
Abstract
Background:
To develop and test brief nutrition and physical activity screening questions for children ages 2–11 years that could be used as a pragmatic screening tool to tailor counseling, track behavior change, and improve population health.
Methods:
A literature review identified existing validated questions for nutrition and physical activity behaviors in children ages 2–11 years. Response variation and concurrent validity was then assessed using a mechanical Turk (MTurk) crowdsourcing survey employed in 2018. Additionally, cognitive interviews were conducted with both providers and parents of 2- to 11-year-old children to assess screening question priorities and perceived added value.
Results:
The literature review identified 260 questions, and 20 items were selected with expert guidance based on prespecified criteria (simplicity and potential utility for both clinical interactions during a well-child exam and population health). MTurk surveys yielded 1147 records that met eligibility criteria and revealed 6 items that had adequate response variation and were significantly correlated with parent-reported child BMI or BMI percentile, exhibiting concurrent validity. Cognitive interviews with 10 providers and 20 parents uncovered themes regarding suggestions and usability of the questions, eliminating 3 items due to parent and provider concerns. Combining quantitative and qualitative results, 3 nutrition and physical activity screening items remained for inclusion into the electronic health record (EHR).
Conclusions:
The three-pronged validation methodology produced a brief, 3-item child nutrition and physical activity screener to incorporate in the EHR, where it can inform tailored counseling for well-child care and be used to test associations with population health outcomes.
Introduction
Evidence consistently shows that healthy eating and physical activity in childhood facilitates health promotion and disease prevention.1–3 The American Academy of Pediatrics recommends physicians routinely target modifiable behaviors, such as eliminating intake of sugar-sweetened beverages, encouraging consumption of fruits and vegetables, limiting screen time, and promoting moderate-to-vigorous physical activity for an hour per day. 4
Many U.S. children, however, do not meet these recommendations. Less than one-quarter of children participate in 1 hour of physical activity every day. 5 Empty calories, from foods such as soda, fruit drinks, desserts, and whole milk, account for 40% of daily calories in children. 6 Over half of children do not meet fruit intake recommendations, and nearly all children do not meet vegetable intake recommendations. 7
The electronic health record (EHR) provides an opportunity to incorporate consistent health behavior screenings into routine health care longitudinally. Of the EHR tools identified, most focus on increasing identification of overweight and obesity rather than screening for behaviors that might assist providers with prevention and treatment management. 8 The Study of Technology to Accelerate Research (STAR) study found that clinical decision support tools built into the EHR, in addition to direct parent outreach, resulted in improved health care quality measures for childhood obesity for obese children ages 6–13 years.9,10
Despite current research and recommendations to review nutrition and physical activity, screening questions for children have not been consistently included into annual exams through the EHR. In this article, we present our methodology for identifying and developing brief, valid, and meaningful nutrition and physical activity behavior screening questions for children ages 2–11 years to be incorporated into the EHR during well-child examination. A similar process was utilized for identification of items for adolescents and adults although separately analyzed given parents of young children would answer as proxy while adolescents and adults would answer themselves (separate article in preparation).
Methods
A three-pronged data collection and validation methodology (Fig. 1) was used to select nutrition and physical activity screening questions from the literature that provided varied response distributions; demonstrated concurrent validity; and were simple, concise, and noted as value added for patients and providers. First, a literature review was conducted in 2018 to identify an item pool of existing validated questions for children's nutrition and physical activity behaviors. Second, a mechanical Turk (MTurk) crowd-sourcing survey was administered and response distributions and concurrent validity were assessed to reduce the number of items under consideration. Lastly, cognitive interviews with both providers and parents of children ages 2–11 years were conducted to evaluate screening questions, elicit feedback, and guide selection of the final items.
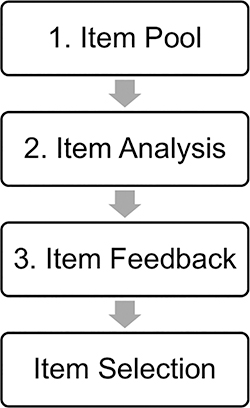
Three-pronged data collection methodology utilized to select screening items.
