
Abstract
Background:
Among adults, weight stigma is associated with markers of poor cardiometabolic health. Although weight-based teasing (WBT) is common among youth with high body weight, few studies have examined its associations with cardiometabolic markers. Owing to unique stressors (e.g., parental deployment and frequent moves), military-dependent youth may be at particularly high risk for obesity, WBT, and poor cardiometabolic health. We, therefore, assessed associations between WBT and cardiometabolic health markers among adolescent military dependents presenting for a weight gain prevention trial.
Methods:
Participants underwent fasting phlebotomy; had fasting weight, height, and waist circumference measured; and completed assessments of WBT, anxiety, and loss-of-control eating. Multivariate analysis of covariance, adjusting for relevant covariates including demographics and body composition, was used to examine differences in metabolic syndrome (MetS) components (waist circumference, systolic and diastolic blood pressure, high-density lipoprotein cholesterol, triglycerides, and glucose) between youth reporting WBT and youth reporting no WBT. Bootstrapped models examined whether WBT mediated the relationship between BMIz and MetS components.
Results:
Data from 142 youth (57.7% female; 14.4 ± 1.6 years; 51.2% non-Hispanic White, 20.9% non-Hispanic Black; BMIz: 1.9 ± 0.4) were analyzed. WBT was not significantly associated with any MetS component. Relationships were observed between BMIz and all MetS components (except systolic blood pressure and glucose), although WBT did not significantly mediate these relationships (p's > 0.05).
Conclusions:
This study did not find support for a relationship between WBT and MetS components in adolescent military dependents at risk for adult obesity. Prospective research is needed to determine whether associations between WBT and adverse cardiometabolic outcomes emerge primarily in adulthood.
Introduction
Persons with high body weight are vulnerable to pervasive societal stigma and discrimination. 1 Among adults, associations have been documented between weight-based stigma and poor psychological and physical health,2,3 above and beyond the contribution of body composition or excess adiposity.4,5 Specifically, associations have been observed between weight-based stigma and discrimination and markers of cardiometabolic health including elevated allostatic load, 6 glycated hemoglobin, 6 F2-isoprostanse (a marker of oxidative stress), 7 C-reactive protein, 8 salivary cortisol, 9 and cortisol reactivity. 10 Furthermore, weight-based stigma in adults is associated with behavioral and physiological stress processes that may contribute to adverse cardiometabolic health in vulnerable individuals.7,10–12
Weight-based teasing (WBT) is the most common form of bullying reported among youth, however, limited research has examined WBT and markers of cardiometabolic health in pediatric samples. Importantly, children and adolescents with overweight and obesity have a far greater likelihood of experiencing WBT than their peers without overweight,13,14 and the majority of high school students report witnessing others being teased due to high body weight. 15 Youth experience WBT from a variety of sources, including parents, siblings, peers, and teachers, and across domains, including home, school, and health care settings. 16 Adolescents who have experienced WBT demonstrate low self-esteem and greater body dissatisfaction, depression, loneliness, suicidality, and social isolation.13,17–19
Given that WBT appears to be a significant psychosocial stressor among youth with high body weight, it is plausible that youth affected by WBT may also be at risk for poor health outcomes. For instance, teasing among adolescents has been associated with unhealthy eating and obesogenic behaviors, including binge eating and overeating,11,20,21 restrictive dieting, 22 and avoidance of exercise. 23 A distinct, but related construct, pressure to be thin has also been associated with insulin resistance and greater odds of hyperinsulinemia in adolescents after adjusting for body composition. 24 These relationships may putatively be driven by physiologic stress, negative affect, and disordered-eating behaviors.
