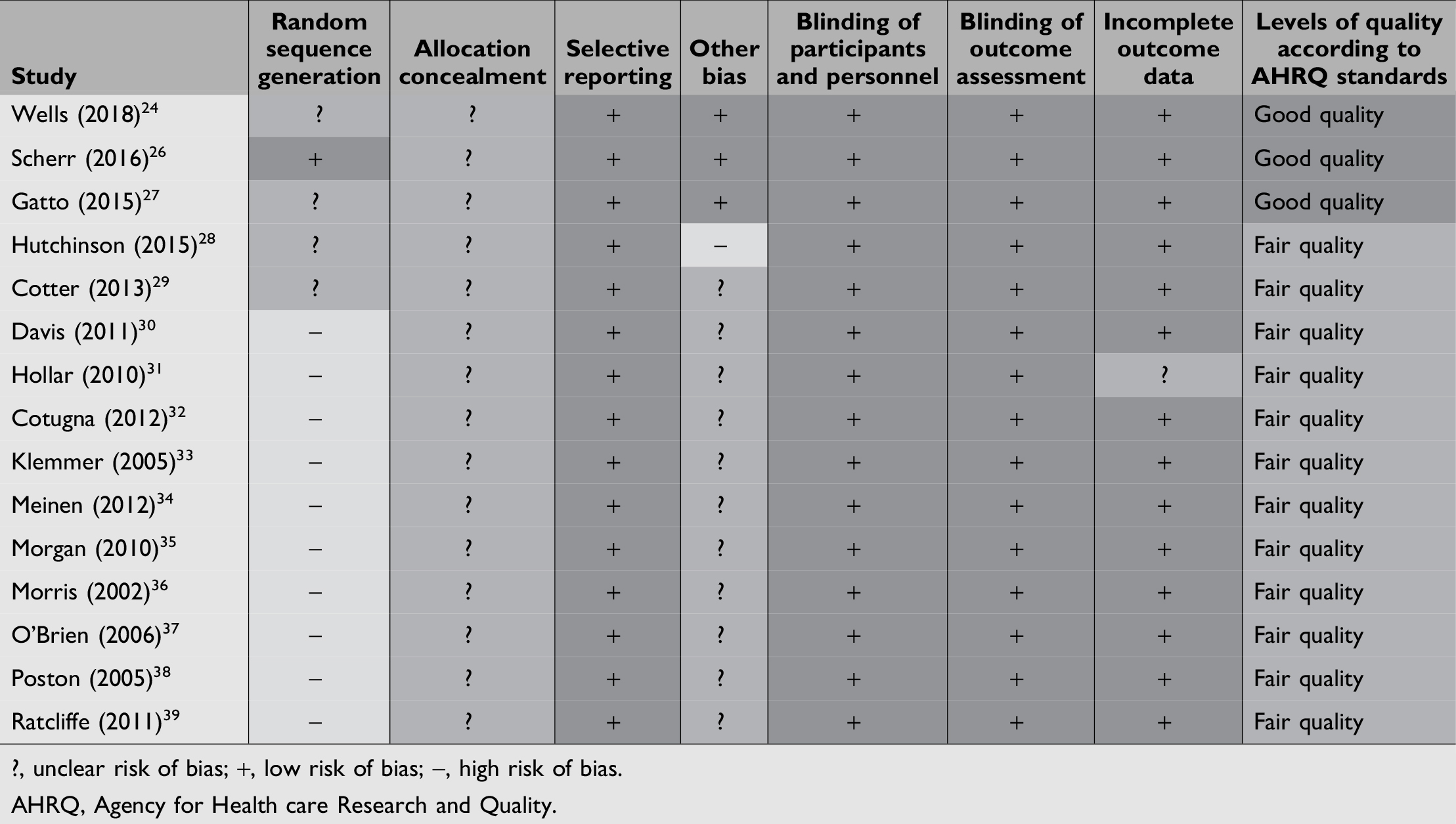
As previously explained above, we analyzed for quality the two RCTs24,25 which shared the same study design as one. We used the Cochrane Tool for Quality Assessment to assess 15 studies24,26–39 (5 RCTs24,26–29 and 10 quasi-experimental30–39 ): 3 scored good quality,24,26,27 while 12 scored fair quality (details are shown in Table 2).28–39 About those rated as fair quality, one RCT had a high risk of bias due to the control group's features (identical activities into the intervention group, only carried out by different staff members), 28 while all the quasi-experimental studies had a high risk of bias due to absence of randomization.30–39 Specifically in the latter studies, due to their study design, there was a potential risk of bias (marked in yellow under “other bias” in Table 2). In addition, in the study by Hollar et al. 31 the outcome data related to blood pressure was not shown point-by-point and there was a graph without clear numerical references. In all the studies, there were no detailed information on allocation concealment; thus representing unclear risk of selection bias for all of the studies analyzed. Similarly, in four out of five RCTs analyzed,24,27–29 random sequence generation details were not explained. For this reason, we assessed an unclear risk of selection bias. Finally, for one RCT, 29 we assessed a potential risk of bias because of the small sample size together with a difficulties in the achievement of 24 hours urine collection in a pediatric population.
