
Abstract
Background:
Fat distribution is associated with chronic diseases and birth weight may influence fat distribution throughout life. Our aim was to compare fat distribution in children born extremely low birth weight (ELBW) and very low birth weight (VLBW).
Methods:
This retrospective cohort study evaluated children born ELBW and VLBW around the 7th year of life. Fat distribution was assessed by ultrasonography measurements of abdominal subcutaneous and visceral fat thickness. Multiple linear regression analysis was performed.
Results:
We studied 63 children. Visceral fat thickness but not subcutaneous fat thickness was significantly increased in children born ELBW compared with children born VLBW, respectively, 3.13 (±1.08) versus 1.86 (±0.76) mm. This result remained after adjustment for age, gender, and BMI; adjusted coefficient 0.118, 95% confidence interval 0.009–0.227, p = 0.034.
Conclusion:
Children born ELBW seem to have increased visceral fat thickness compared with children born VLBW.
Introduction
In recent decades, there has been a significant increase in survival rates of preterm babies especially those with very low birth weight (VLBW), that is, ≤1500 g and extremely low birth weight (ELBW), that is, ≤1000 g (Ref. 1 ). However, these children have a high prevalence of growth and development failure and high risk for cardiovascular dysfunction, greater insulin resistance, and dysglycemia throughout life.2,3
It has been suggested that the greater cardiometabolic health risk seen in adults born ELBW and VLBW is due to inappropriate fetal development of metabolic tissues, especially body fat distribution. Abdominal fat includes subcutaneous and intra-abdominal fat (omental and mesenteric, visceral depots). Abdominal obesity, especially visceral adipose tissue (VAT), has emerged as an important risk factor for cardiometabolic disease. VAT is highly metabolically active and has been associated with insulin resistance, hypertension, and subclinical atherosclerosis. Fat distribution plays a crucial role in obesity pathophysiology, and its programming is influenced in early life. 4 By the beginning of the third trimester, adipose tissue expands rapidly and premature birth may interfere with a critical period of adipose tissue distribution. 5
Adominal anthropometry measurements have been frequently used, but this method does not distinguish between subcutaneous and visceral adiposity. Computed tomography (CT) and magnetic resonance imaging (MRI) have been considered the gold standards for fat distribution measurement. However, these methods expose children to ionizing radiation (CT) and the need for expensive equipment and specialist technicians; besides MRI frequently requires sedation. Abdominal ultrasonography has been assessed and validated as a noninvasive estimate of fat distribution, that is, visceral and subcutaneous fat depth. This procedure has been shown to be reliable and reproducible when compared with CT or MRI image in all the age groups.6,7
Other studies have shown a correlation between low birth weight and visceral adiposity in neonates and adult life.8,9 Some studies reported that adults born with low birth weight have more abdominal adipose tissue and increased metabolic health risk.10,11 However, there are studies with divergent findings. Kwinta et al. found a lower fat mass in ELBW children at the 7th year of age compared with a control group. 12 Engan et al. also reported lower values for muscle mass, total bone mineral density, and fat mass ratio in children born ELBW and VLBW. 13 A recent systematic review concluded that there is a lack of information on body composition in ELBW infants. 14 Thus, this subject is still controversial, especially in children born ELBW, and fat distribution during the growth of these children remains poorly understood. Our hypothesis was that there is a greater abdominal fat accumulation in children born ELBW compared with children born VLBW. Our aim was to compare abdominal fat distribution, that is, subcutaneous and visceral fat thickness in school-age children born ELBW and VLBW.
Methods
This was a retrospective cohort study performed at the Kangaroo Mother Care Unit, Instituto de Medicina Integral Prof. Fernando Figueira (IMIP), Brazil. IMIP is a hospital dedicated to the low-income population and most of patients have an annual per capita income of US$1025 or less. The Kangaroo Mother Care Unit offers a follow-up health care program for premature and low birth weight babies until the school age. This study was developed from March 2017 to July 2019. This project was previously approved by the Research Ethics Committee of IMIP (CAAE: 58833016.9.0000.5201) and all mothers signed an informed consent.