Item Pool
A literature review using electronic searches of PubMed/Medline sources yielded validated child nutrition and physical activity screening questions in English published from 2000 to 2018. Search terms included: “physical activity,” “nutrition,” “questionnaire,” “survey,” “instrument,” “child,” and “adolescent.” The search was deemed sufficient when similar items were consistently repeated in different questionnaires, implying that no new themes would be identified in further investigation and that item pool saturation was reached. Expert input from the research team represented practicing pediatric primary care providers and interdisciplinary members specializing in health psychology, questionnaire development, and food decision-making perspectives to assess items using these inclusion criteria: relevance for well-child assessments for children ages 2–11 years, question simplicity and clarity, with responses that could be actionable in the context of a clinic-based primary care visit. Items were excluded if they were longer than a few phrases, included long answer choices, difficult to apply to a young age group, applicable only in a cumulative research-oriented questionnaire, or similar to a previously chosen screening question.
Item Analysis
To further cull the questions identified and test for concurrent validity, a crowdsourcing approach through Amazon's MTurk was used. 11 MTurk is an online participant-recruitment service widely utilized for social science research 11 and previously validated by researchers for reliability and better resemblance to the U.S. population than many other available subject pools.12–14 MTurk facilitated rapid access to a heterogeneous research participant pool and provided a platform to conduct research with a large national sample size.11,15
A survey for parents of children ages 2–11 years was created, reviewed by an experienced MTurk developer (J.B.S.), and distributed to anonymous MTurk participants with Vanderbilt Institutional Review Board approval (IRB No. 181135). Inclusion criteria consisted of 18 years or older, legal guardian of at least one child age 2–11 years, and English speaking. Consent was obtained at the beginning of each survey. Consistent with MTurk standards, participants received $0.50 for completing the survey.
To help ensure balanced representation across 2- to 11-year-old ages, the survey was administered separately to parents of children in two age groups (2–5 and 6–11 years old). The surveys included demographic questions for both the parent and the child (such as gender, age, height, weight, educational attainment, race/ethnicity) and the child nutrition and physical activity screening questions identified from the literature review. Child BMI (kg/m2) was calculated from parent-reported child height and weight, and child BMI percentile was calculated using the 2000 CDC Growth Charts to standardize BMI based on approximate child age and gender. 16 Item response distributions were examined through univariate statistics. Most items had five or fewer ordinal response values and were summarized using frequency (%), whereas several continuous items demonstrated non-normal distributions and were best summarized using median (Q1, Q3). Discrete items that had one response category with a frequency >50% were determined to not satisfy the adequate variability criterion. Concurrent validity of the items as measures of child health was evaluated by significant nonparametric Spearman's rank correlation with child BMI or child BMI percentile. Child BMI and child BMI percentile were highly correlated (Spearman = 0.96; p < 0.001), and both were used for validation due to inherent advantages and limitations of each. Statistical significance was defined using a two-sided test at the p < 0.05 level. Statistical analysis was conducted using Stata version 15.1 (StataCorp).
To be eligible for analysis, surveys were required to have complete data. Data were also required for child height, weight, and birth year (used to calculate approximate child age with 2018 as the reference year). Using a protocol from our prior research, 17 extreme values for height or weight were excluded from analysis.
Item Feedback
Cognitive interviews were conducted with both parents and providers to gather opinions on the usability of the questions, practicality of use, and perceived value added to well-child check visits. Interviews were conducted until data saturation was reached. 18 Cognitive interviews were conducted by research staff, with a script incorporating open-ended questions and follow-up prompts to elicit overarching themes and suggestions for the questions. Our multidisciplinary team was concurrently working on a large-scale national study and had developed an interview guide that included probes for identifying the perceived value of the questions as well as problems with wording, ambiguity, comprehension, and response scales. 18 We used this same approach to finalize our interview guide.
