
Abstract
Background:
Childhood obesity is an ever-growing public health concern in the United States and globally. By 2030, it is estimated that 70% of the world's population of children and adolescents will be obese. Therefore, efforts to reduce childhood obesity are of utmost importance, particularly with the current coronavirus disease 2019 pandemic, as rates are expected to soar due to social distancing measures and restrictions. This systematic review aims to examine the literature regarding the effectiveness of clinic-based telehealth vs. face-to-face modalities to reduce obesity among school-aged children.
Methods:
An electronic database search of articles published in English over the last 10 years was undertaken in PubMed, Medline, and CINAHL. Key terms used to identify studies included school-aged children and adolescents with overweight and obesity in clinic-based weight management interventions conducted face-to-face or via telehealth, and having efficacy determined through changes in measured child BMI as primary outcomes and dietary and physical activity changes, as well as assessing feasibility and satisfaction with telehealth, as secondary outcomes.
Results:
Out of 1093 articles identified, 10 met the inclusion criteria. While both telehealth and face-to-face weight management interventions are effective in reducing obesity in children and adolescents, the evidence is lacking in which is more effective. Of the 10 studies, 5 showed outcome improvements when both telehealth and face-to-face interventions were combined as adjunct therapies.
Conclusions:
Findings support using telehealth in conjunction with face-to-face visits for obesity treatment among children and adolescents. However, more research involving telehealth weight management interventions for young children is recommended.
Introduction
Children and adolescents with obesity is an ever-growing public health concern in the United States and on a global scale. 1 The prevalence of obesity among children and adolescents aged 5–19 has risen from 4% in 1975 to over 18% in 2016. 2 By 2030, it is estimated that 20% of the world's population will be obese. 3 High consumption of energy-dense foods and sugary beverages exceeding total energy expenditure is the primary driver for excess weight gain among children and adolescents. 4 In addition, disrupted sleep patterns, low levels of physical activity, and extended use of screen time also lead to rapid weight gain in this population. 5 Childhood obesity is a predisposing factor to several chronic diseases and conditions, such as type 2 diabetes, heart disease, sleep apnea, certain cancers, and hypertension, later in life. 6
Amid the pandemic of coronavirus disease 2019 (COVID-19), medical facilities have implemented social distancing regulations making face-to-face obesity management challenging for practitioners and recipients. 7 The unprecedented self-quarantine during the pandemic has led to widespread concern on increasing the risk of childhood obesity. 8 Children and adolescents may find themselves in quarantine eating in response to stress, lacking sleep, less physically active, and spending more time on screens. 9 Managing obesity in this population is critical, given it may increase their risk for contracting COVID-19 and can worsen outcomes from the virus if left untreated. 10 However, the COVID-19 pandemic has forced weight management clinics to reduce in-person visits due to social distancing and provide virtual services. 11
Despite the growing need for using telehealth to treat children and adolescents with obesity, this modality can potentially create obstacles for patients requiring more intensive levels of treatment.12,13 The current guidelines for pediatric obesity treatment recommend four stages for weight management. Stage 1 occurs individually in a primary care office and stage 2 involves a multidisciplinary team intervention. Advanced stages of treatment require more frequent and routine visits. Stage 3 is a family-based intervention characterized by weekly visits for 2–3 months, and then monthly follow-ups. Stage 4 operates by protocol to include intensive obesity treatments, such as pharmacotherapy and bariatric surgery.13,14 Also, weight management interventions should provide at least 26 contact hours over 6 months for children 6 years and older. 15 Given the high prevalence of childhood obesity, there is an urgent demand to find reliable telehealth solutions for pediatric weight management treatment.16,17 Without such interventions, the burden of this pandemic will be exacerbated. 16
The evidence is mixed regarding the treatment of children and adolescents with obesity via telehealth.13,18–20 A previous review on the efficacy of telehealth weight management interventions for pediatric obesity found telemedicine to be a potential avenue for expanded obesity treatment. 13 Nguyen et al. showed promising outcomes on dietary changes and physical activity using telehealth. 20 However, a parent-focused weight management literature review revealed no significant difference in BMI or BMI z-score between the control groups and the telehealth participants. 19
As telehealth is becoming popular in delivering weight management interventions, examining its effectiveness compared with a face-to-face modality is of clinical significance. 21 In the literature, telehealth and telemedicine are used as synonyms and interchangeably. For this review, telehealth is defined as synchronous, real-time interactive communication between a patient and a physician or practitioner at a distant site through audio and visual telecommunication equipment.22,23 As such, this systematic review aims to examine the literature regarding the effectiveness of clinic-based telehealth vs. face-to-face interventions to combat obesity among children and adolescents. Efficacy was determined based on changes in measured child BMI (primary outcomes) and dietary and physical activity changes, as well as intervention feasibility and satisfaction with telehealth, as secondary outcomes.