Quality Assessment of Randomized Controlled Trials and Quasi-Experimental Studies
Using the STROBE tool, we rated 17 observational studies,40–56 4 of which scored intermediate quality45,46,48,54 and the remaining 13 scored good quality.40–44,47,49–53,55,56 The main critical issues assessed in these studies were small sample size, absence of eligibility criteria for study participants inclusion, unspecified/unclear follow-up period, unclear intervention type outcome, and lack of a control group.
Assessed Outcomes and Evidence Synthesis
Anthropometric measures
The meta-analysis of two studies29,30 showed a 0.13 (95% CI: −0.94 to 1.20) nonsignificant increase (random model I2 = 0%) of absolute BMI measure in the intervention group compared to control group (Fig. 2A). The meta-analysis of 4 studies26,27,30,31 showed a 0.09 (95% CI: −0.19 to 0.01) nonsignificant decrease (random model I2 = 78%) of BMI z-scores in the intervention group compared to control group (Fig. 2B). The meta-analysis of 4 studies26,27,30,31 showed a 1.37 (95% CI: −2.38 to −0.37) significant decrease (random model I2 = 41%) of BMI% in the intervention group compared to control group (Fig. 3A). The meta-analysis of three studies27,29,30 showed a 1.30 cm (95% CI: −1.43 to −1.16) significant decrease (random model I2 = 0%) of WC in the intervention group compared to control group (Fig. 3B).

Impact of school gardening and control on BMI
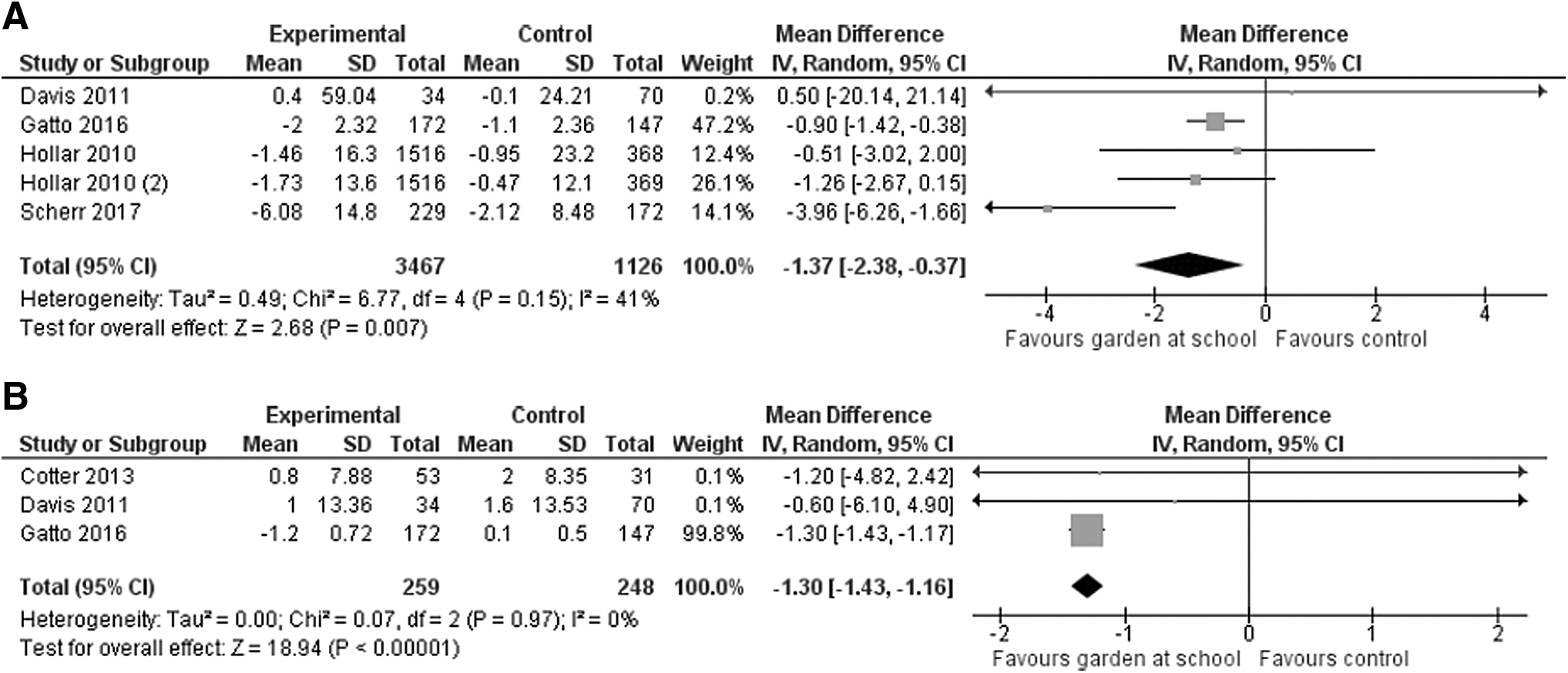
Impact of school gardening and control on BMI%
Blood pressure