Parents of children ages 2–11 years were recruited in person by research staff from the waiting room of Vanderbilt Children's Primary Care Clinic according to the Vanderbilt IRB approval (IRB No. 181135). This clinic serves >85% Medicaid-insured patients. Parent participants were compensated with a $20 gift card after completing the interviews, that lasted on average 20 minutes to refrain from hindering clinical workflow. Inclusion criteria included: English-speaking adults with at least one child age 2–11 years who was a patient of the clinic. All participants signed an informed consent document before participation. Cognitive interview questions were designed to identify parent opinion, interpretation, perceived importance of the nutrition and physical activity screening questions, and assessment of question comprehension.
Vanderbilt Children's Primary Care Clinic providers, including physicians and nurse practitioners, were recruited and interviewed in person or over the phone for 30–40 minutes without compensation, as per IRB. Cognitive interview questions were designed to identify provider opinion, perceived importance, and relevance of the nutrition and physical activity screening questions for children ages 2–11 years.
Each interview was audiorecorded and transcribed verbatim through a remote transcription service. Transcripts were reviewed for themes of value, understandability, wording, ambiguity, comprehension, and recommendations. After deciphering the major themes, each item was assessed as eliciting either overall concern or overall favor from parents and/or providers. Preferred questions were selected based on the full set of themes and items were reworded or discarded, leading to a final decision about items and wording to be included in the brief screening tool.
Results
At each stage, potential questions were excluded, resulting in the final set of items, shown in Figure 2.
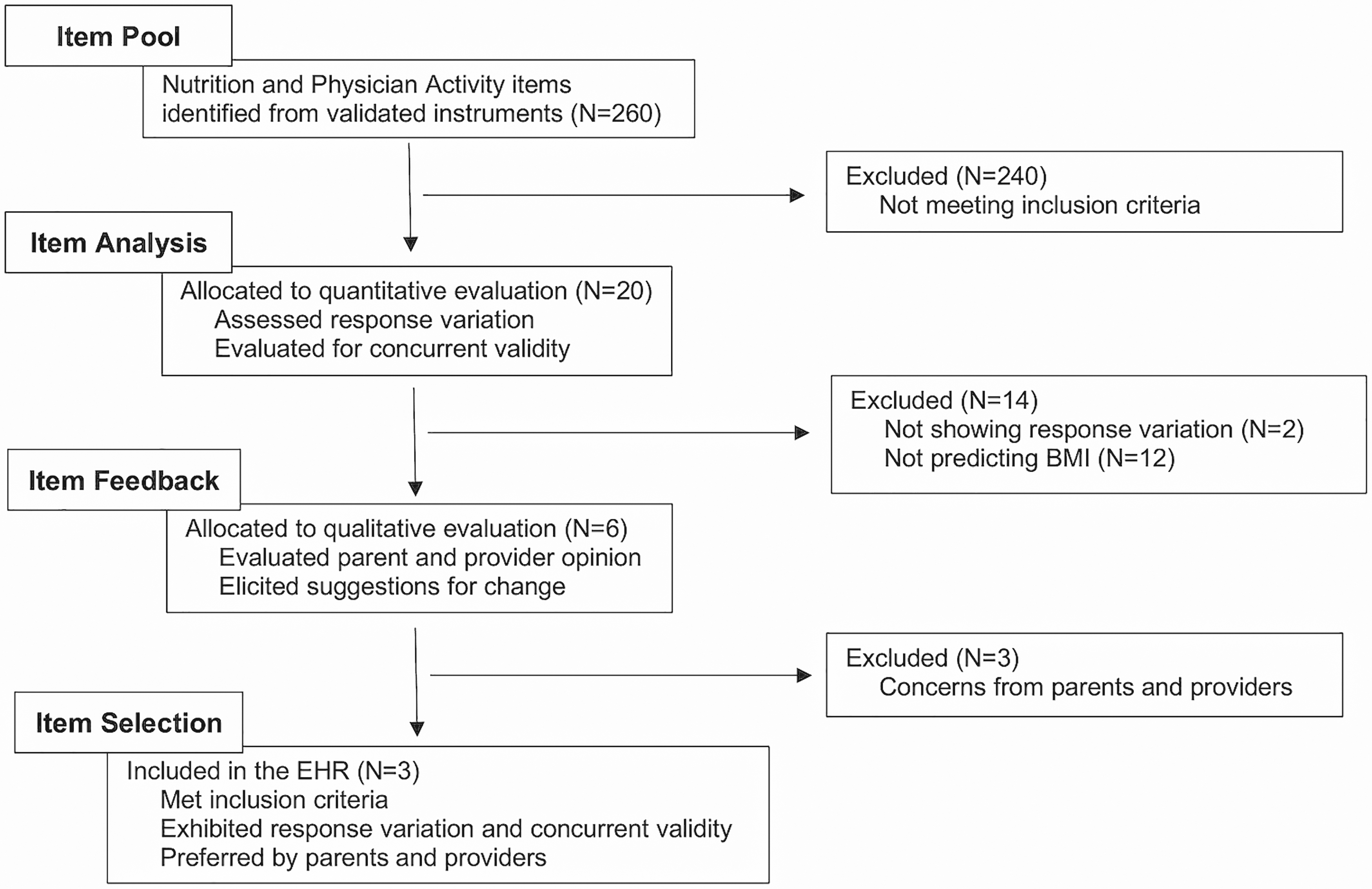
Process for identifying and selecting child nutrition and physical activity screening questions. HER, electronic health record.
Item Pool
From a literature review, 260 existing nutrition and physical activity screening questions were identified from published validated instruments (Table 1). Of the 260 questions, 20 fit our pre-specified inclusion criteria for children ages 2–11 years in a clinic-based primary care setting. These were further evaluated through quantitative and qualitative analysis.