Methods
Literature Search
This systematic review adhered to the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) protocol. 24 This systematic review did not require IRB review because the data used originated from database searches with no identifiable human subjects. The identity of the subjects in the reviewed manuscripts from whom the data originated was not identifiable. The electronic databases of PubMed, Medline, and CINAHL with full text were searched. Google Scholar was used to search for gray literature. Reference lists of relevant articles were scanned. The search incorporated both Medical Subject Headings (MeSH) and other key search terms used to locate articles.
The MeSH terms for population included overweight. Key search terms included: childhood obesity, pediatric obesity, childhood overweight, pediatric overweight, school-age obesity, adolescent overweight, adolescent obesity, and obesity. This was a combined “OR” search.
The intervention MeSH terms included pediatric/prevention and control, pediatric obesity therapy, diet, healthy, weight management program, lifestyle changes, or lifestyle modification. Key search terms included: health promotion, weight reduction programs, obesity prevention, obesity treatment, clinical interventions, diet intervention, dietary intervention, healthy diet, nutrition interventions, therapy, lifestyle choices, and primary health care. This was also a combined “OR” search.
Two separate term searches were conducted for comparisons, “telehealth” and “face-to-face.” MeSH terms for “telehealth” included office visits, ambulatory care, and telemedicine. Key Terms: telehealth, eHealth, mhealth, health technology, mobile health, mobile health applications, smartphone, computer, online, internet. This was a combined “OR” search. The MeSH terms for the “face-to-face” search included ambulatory care. Key Terms included: in person or face-to-face visit vs. online, in-person, in office, clinic visits, office visit, primary care visits, face-to-face office visits, primary care in office, in office clinic visit, and primary care face-to-face visit. This was a combined “OR” search.
Lastly, the MeSH terms for outcomes included Body Mass Index (BMI), weight loss, and weight reduction. Key Terms: Body Mass Index, BMI z-score, Body Mass Index z-score, body fat loss, health improvement, diet improvement, BMI reduction, reduce obesity, and reduce weight. This was also a combined “OR” search. Afterward, the searches were combined as an “AND” search, and articles were retried and reviewed.
Inclusion Criteria
Article inclusion criteria included studies published within the last 10 years and written in English. Types of participants were children with overweight or obesity (school-aged children 6–12 years and adolescents 13–18 years).25,26 Interventions included clinic-based weight management treatments for children and adolescents with overweight and obesity. Comparison interventions included face-to-face in-person visits vs. telehealth visits. Primary outcomes included improvements in BMI or BMI z-score and secondary outcomes included telemedicine feasibility, satisfaction, dietary intake, physical activity, and other biochemical indicators at baseline and postintervention. Inclusion criteria also included studies utilizing telehealth communication methods defined as synchronous, real-time interactive communication between a patient and a physician or practitioner at a distant site through audio and visual telecommunication equipment.22,23
Exclusion Criteria
Studies were excluded for being community-based interventions, age of participants younger than 6 years, older than 18 years, or primary focus of the intervention was another medical or underlying condition such as type 2 diabetes or Prader–Willi. Also, exclusion criteria included articles in which not all participants were overweight (BMI 85th–95th percentile) or obese (≥95th percentile) at the start of the intervention. Healthy weight children and adolescents, greater than the 5th percentile and ≤85th percentile, given that they are not expected to lose weight. 2 Exclusion criteria also included studies that utilized other technologies such as internet, text messaging, and social media.