Children born with birth weight between <1500 and ≥1000 g (VLBW) and <1000 g (ELBW) admitted to Kangaroo Mother Care Unit between March 2011 to February 2012 and regularly accompanied (minimal attendance of two postdischarge follow-up visits during the 1st year of life and one visit from the 2nd to 7/8 years of life) until July 2019 were considered eligible (Fig. 1). Exclusion criteria were as follows: genetic syndromes, severe malformations or diseases that compromise growth, and intensive care unit hospitalization during the 1st year of life. Data delivery, Kangaroo Mother Care assistance, and health care monitoring until the 7th/8 years of life were taken from medical records. Gestational age was calculated based on last menstrual period or first-trimester obstetric ultrasound. Current weight was measured with minimal clothing to the nearest 0.1 kg with an electronic scale. Height was measured without shoes using a stadiometer to the nearest 0.1 cm. A standard technique was performed. Small for gestational age was defined as below 10th percentile, according to the Fenton growth chart. 15 Postnatal catch-up growth during the 1st year of life was defined as a change in the Z-score >0.67 between 0 and 12 months of age according to Westerberg. 16

Flowchart of participants in the cohort study. ICU, intensive care unit.
Ultrasonography has been considered an accurate method for determining abdominal fat thickness. 17 Abdominal subcutaneous and preperitoneal adiposity thicknesses, a measure of visceral fat, were measured by an ultrasound (Envisor Scanner, Philips Ultrasound, Bothel, WA) with a linear array probe L12-5 (38 mm, 5–12 MHz) in the supine position. The probe was positioned perpendicular to the skin of the median upper abdomen and touched as lightly as possible to prevent compression of the fat tissues. To obtain a transversal image with maximum preperitoneal fat thickness, the probe was moved longitudinally and perpendicularly to the linea alba from the xiphoid process and the umbilicus. The thicknesses of the fat layers were measured in this transversal image; the preperitoneal fat thickness was determined by the maximum height of the triangular-shaped area in the transversal image and the maximum subcutaneous fat thickness was measured directly above this triangular area. All measurements were performed by the same researcher (E.J.S.).
Data on each numeric variable were expressed as means with standard deviations or medians with interquartile ranges, as appropriate. Independent sample t-tests were used to compare the ELBW versus VLBW groups on quantitative variables with normal compatible distributions. The proportional differences for categorial or categorized variables were tested with the chi-squared test or Fisher's exact test, as appropriate. The Wilcoxon rank-sum test was used to compare fat distribution between the two groups due to the presence of a few unusually large values and skewness in their distributions. Multiple linear regression analyses were also performed to assess the relative contribution of other variables on abdominal fat distribution in children born VLBW and ELBW. Analysis was performed using STATA version 12.1 (Statacorp, TX) and R (R Core Team 2020), and a significance level of 0.05 was accepted.
Results
We studied 63 children, 44 born VLBW and 19 born ELBW, 39 boys and 24 girls. ELBW children had a lower gestational age and current weight and height compared with VLBW children (Table 1).
Characteristics of Extremely Low Birth Weight and Very Low Birth Weight Children
Two-tailed t-test for continuous variables and chi-squared test for categorical data.
ELBW, extremely low birth weight; VLBW, very low birth weight.