Instruments Identified for Measuring Child Nutrition and Physical Activity (N = 13)
Item Analysis
MTurk surveys were started by 2538 participants, and 1147 met all eligibility requirements for analysis, including completion of all questions and biologically plausible values for parent-reported height and weight. Eligible children had an average (standard deviation [SD]) reported BMI of 17.7 (4.1) kg/m2, BMI percentile of 61.4 (36.1), 76.7% were White, and 56.8% were male. Parents had an average (SD) age of 34.7 (6.8) years, and 60.4% had an education at the bachelor's degree level or higher (Table 2).
Mechanical Turk Participant and Child Demographic Data (N = 1147)
Response distributions for the 20 questions from the item pool are presented in Table 3, and item correlations with child BMI and BMI percentile are reported in Table 4. Questions that demonstrated the strongest significant correlations with child BMI included sugar-sweetened beverage intake (Item No. 3) (r = 0.073; 95% confidence interval [CI] [0.015 to 0.130]; p = 0.014), anxiety around weight (Item No. 9) (r = 0.233; 95% CI [0.177 to 0.287]; p < 0.001), emotional eating (Item No. 10) (r = 0.171; 95% CI [0.114 to 0.226]; p < 0.001), preference to sit or move (Item No. 17) (r = −0.122; 95% CI [−0.178 to −0.064]; p < 0.001), screen time hours (Item No. 18) (r = 0.110; 95% CI [0.052 to 0.166]; p < 0.001), and level of activity (Item No. 16) (r = −0.094; 95% CI [−0.151 to −0.036]; p = 0.0015). Patterns of significant correlations were closely aligned between child BMI and BMI percentile, with two exceptions. While screen time frequency (Item No. 12) and level of activity (Item No. 16) were significantly correlated with BMI, they were not significantly correlated with BMI percentile.
Item Analysis of Child Nutrition and Physical Activity Questions (N = 20)
Survey item data provided as frequency (%) or median (1st quartile, 3rd quartile) to assess response distribution (N = 1147).
For participants who responded “Never” on the general snack question (Item No. 4), a response of “Never” was automatically entered for the three subsequent snack type items (Items No. 5–7).