Results
Study Selection
A database search generated a total of 1093 results. Articles were screened and eliminated based on duplications, study populations, and country. The remaining 1087 articles were assessed, screened, and eliminated based on titles and abstracts. A total of 32 articles remained for full-text review. Twenty-two articles were excluded for lack of comparison of telehealth visits with face-to-face and not being conducted in a clinical setting (Fig. 1). 24 Accordingly, 10 articles were included in this systematic review.27–36 Studies located within the search parameters were uploaded to EndNote used to manage studies.
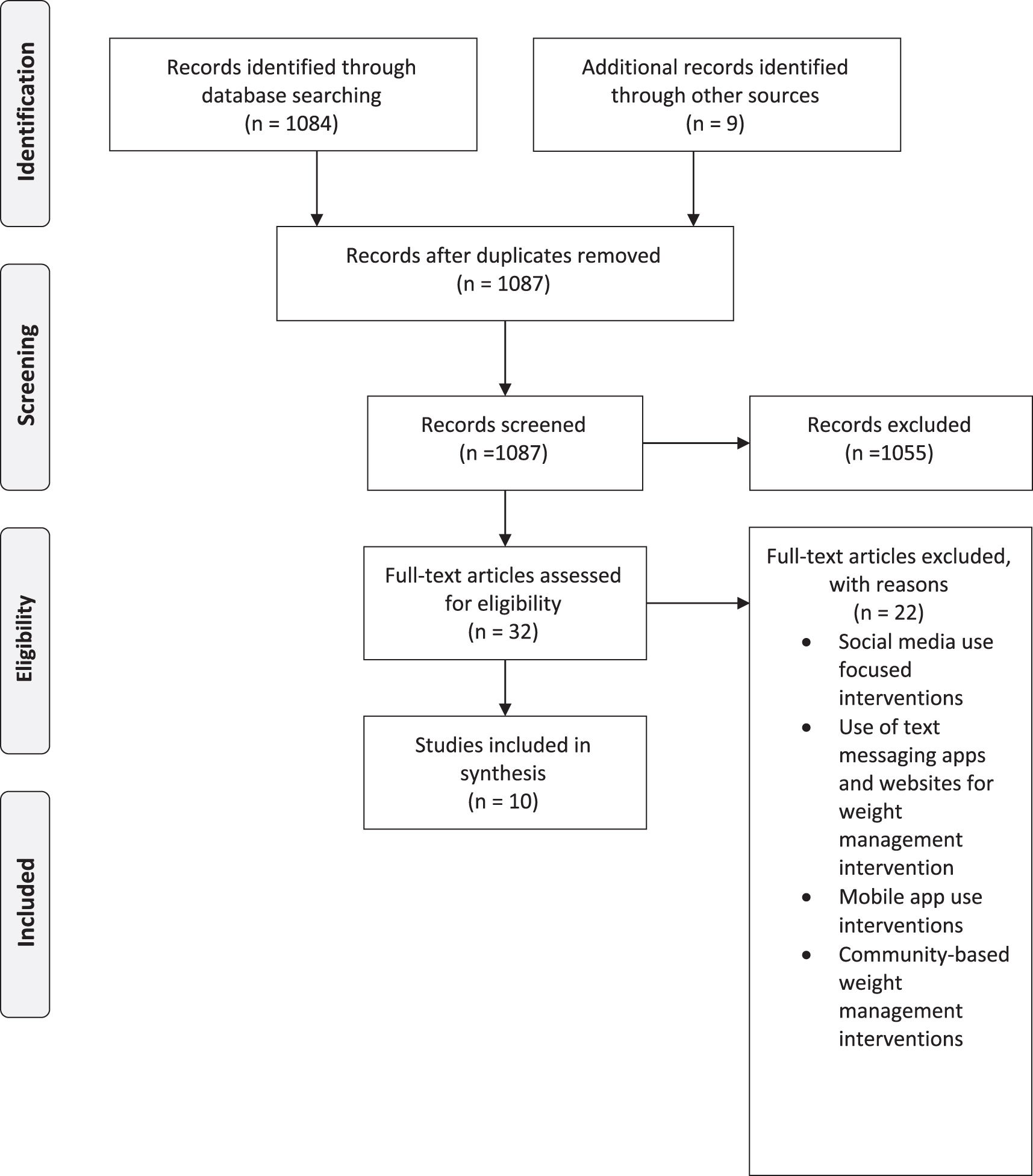
Flow diagram illustrating the literature search and study selection process.