Longitudinal data lend further support for the links between WBT and health; prior research indicates that WBT may place youth at risk for greater weight and adiposity gain over time, even after adjusting for baseline levels of these variables,25,26 which ostensibly may contribute to the development of worsening cardiometabolic health. 27 However, studies directly assessing the associations between WBT and markers of cardiometabolic health in youth are limited, 28 signaling a need for greater attention to this area. In particular, assessing these links within high-risk populations of youth is necessary to improve our understanding of the associations between WBT and health during critical periods of development, such as adolescence. 29
One such high-risk population may be the adolescent children of military service members. Prior research has found that adolescent military dependents with overweight and obesity may be at high risk for WBT, and that those reporting WBT have poorer social functioning, lower self-esteem, and greater eating pathology and depression. 30 Furthermore, military dependents face unique stressors due to their parents' careers, such as parental deployments, relocations, and concerns about parental safety, which collectively may increase risk for obesogenic behaviors, such as binge eating and disordered eating.31–33 In addition, heightened attention to weight loss and fitness in the U.S. military might promote weight stigma among service members, giving rise to WBT in military families. 34 To date, however, no research has examined associations between WBT and indices of health among adolescent military dependents. Given that these youth may be at considerable risk for psychosocial stress,31,32,35 coupled with the fact that the children of service members are more likely to join the military than their civilian peers, 36 attention to the links between WBT and health among this population is warranted.
We, therefore, examined associations between WBT and components of metabolic syndrome (MetS), a cluster of risk factors that collectively indicate cardiometabolic health risk 37 among adolescent military dependents at high risk for adult obesity and binge-eating disorder.31–33 As some research among adults indicates that weight stigma may partially explain the link between adiposity and cardiometabolic risk,6,38–40 the mediating effect of WBT on the relationship between body composition and MetS was also explored. We hypothesized that the presence of WBT would be associated with worsened MetS components and that WBT would partially mediate the association between BMIz and MetS.
Methods
Participants
This study included baseline data from an obesity and eating disorder prevention trial (ClinicalTrials.gov ID No.: NCT02671292) for adolescent military dependents at risk for adult obesity and binge-eating disorder [BMI ≥85th percentile adjusted for age and gender 41 and either at least one episode of loss-of-control (LOC) eating during the previous 3 months 42 and/or elevated anxiety symptoms (≥32 on the trait scale of the State-Trait Anxiety Inventory for Children)].5,43–45 Adolescents were eligible for the study if they were 12–17 years old and English speaking and excluded if they met at least one of the following criteria: a major psychiatric or medical condition (including pregnancy), weight loss exceeding 3% of body weight during the past 3 months, current participation in psychotherapy or a structured weight-loss program, or regular use of prescription medications that affect appetite or body weight (unless weight stable for ≥3 months before the start of the study).
This study received approval from the Uniformed Services University Institutional Review Board and the Fort Belvoir Community Hospital Research Office. TRICARE-eligible adolescent military dependents in the Washington, DC metro area were identified through the Defense Enrollment Eligibility Reporting System and recruited through direct mailings addressed to parents. Other sources of recruitment were referrals from providers and flyers posted on military bases and listservs.
Procedures
A brief phone screen determined preliminary eligibility followed by an in-person baseline visit. Participants and their parents/guardians provided written assent and consent, respectively, and participants completed a fasting blood draw, measures of body composition, and psychosocial questionnaires and interviews. All data were derived from this baseline visit, before any intervention.
Measures
Body composition
Height (cm) and fasting weight (kg), measured while wearing light clothing with shoes removed, were used to calculate BMI (kg/m2). BMIz scores were calculated, adjusting for age and gender, using the CDC Standards. 46
LOC eating
The presence of LOC eating in the past 3 months was assessed by the Eating Disorder Examination Interview v.14 OD/C.2, 47 a semi-structured clinical interview that has demonstrated high reliability among samples of adolescents. 48 This interview was administered by trained postbaccalaureate or graduate students.