The presence of outliers and skewness in the data (Fig. 2) cast doubt on the use of the Student's t-test to compare the two groups. Thus, we used the Wilcoxon–Mann–Whitney test. Visceral fat thickness, but not subcutaneous fat thickness, was significantly increased in children born ELBW compared with children born VLBW, respectively, 3.13 (±1.08) mm versus 1.86 (±0.76) mm, two-sample Wilcoxon rank-sum test p < 0.03 (Table 2). The estimated probability that preperitoneal abdominal fat was higher for the ELBW group than for the VLBW group was 66.4% [95% confidence interval (CI): 51.7%–81.1%] and the estimated probability that subcutaneous fat was higher for the ELBW group than for the VLBW group was 65.5% (95% CI: 50.0%–81.0%). Multiple linear regression analyses showed that this difference persisted after adjustment for age, gender, abdominal circumference, and BMI (adjusted coefficient 0.118, 95% CI 0.009–0.227, p = 0.03).
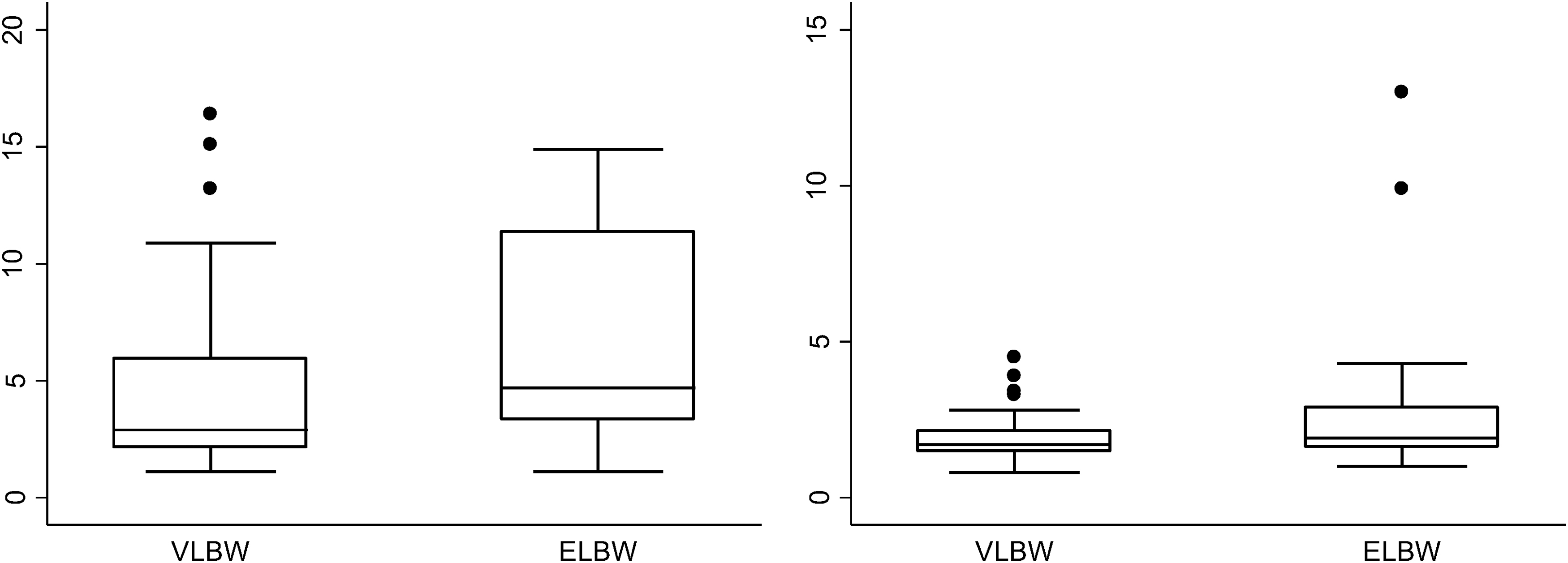
Boxplots show the distributions of subcutaneous fat thickness and visceral fat thickness between children born ELBW and VLBW. ELBW, extremely low birth weight; VLBW, very low birth weight.
Fat Distribution among Extremely Low Birth Weight and Very Low Birth Weight
Two-sample Wilcoxon rank-sum test.