Concurrent Validity of Survey Items as Measured by Correlation with Child BMI and BMI Percentile (N = 1147)
See Kuczmarski et al. 16
CI, confidence interval; SSB, sugar-sweetened beverage.
Through item analysis, fourteen questions were eliminated (Table 5). Two items (Items No. 9–10) did not display varied response distributions (Table 3), and 12 items (Items No. 1–2, Items No. 4–8, Items No. 13–15, and Items No. 19–20) did not exhibit significant concurrent validity (Table 4). The remaining six questions were further evaluated through qualitative feedback.
Child Screening Question Results from Quantitative and Qualitative Analysis
Light gray indicates the item fulfilled the respective test requirements; medium gray indicates the item did not fulfill the respective test requirements; dark gray indicates the item displayed part of the respective test requirements (i.e., correlated with BMI but not BMI percentile); bold text with gray indicates the item did not fulfill a previous test and was no longer considered for the final question set.
Item Feedback
Twenty parents and ten providers completed cognitive interviews and their responses were transcribed and coded. Overwhelming consensus from parents and providers was reached on the high importance of incorporating nutrition and physical activity screening questions into the well-child exam, with all respondents reporting a 4 or 5 on a 5-point importance scale. Further consensus was reached among providers on the preferred method of utilization during a clinic visit: administered by a medical assistant or nurse before the patient encounter, input into the EHR, and identified within the patient chart during the encounter.
Clear parent and provider themes emerged regarding value of the items, unanswerable items by the parent proxy, preference for quantitative behavior tracking, and desirable reporting (Table 6). Through item feedback, three questions were excluded due to parent or provider concerns, preference for quantification, and/or concerns for socially desirable reporting (Table 5).
Qualitative Themes and Quotes Regarding Reactions to Screening Questions
Consistent suggestions for change also arose throughout qualitative analysis. Providers identified “activity” as a vague term and called for clarification between physical activity and hyperactivity and expressed the need to add popular sugar-sweetened beverages as an example (Table 6).
Quantitative and qualitative analysis converged on three final screening questions that were found to have acceptable variation, significant concurrent validity, and preference from parents and/or providers. Suggestions from parents and providers yielded the following finalized versions of the three questions: (1) Based on a typical week, how often does your child drink sweet beverages (e.g., juice, soda, Gatorade, or chocolate milk)?; (2) In your opinion, how physically active is your child?; and (3) On a typical day, how many hours does your child spend in front of a screen (such as an iPad, smartphone, computer, TV, or video game)?
Discussion
In this study, a three-pronged data collection and validation methodology identified and tested child nutrition and physical activity screening questions that can serve as a tool for discussing health behaviors and tracking individual and population health nutrition and physical activity. Incorporation of such questions has proven to be feasible in clinical routine visits, 19 correlated with greater population health outcomes, 20 and associated with improved health care quality measures. 9 A systematic process to create such questions, however, has not been elucidated in the current literature. In this study, we developed a logical, thorough approach to selecting screening questions, through both quantitative and qualitative methods.
In addition to creating a novel approach, this study elicited several interesting findings. While pooling items, we found few child nutrition and physical activity questionnaires designed for use within busy primary care clinical settings. Furthermore, while physical activity screening questions exist for adults, 21 we had difficulty finding similar questions for children. Importantly, our methodology revealed the importance of capturing both physical activity and sedentary behavior.
Through item analysis, we were surprised to find that parent perception of child physical activity was one of the best tools for screening health behaviors. The level of activity item (Item No. 16) was significantly correlated with child BMI and was included in our final item set, suggesting that parents are aware of their 2- to 11-year-old child's health behaviors. Item analysis also further validated Lewis's sugar-sweetened beverage question (Item No. 3), which has been utilized at Wake Forest Baptist Medical Center as an effective measure. Findings also reemphasized the importance of counseling on screen time (Item No. 18). This aligned well with existing literature.4,19
Qualitative feedback further added value to the study. Before gathering parent and provider opinion, questions testing emotional eating were favored. Upon gathering qualitative data, however, it became clear that emotional questions could hinder the parent–provider interaction for children ages 2–11 years. Additionally, the nutrition item assessing sugar-sweetened beverage intake (Item No. 3) was unexpectedly preferred by parents and providers over those that tested fruits, vegetables, or snacking behaviors.