Quality of Studies
The Study Quality Assessment Tool developed by the National Heart, Lung, and Blood Institute was used to assess study quality. 37 Quality was examined by study design; selection, performance, measurement, and attrition bias. Unique template checklists pertaining to observational and randomized control trials, case series, cohorts, pre-and-post studies as well as cross-sectional studies were utilized. A checklist, based on article type of between 8 and 14 items, was used to assess the evidence of outcomes of each study in which <60% score indicated low quality, 60%–90% score indicates moderate quality, and >90% score indicates high quality. Based on the evaluation checklists, the majority of trials in this review were rated moderate in quality. One article scored <60% indicating low quality. 27 Seven articles scored between 60% and 90% indicating moderate quality.28–34 Two articles scored high quality above 90%.35,36
Characteristics of Studies
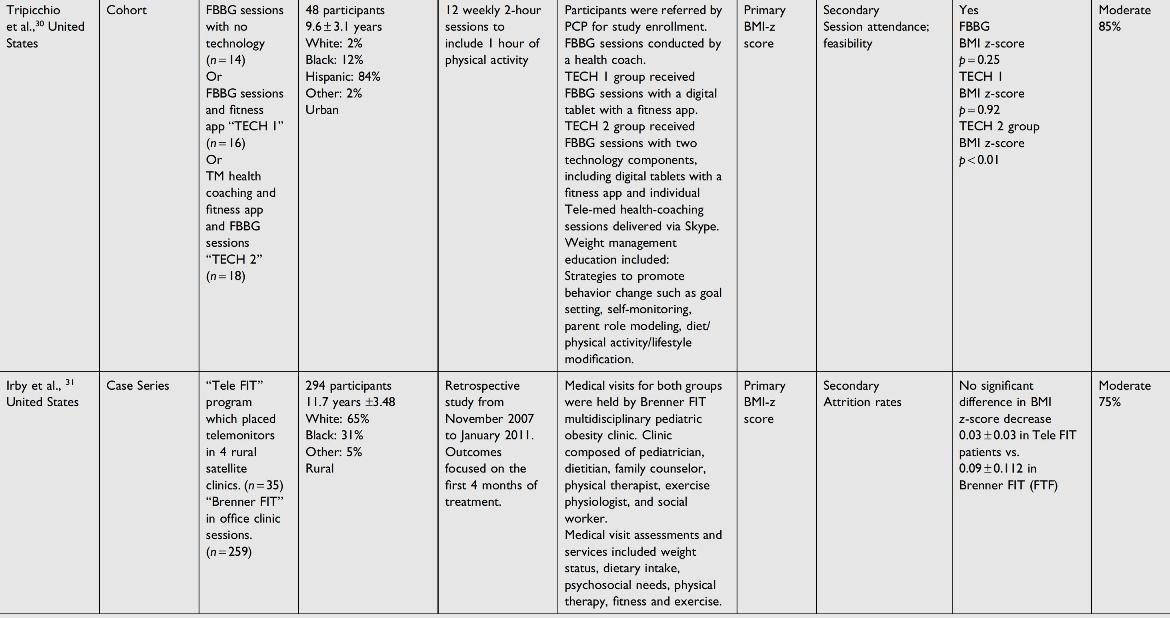
The characteristics of the studies meeting the inclusion criteria are presented in Supplementary Table S1 and Table 1. Ten studies met the inclusion criteria: 9 in the United States and 1 in Canada. The participants in all studies were children and adolescents