Anxiety
The trait subscale of the State-Trait Anxiety Inventory for Children is a 20-item self-report measure of trait anxiety that has demonstrated strong internal consistency in prior studies. 44 Example items are “My hands get sweaty” and “I worry about things that may happen.” Response options range from 1 = “Hardly-Ever” to 3 = “Often.” Scores range from 20 to 60 with higher scores indicating greater trait anxiety. Internal consistency in the current sample was α = 0.75.
Perception of Teasing Scale
The 6-item WBT subscale of the Perception of Teasing Scale (POTS) 49 assesses the lifetime frequency of teasing due to high body weight. Example items include “People made fun of you because you were heavy” and “People called you names like ‘fatso’.” Response options range from 1 = “Never” to 5 = “Very often,” with higher scores indicating greater frequency of teasing. Internal consistency of the POTS in prior studies of adolescents with or at risk for obesity was good to excellent.26,49 In the current sample, internal consistency was α = 0.91.
Metabolic syndrome
All components of MetS [waist circumference (cm), systolic and diastolic blood pressure (mmHg), high-density lipoprotein cholesterol (HDL-C; mg/dL), triglycerides (mg/dL), and glucose (mg/dL)] were assessed. 37 Waist circumference was measured in triplicate at the iliac crest. Blood pressure (mmHg) was measured with the Life Source UA-789 Digital Blood Pressure Monitor (A&D Medical, San Jose, CA). HDL-C, triglycerides, and glucose were measured from fasting blood samples collected by trained phlebotomists and analyzed on Cobas 6000 c 501 (Roche Diagnostics, Indianapolis, IN) systems using standard procedures. 50
Data Analytic Plan
Data were screened for univariate and multivariate normality, and relevant assumptions were checked for each analysis. Five plausible univariate outliers, defined a priori as at least 3 standard deviations (SDs) from the mean, were recoded to that threshold. 51 No multivariate outliers with Mahalanobis distances meeting the criteria of chi-square critical value for p < 0.001 were present for any analysis after recoding the univariate outliers. Missing data were <3% of observations for each variable and estimation maximization was used to impute the remaining missing values (Little's MCAR test: chi-square = 305.43, df = 368, p = 0.99). Scores on the POTS were highly skewed with many respondents reporting no instances of WBT; thus, similar to previous studies in this area,52,53 scores were dichotomized to indicate presence (i.e., any response other than “Never”) versus absence (a response of “Never” on all items) of WBT.
Chi-square tests and independent samples t-tests were used to examine differences between participants reporting WBT versus those reporting no WBT on demographic variables, LOC eating status, BMIz, and anxiety. A multivariate analysis of covariance (MANCOVA) was then conducted using presence versus absence of WBT as the independent variable and the MetS components as dependent variables. The MetS components were included in the model as continuous variables due to a lack of consensus over clinical cut-offs in adolescents. 54