Between pre- and posttest comparisons, the meta-analysis of three studies27,29,30 found a 1.91 mmHg (95% CI: −0.78 to 4.59) increase of diastolic values (random model I2 = 73%) and a 0.58 mmHg (95% CI: −1.68 to 2.85) increase of systolic values (random model I2 = 45%), both nonstatistically significant (Fig. 4A, B).

Impact of school gardening and control on diastolic blood pressure
Discussion
This is the first SR and meta-analysis analyzing the impact of school gardening on anthropometric variables in school-aged children, along with other outcomes related to knowledge, attitudes, and other laboratory and clinical outcomes. Our study updates nonanthropometric outcomes, confirming a general improvement in outcomes related to the three main categories analyzed related to F/V, namely F/V consumption, knowledge, and nutritional behavior. With different degrees of evidence, we found a positive impact of school gardening projects on all of these outcomes. In particular, the selected articles demonstrate that children increased F/V daily/weekly intake34,40,41,53 and improved their F/V knowledge.26,28,35,36,39,41,43,46,47,50–53 Moreover, the selected articles found a positive impact on nutritional behavioral attitudes, with a significant improvement in “willingness to try new fruits and vegetables” outcomes.34,35,39,42 Other studies34,35,48,50,52 also showed that school gardening projects improved both F/V preference and self-reported preference for healthy F/V-based snacks. The abovementioned results are in accordance with previous secondary studies' results for these outcomes57–64 and highlight their paramount importance in the obesity prevention field.