Discussion
Children born ELBW showed visceral fat excess compared with children born VLBW. Visceral fat excess in children at school age remained associated with ELBW after control of confounder variables: gender, age, BMI, and abdominal circumference. Some authors report that a suboptimal environment, including severe prematurity during adipose tissue development, plays a crucial part in defining an individual's propensity for accumulating abdominal visceral fat later in life. 18 Adipose tissue development begins during the second trimester of fetal life and expands rapidly in the third trimester. The other period of increase in adipose tissue occurs during the 1st month of life, and only some adipogenesis continues throughout childhood and adulthood. Therefore, ELBW and VLBW newborns lose a critical period of adipose tissue expansion and they exibit a fat distribution different than that of term born neonates. 19 Furthermore, it seems that fat excess persists until school age and maybe throughout life increasing the risk for chronic diseases. Adults born VLBW and even more ELBW are more susceptible to cardiovascular diseases, type 2 diabetes, and chronic kidney injury. 8 Adipose tissue is now acknowledged as a major endocrine tissue involved in functions that may impact homeostasis and develops diseases.
Regarding fat distribution in ELBW infants, there remains some controversy. A recent systematic review reported only two studies on fat distribution in ELBW infants. 14 ELBW infants had a higher VAT deposition in one cohort study with 96 participants, 19 which is in agreement with us. The other study showed higher subcutaneous fat tissue 20 and elevated hepatic, pancreatic, and subcutaneous fat deposition in 29 ELBW adults. The authors of this systematic review concluded that there is a lack of long-term information on body composition in ELBW children. A cohort study of ELBW subjects found that these adults had increased body fat, and a fourfold increased risk of developing dysglycemia. 21 A previous study has found greater hepatic, intramuscular, and abdominal fat content in adults born preterm (mean gestational age of 29 weeks) compared with normal birth weight term controls. 22 Raaijmakers et al. reported that adolescents born ELBW and catch-up growth in the first 2 years of life had a lower percentage body fat. 23 Kwinta et al. 12 studied 81 children born ELBW in the 7th year of life and found a lower fat tissue mass. These children were also shorter and had lower body mass compared with their peers. However, fat distribution in this study was calculated by anthropometric measurements and not by ultrasound. Anthropometric measurements assess indirectly visceral fat. Ultrasound has been considered a gold standard method for measuring visceral fat. 17
There are several strengths to the present study. No prior investigations have assessed abdominal visceral fat measured by ultrasound in ELBW survivors. We were able to perform a retrospective cohort study with children born ELBW and VLBW at 7 years of age, who were born and followed in a teaching hospital. Moreover, we assessed abdominal fat distribution by ultrasound. Ultrasound assessment of subcutaneous and visceral fat has been shown as an accurate method. Our study also has some limitations. First, we studied few children born ELBW; although this number could demonstrate a mean difference of 0.97 mm between fat thickness of the two groups, according to a poststudy sample size calculation (α 0.05 and power 80%), we found a mean difference of 1.27 mm; 3.13 mm (ELBW) minus 1.86 mm (VLBW). The mortality rate for ELBW is high especially in undeveloped and developing countries; the mortality rate in IMIP is ∼70%. Second, since the mortality rate for ELBW is high in our hospital and we did not present data on deaths, and neurodevelopmental impairment, our results may not be generalized to other populations owning to selection bias. Third, we did not perform whole-body composition and we could not control all variables that could potentially interfere with fat distribution. A range of factors determine fetal adiposity, including gender, maternal body composition, fetal growth, and breastfeeding. In this study, we did not observe differences regarding intrauterine growth restriction, catch-up growth during the 1st year of life, or breastfeeding among children ELBW or VLBW.
Conclusion
School children born ELBW had more abdominal visceral fat compared with children born VLBW. This finding implies an increased risk of cardiometabolic diseases later in life and needs to be confirmed in larger studies.
Footnotes
Funding Information
No funding was received.
Author Disclosure Statement
No competing financial interests exist.