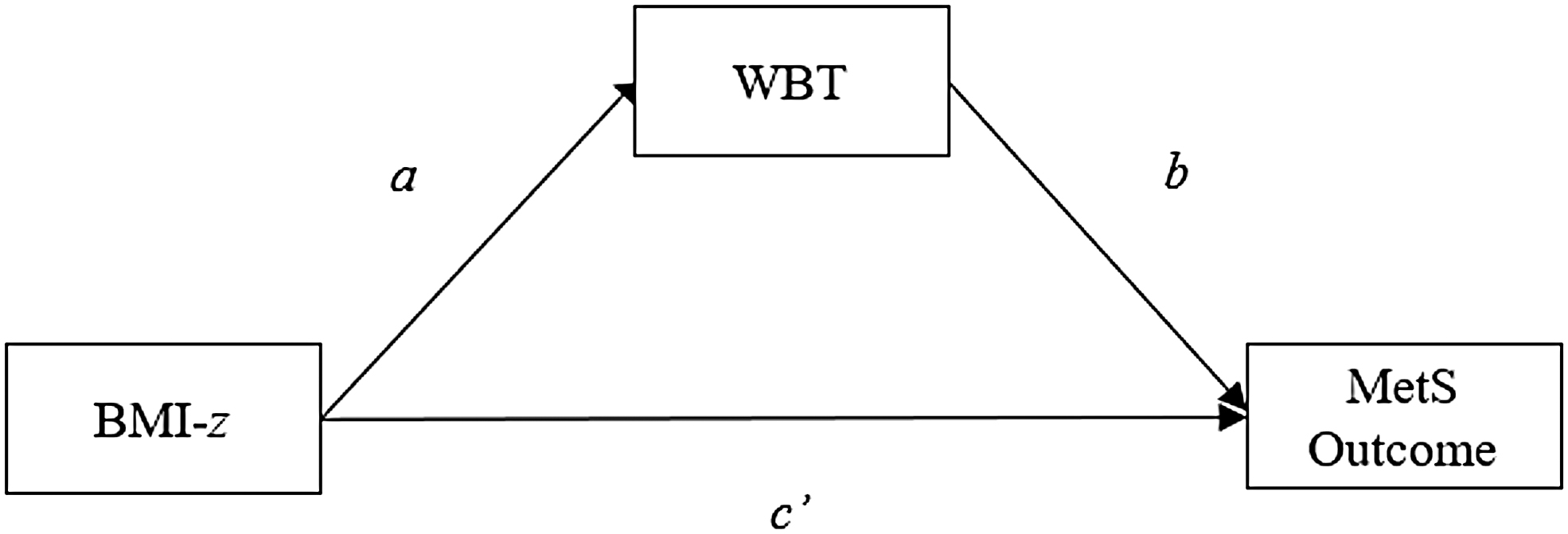
The MANCOVA was conducted using IBM SPSS 25.0 (IBM Corp., Armonk, NY). Covariates included were age (months), gender (female = 0, male = 1), race (0 = non-Hispanic White, 1 = other), LOC eating status (0 = absent, 1 = present), BMIz, and anxiety symptoms. The presence of LOC eating and anxiety were included as covariates as they were inclusion criteria for participation. To determine whether the presence of WBT mediated the associations between BMIz and components of MetS, a series of mediation analyses were conducted with bootstrapped 95% bias-corrected confidence intervals (CIs; samples = 5000) using the weighted least squares means and variance (WLSMV) estimator in Mplus v.8. These analyses were run sequentially with each of the MetS components as outcomes, BMIz as the independent variable, and presence versus absence of WBT as the mediating variable, adjusting for age, gender, race, LOC eating status, and anxiety symptoms (Fig. 1). CIs for the indirect pathways (ab) that did not include 0 were considered statistically significant. 55 All tests were two-tailed and p's < 0.05 were considered significant.
Three sets of supplementary analyses were run to corroborate results of the primary analyses. First, the MANCOVA and mediation analyses were repeated using the Weight-Based Victimization Scale, in lieu of the POTS. 15 This scale has not been adequately validated, but includes items that reflect more recent bullying trends, such as comments made on social media. 56 Second, to assess whether WBT is associated with the presence of MetS, which may be occluded when the MetS components were examined individually, a logistic regression was conducted to predict MetS status (defined by aggregated criteria used in previous studies of youth).57–59 Third, the general linear model used for the MANCOVA was repeated using log-transformed continuous (rather than dichotomous) POTS scores to assess associations between teasing and MetS components with more granularity. The pattern of findings was the same across the primary and supplementary analyses; for clarity and concision, only the former are reported here. Information about the Weight-Based Victimization Scale, the aggregate MetS criteria, and full results from the three additional analyses are provided in Supplementary Data.
Results
Participant Characteristics
A total of 142 adolescents (14.4 ± 1.6 years; 57.7% female; 51.2% non-Hispanic White, 20.9% non-Hispanic Black; BMIz: 1.9 ± 0.4; 74.6% with obesity) were included. The majority of participants (67%) reported the presence of WBT (mean ± SD: 18.34 ± 9.63). See Table 1 for participant characteristics by teasing status and Table 2 for a full correlation matrix of relevant variables. Youth reporting WBT had significantly greater anxiety symptoms (p < 0.01); there were no other significant differences (p's > 0.05) between those reporting WBT and those not reporting WBT.