Limitations
This study has several limitations. The literature review conducted to pool items relied on published databases for identification of existing eligible screening tools and could potentially miss other measures not in the published literature. Beyond literature identification, selection of questions from the item pool involved subjective inclusion criteria with pragmatic input from experts working in clinical settings and did not undergo further methodology, such as a Delphi approach. MTurk's crowdsourcing platform utilized for item analysis was a convenience sample and may differ somewhat from the U.S. population, tending to be more educated and employed. Additionally, the online nature of the surveys may not be directly applicable to a face-to-face interaction with a health care provider. Moreover, reliance on parent-reported measures of child height and weight was a limitation, possibly exacerbated by use of the MTurk platform, which did not allow for independent verification of data. Unavailability of child date of birth to calculate an exact age reduced the accuracy of child BMI percentile and necessitated approximation based on years of age. Use of an approximate BMI percentile enhanced comparability of weight-related data across a wide range of ages. While the interpretation of BMI changes across a wide range of child ages, BMI allowed for sensitivity to high and low BMI values, whereas BMI percentile was bounded at high and low ends. The limitations of each were reduced by use of both measures, and validity was strengthened by the observed high correlation between them (Spearman = 0.96; p < 0.001).
We believe, however, that the study's strengths outweigh these limitations. Research for the item pool was performed systematically, identifying validated questions. For the item analysis, we utilized a large sample size of over 1000 to measure question correlations with child BMI and BMI percentile. Furthermore, the MTurk platform, although a convenience sample, has been validated by scientists for greater reliability and better resemblance to the U.S. population than most other subject pools.12–14 Exclusion of extreme values for height and weight using well-defined criteria enhanced validity and accuracy by removing likely erroneous or fictitious responses (e.g., responses that were fabricated to receive the compensation). During item feedback, we interviewed the subjects of the study as well as providers who deliver patient care. Theme saturation was achieved in each group.
Future Directions
These screening questions are now actively integrated at Vanderbilt University Medical Center, administered by medical assistants, and input into the EHR before provider–patient interaction as part of routine well-child care visits. This approach allows us to assess change in these foundational health behaviors across different ages. Importantly, these screening questions are now available for use in any health care system that wishes to build the items into their EHR, addressing a consistent approach to capturing these important health behaviors.
Future research should assess the impact of standardized child nutrition and physical activity screening questions by objectively measuring individual patient outcomes, such as individual BMI, BMI percentile, and physical activity and nutrition behaviors, and population health outcomes, such as changes in population BMI and hemoglobin A1c over time. Validation of these items in a clinic setting is also needed, ensuring appropriate correlation with objectively and more precisely measured child BMI, BMI percentiles, or z-scores. Further analysis should also study the adoption of the screening items, including discussion of burden among staff and proper connection to provider counseling.
Conclusions
We have described a novel systematic process of vetting and testing brief nutrition and physical activity screening questions for children to include consistently in routine health exams. This tool serves as a starting point for individualized counseling, a database for tracking behavior change over time, and a potential measure of population health outcomes. Future research should examine combining this screener with clinical decision support tools. This approach holds the potential to change the way providers identify and manage common foundational health behaviors seeing the patient over time rather than as a snapshot in time.
Footnotes
Acknowledgments
The authors are grateful to the participants in this study and acknowledge the hard work of the study team that allowed for the high-quality data collection and analysis required for this work. This research was supported by the Vanderbilt University Trans-Institutional Program (TIPS) under a Vanderbilt Initiative Award (ViA).
Funding Information
This research was supported by the Vanderbilt University Trans-Institutional Program award. Also, part of Dr. Barkin's time was supported by a P30 grant from the NIDDK (2P30DK092986-07).
Author Disclosure Statement
No competing financial interests exist.