Gardening activities have the common purpose of improving children's knowledge about the natural world. 63 Developing this skill from childhood can establish an environmental responsibility and awareness about wellbeing and quality of life, as long-term effects also in adulthood. 63 Regarding F/V intake, some studies showed an increase of combined vegetables and fruit intake or of vegetables alone intake. There was no study which reported an increase in the fruit intake only. Similar results were found for willingness to try new F/V. We hypothesized that this has been caused by studies, which were designed to measure vegetable intake only32,39,45,47,54 or because school gardens often contain mostly vegetables (which are much more easy to cultivate). This peculiarity has been reported also in other secondary studies.57–60,63
Among those, one study, 60 to explain the potential relationship among school garden, vegetable intake, and willingness to try new F/V, has assumed that gardening activities has the potential to bring the children closer to the vegetables and, at the same, to reduce their unwillingness to try new foods. Another review 64 demonstrated that an increased willingness to taste F/V in children attending kindergarten and first grade can result into a greater fruit and vegetables preference and intake also in older ages. This result is crucial for obesity prevention. School gardening activities, nutritional education, and healthy meals offered in the lunchrooms can give the opportunity for children to improve the quality of their diet and nutrient intake. 58 This last consideration could also explain the increased self-efficacy observed in one study 41 we included in this SR.
As far as the organizational structure of the school garden programs are concerned, among the studies that reported two types of intervention29,35,36,38,49,51 (gardening + nutritional education vs. nutritional education only), four out of six showed significant better result in the group which undergo a double intervention compared to the control group.35,36,49,51 These conclusions are in accordance with the literature which supports the strength of the school garden combined with nutrition education to achieve some outcomes related to obesity prevention (particularly vegetable intake).60,65
In addition, we analyzed four different multicomponent programs,26,31,41,53 and in two of them,41,53 we found significant differences in terms of F/V outcomes between schools providing full-program components and other schools which offered partial programs. A secondary study 57 highlighted that multicomponent interventions have higher impact on change in nutrition-related behaviors than a single component intervention. Multicomponent interventions usually consist in the development of a series of interventions, in which families can find a strict involvement of the family (which has a crucial role in the obesity prevention 59 ), introduction of healthy foods in the school lunchrooms, which increases the quality of diet and different food options, 58 and finally, the implementation of food laboratories. Food workshops as well as active gardening activities (i.e., planting, cultivation and harvesting processes), are an example of “hands on” learning experience, 59 making children play an active role in the learning process, rather than being passively involved. 59
Other outcomes, such as blood pressure or laboratory outcomes, showed mixed and inconsistent results with the exception of academic achievement31,33,56 and physical activity level.25,45 Positive improvement for academic performance covered only science33,56 and math 31 subjects, while reading 31 did not reach any statistical difference between intervention and control groups. In fact, other studies demonstrated a positive impact of school gardening on children's social development 58 and in other academic achievements. 64 This can be assumed by the demonstrated improvement of both observational skills of the children and interdisciplinary content of the school programs, 58 encouraging academic learning in the scientific area.61,62 Furthermore, as demonstrated in the previous results, natural green areas have also the opportunity to increase the amount of physical activity carried out by children. 66
This is the first SR and meta-analysis studying the impact of school gardening on anthropometric variables in school-aged children. Our study shows a statistically significant reduction of WC and BMI% comparing pre- and postintervention. We found no significant differences in other anthropometric outcomes investigated, including blood pressure. The pooled analysis showed a 1.3 cm significant reduction of WC and a 1.37 reduction of BMI%. The use of WC and waist–hip ratio as anthropometric indicators has been analyzed in a previous WHO report. 67 The working group states that anthropometric parameters (i.e., BMI, WC, and waist–hip ratio) can well estimate the risk of chronic disease. Therefore, WC and waist–hip ratio, regardless of cutoff points developed, could be utilized alone or in association with BMI. In addition, experts recommend, during the cutoff points development for WC and waist–hip ratio, to adopt a statistical approach based on policy relevance methodology with a final clear explanation of the decision rules. 67 This confirms that there is no consensus in the scientific community on cutoffs defining a clinically significant WC decrease, particularly for the pediatric population.