Participant Characteristics by Weight-Based Teasing Status (N = 142)
Data presented as mean (standard deviation) unless otherwise noted.
Group differences are significant at p < 0.05 for independent samples t-tests or chi-square analyses, as appropriate.
LOC eating presence in the past 3 months.
BMIz, body mass index adjusted for age and gender; HDL-C, high-density lipoprotein cholesterol; LOC, loss-of-control; WBT, weight-based teasing.
Pairwise Correlations for Continuous Weight-Based Teasing Scores as Determined by the Perception of Teasing Scale
Pearson and point-biserial correlations. Gender (0 = female, 1 = male) and LOC eating (0 = absent, 1 = present) are dichotomously coded.
Note: *p < 0.05, **p < 0.01.
WBT scores are logarithmically transformed.
Multivariate Analysis of Covariance
The results of the multivariate test for the MANCOVA (Table 3) did not support an association between presence of WBT and any of the MetS components (HDL-C, triglycerides, glucose, systolic blood pressure, diastolic blood pressure, and waist circumference); p's > 0.27.
Multivariate Test Assessing Associations between Weight-Based Teasing and Metabolic Syndrome Components
Mediation Analyses
The path between WBT and BMIz was nonsignificant (α = 0.23, p = 0.45, [−0.35 to 0.85]). The direct effects of BMIz on waist circumference, diastolic blood pressure, HDL-C, and triglycerides were significant after adjusting for covariates, whereas the direct effects of BMIz on systolic blood pressure and glucose were not. The analyses did not provide support for a mediation effect of WBT on the relationship between BMIz and any of the MetS components after adjusting for covariates (Table 4).
Indirect and Direct Path Coefficients for the Mediation of Weight-Based Teasing Status on the Relationship between Body Composition and Components of Metabolic Syndrome
Path coefficients are unstandardized with 95% confidence intervals, adjusting for demographic variables, LOC eating, and anxiety symptoms. The ab path indicates the presence of mediation.
Confidence interval does not contain 0.
Discussion
This study examined associations between WBT and MetS components among adolescent military dependents at risk for adult obesity and binge-eating disorder. At least one instance of WBT was reported by 67% of participants and was associated with greater anxiety. This finding corroborates prior studies linking WBT with psychological difficulties among children and adolescents with overweight.13,18,19 WBT may be particularly relevant for adolescent military dependents with overweight and obesity due to the emphasis on fitness and appearance standards in military culture, which may be endorsed and modeled within some military families. 34 Military adolescents may also be vulnerable to WBT and its adverse psychological sequelae due to exposure to unique stressors, such as parental deployments and frequent moves and school changes.31,60 Collectively, these stressors may lead to the disruption of peer groups and social support networks, changes in family roles and responsibilities, and worries about the well-being of deployed parents.31,61
Findings, however, did not support associations between WBT (as assessed by either measure) and any marker of cardiometabolic health after adjusting for relevant covariates, including demographics and body composition. Furthermore, WBT did not mediate the relationships between body composition and MetS components. These findings are consistent with a recent study that detected no significant associations between WBT and MetS components in two samples of civilian youth, but differ from research in adults showing a relationship between weight-based stigma and markers of cardiometabolic risk.6,28,53 It is, therefore, plausible that the observed associations between weight stigma and cardiometabolic health emerge over time or primarily in adulthood, after greater chronicity of WBT and subsequent stress. Prior studies indicating that the health-related effects of adverse childhood events may manifest in adulthood lend possible support for this.62,63 Although no study has assessed the long-term effects of WBT on cardiometabolic health, research linking adverse childhood events, such as bullying (not specifically due to weight), with poor cardiometabolic health in adulthood,64,65 suggests that teasing in youth may contribute to worsened health over time. If the physiological correlates of weight stigma tend to emerge in adulthood, then adolescence may be a critical period for prevention, before the onset of the harmful sequelae observed in adults. Longitudinal studies to assess whether WBT in adolescence is associated with cardiometabolic function in adulthood are needed to elucidate at what age, and under what conditions, weight-based stigma may confer additional risk for poor health outcomes.