Due to the preventive nature of the intervention, our study included both children with normal and abnormal BMI. Therefore, we considered pre–post intervention nonincreasing or slightly reduced BMI values as a positive result. Furthermore, for more clarity, anthropometric variables should be stratified according to baseline values, as described by Davis et al. 30 Although it is still not clear if gardening activities have a strong impact on children's health, using a conservative approach, we may consider any reduction in WC or BMI% as a positive impact, particularly if addressed to overweight and obese children. This is also particularly important in the contemporary population, in which anthropometric measures, including WC and BMI%, show increasing trends in the pediatric population.68–70 Finally, literature shows an impact, along with all the other anthropometric variables considered, also on metabolic syndrome of the children undergoing obesity prevention multicomponent programs. 71 Previous studies have shown that there are two main reasons to target childhood anthropometric outcomes. First, overweight and obese children and teens are, compared to normal BMI children, much more likely to develop overweight and obesity in adult age. Second, as adults it is more challenging to lose the excess weight, compared to childhood or teen age, once they become overweight or obese. Moreover, children who learn healthy eating habits at a young age have a higher likelihood to maintain these habits through their life, compared to interventions carried out in adulthood. 72 Furthermore, obese children today are experiencing diseases and health problems previously observed only in adults. The resulting complications of these diseases (i.e., type 2 diabetes, cardiovascular disease, hypertension, osteoporosis, and some carcinomas) can be a leading cause to a shorter life. 73
A possible criticism of similar interventions, as investigated by a recent SR 74 on interventions for preventing obesity in children, may be the potential impact of adverse or unintended consequences of the interventions. The study found no evidence of adverse outcomes, such as underweight, unhealthy eating practices, teasing, stigmatization, body image perceptions, satisfaction, or self-worth, although it acknowledged that only a minority of the included studies assessed adverse effects. Literature has previously shown that multicomponent interventions are effective in reducing the analyzed anthropometric variables.75–77 Interventions for childhood obesity prevention should include both diet and physical activity and be preferentially targeted toward school-aged children.65,74
In particular, for school-aged children, there is evidence of a positive effect of the interventions on anthropometric variables (i.e., BMI%, BMI z-score) in school settings. As highlighted by Katz et al., the 6 hours that school-aged children spend in school every day, for more than half the year, constitute a substantial part of their time and their lives.78,79 Therefore, it is important to consider school as one of the major drivers and elective settings for children education on healthy lifestyles.80,81 Recently, the programs for childhood obesity prevention have started to include activities and lessons focused on the importance of physical activity and on the dangers of sedentary lifestyle. In this context, some studies have shown a positive impact of the school and community gardens on outcomes such as blood pressure, BMI, and mental well-being. These studies showed also that outdoor activities improve the promotion of physical activity.82,83 In addition, strategies for overweight/obesity prevention, including gardening activities starting from childhood, could contribute to reduce health inequalities. Indeed, recent evidence highlights the association between low socioeconomic status and higher BMI in children aged 6–12 years.84,85 Three studies included in this review confirmed this evidence, showing that school gardening projects can improve health outcomes of low-income children who belong to families that may be unable to afford the cost of healthy food by increasing their access to healthy food in the school lunchrooms.27,30,31
This study has important strengths. First, we followed a robust methodology, based on the Cochrane guidelines and PRISMA methodology for SRs and meta-analysis. Second, we included in our qualitative analysis non-RCT studies to provide comprehensive data from all the available literature. Third, we assessed the risk of bias for the various studies. The results of this study must be also interpreted in light of important limitations. First, although the number of studies on school gardening has steadily increased in the last 10 years, it is still too low to draw conclusions on this topic.