The lack of association between WBT and markers of cardiometabolic health may also be accounted for by the relative overall health and/or resilience of participants in this study. Studies in adults with obesity have shown that the presence of MetS is generally associated with worse overall health.66,67 The participants in this study may have been healthier than similar weight peers due to the exclusion of individuals with clinically significant medical comorbidities; thus, they may also have had better cardiometabolic health than peers of a similar BMI. The health impacts of WBT may also have been ameliorated by the relative resilience of military-dependent adolescents in adjusting to stressors in their social and family environment.31,68,69 Alternatively, since the study excluded individuals with average or below average body weight, there may have been fewer individuals without WBT, but with excellent metabolic health, to see straightforward relationships between these variables.
It is likely that the effects of WBT on health vary depending on the type of teasing (e.g., source, salience, and chronicity), the subjective response of the individual targeted, and their social and family environment. For example, during adolescence, WBT perpetrated by peers has been associated with greater depressive symptoms than WBT from parents, which may reflect the increasing influence of peers during this age period. 70 Furthermore, some adolescents experience greater negative affect in response to WBT than others, and this is linked with greater dysfunction, such as avoidance coping and poorer school performance. 19 WBT in adolescence can also coalesce with other factors, such as social connection and family environment, to influence long-term health risks.71,72 Thus, additional research is warranted to explore how the health effects of WBT are influenced by different forms and sources of teasing, an individual's subjective interpretation of and reaction to the teasing incident, and their existing social and family support.
Strengths of this study include its focus on a vulnerable and understudied population and its objective measurement of physiological variables. Limitations include the use of a sample of military-dependent adolescents seeking obesity prevention, which likely does not extend to the general population of military-dependent adolescents or to adolescents with overweight and obesity more broadly. Despite the potential lack of generalizability, this population is important to study due to their heightened risk of binge-eating disorder,35,73 vulnerability to WBT,13,14 and, given that the children of service members are more likely to serve in the military than their civilian counterparts, 36 the potential implications for military readiness. Research should assess associations between WBT and cardiometabolic health among more heterogeneous samples of adolescent military dependents, both cross-sectionally and prospectively.
Taken together, there is complexity in the relationship between bully victimization and health indices.64,74 The potential long-term consequences of WBT are supported by the research showing links between nonspecific bullying and cardiometabolic risk factors,64,65 WBT and weight and adiposity gain,25,26 as well as the research on weight-based stigma and adverse cardiometabolic health outcomes in adults.7,10,26 Research is needed to elucidate the associations between WBT and indices of cardiometabolic health among youth, particularly those who may be most vulnerable to obesity, stress, and related comorbidities. Prospective research is needed to determine additional factors that contribute to the documented relationships between weight stigma and poor health outcomes in adulthood.
Footnotes
Disclaimers
The opinions and assertions expressed herein are those of the authors and are not to be construed as reflecting the views of Uniformed Services University of the Health Sciences, the National Institutes of Health, or the United States Department of Defense. The funding sources had no involvement in study design, in the collection, analysis, and interpretation of data, in the writing of the report, or in the decision to submit the article for publication.
Funding Information
This research was supported by NIDDK 1R01DK104115-01 to M.T.-K., and the Defense Health Agency, MED 83-10180 to M.H. J.A.Y. is supported by the Intramural Research Program, Eunice Kennedy Shriver National Institute of Child Health and Human Development, ZIA-HD-00641.
Author Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.