We tried to address this lack of data by being as comprehensive as possible, carrying out hand-search and trying to find additional references and/or data in the gray literature. Second, the studies we analyzed had considerable heterogeneity, with particular regard to outcomes and measures. Unfortunately, anthropometric outcomes are measured in many different ways and use different units of measure. We tried to address this problem by considering all the potential outcomes (i.e., absolute BMI, BMI%, BMI z-score), and, whenever possible (i.e., more than one study with comparable outcome), we summed up the different data in different meta-analyses. Third, we observed that only a few studies (recent RCTs or quasi-experimental studies) analyzed anthropometric outcomes. School gardening has become an important topic in childhood obesity prevention only recently. We hypothesize that researchers have adopted anthropometric outcomes as more objective measures compared to traditional ones (i.e., F/V knowledge or F/V consumption). Fourth, we generally found mid/low-quality studies, particularly quasi-experimental and observational studies. More specifically, the majority of studies did not include long follow-up periods, therefore registering only short-term changes. Furthermore, F/V outcomes have been achieved mostly through self-reported measures (i.e., questionnaires and/or in a school/pediatric environment), which could have led to a selection bias. 86 This factor may have affected the overall strength of our conclusions. However, it also reveals the state of the art and can encourage researchers to carry out further high-quality studies on this important topic.
Finally, it may appear unrealistic and unreasonable to expect that school-based gardening interventions alone are capable of appreciably influencing anthropometric variables, or other health outcomes, of the pediatric population. Obesogenic environment is, in fact, part of our modern societies. Children, like adults, have easy access to highly palatable, energy-dense foods, and at the same time, they are living into an ever-proliferating world of labor-saving technologies and electronic amusement. These last factors are particularly important outside of school hours. In particular, numerous studies showed the effect of the family lifestyle on the children's dietary habits, therefore, family involvement will be a primary target for obesity prevention programs in the near future.87,88
Conclusions
This is the first SR, conducted in association with a meta-analysis, measuring the impact of school gardening projects on school-aged children's anthropometric outcomes. Our study shows a moderate degree of descriptive evidence for improvement in consumption of healthy foods in school-aged children undergoing intervention in school and after-school contexts, along with their knowledge of fruits, vegetables, and their healthy properties. Moreover, we found a modest but clinically significant reduction of WC and BMI% in children undergoing gardening project activities during the school hours.
It is key to implement global initiatives aimed to prevent childhood overweight and obesity, which has become a major public health issue globally and is the main driver for adult obesity, metabolic syndrome, and early mortality. Secondarily, since the global financial restraints require a targeted funding allocation, it is important to provide evidence-based, cost-effective, preventive interventions for childhood overweight and obesity. 89 New research on individual factors and personal lifestyles (i.e., diet or physical activity), as well as on the obesogenic environment is a priority to ensure high-quality obesity prevention programs.
Finally, we strongly advocate for the adoption of high-quality study designs in preventive medicine, such as RCTs or quasi-experimental studies, and the use of anthropometric measures, according to the last guidelines on childhood obesity.90,91 This will pave the way for direct comparisons and meta-analyses to guide decisions for the implementation of school-based preventive interventions (including gardening activities) targeted to prevent and fight childhood overweight and obesity.
Footnotes
Acknowledgments
A.R., D.T., and M.P.F. conceived and designed the study. A.R., A.U. carried out the review, acquired, analyzed, and interpreted the data. D.T. checked data extractions. A.R. and D.G. drafted the article, which was critically revised for important intellectual content by all authors. A.R. and D.G. carried out the statistical analysis. D.G. supervised the study. All authors have read and approved the final article. D.G. is guarantor and had full access to all the data and takes responsibility for the integrity of the data and the accuracy of the data analysis.
Funding Information
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Author Disclosure Statement
No competing financial interests exist.