with overweight and obesity, ranging from 8.5 to 14.3 years.27–36 Two studies conducted in the United States had intervention durations of 3 months or less, and eight studies, including one in Canada, had interventions of at least 6 months or longer.27–36 Participants included a range of cultural and ethnic groups, including Caucasian, African American, and Hispanic. All studies included both urban and rural demographics and were clinic-based outpatient obesity treatment interventions comparing telemedicine with face-to-face visits.27–36 Eight studies assessed primary outcomes as BMI/BMI-z scores.27–31,34–36 In addition, all studies evaluated secondary outcomes, including dietary intake, physical activity changes, telemedicine feasibility, blood pressure, waist circumference, and triceps skinfold, and one study observed a change in screen time.27–36
Characteristics of Included Studies
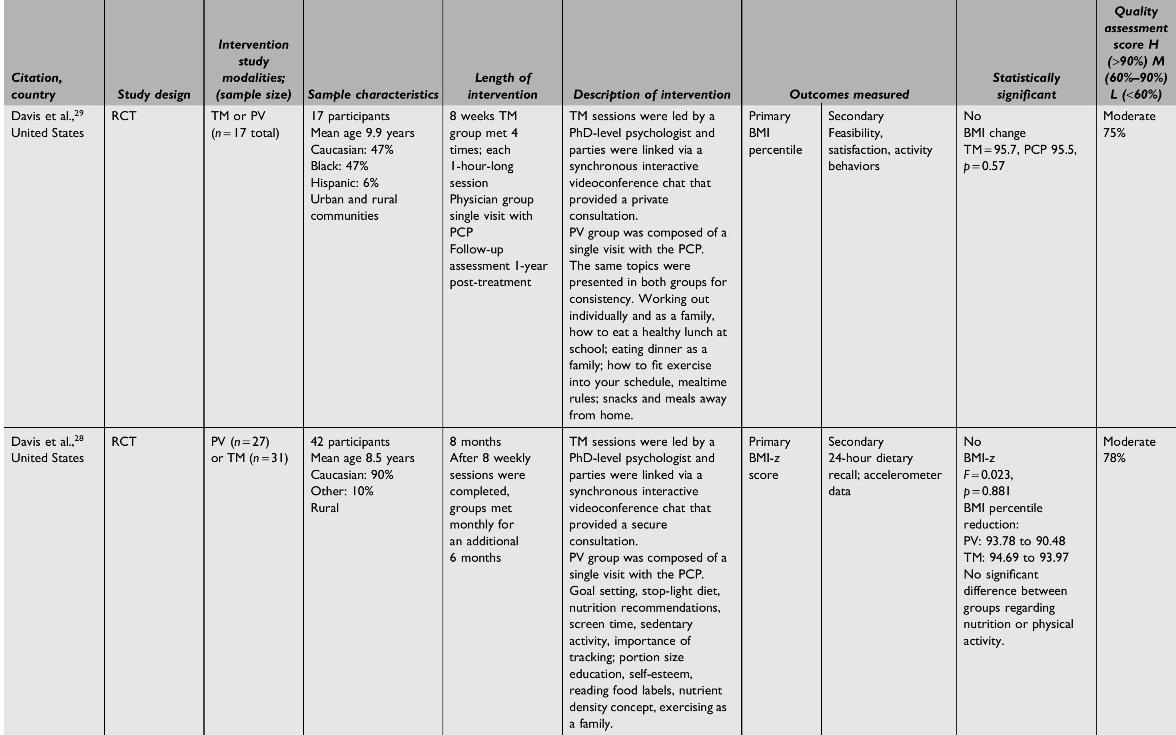



Mean ± SD age shown when reported.
FBBG, Family Based Behavioral Group; FIT, Families in Training; FTF, face-to-face; PCOS, polycystic ovary syndrome; PCP, primary care physician; PV, physician visits; RCT, randomized-controlled trial; TM, telemedicine.
Primary Outcomes
BMI/BMI z-score
Most studies found that both telehealth and face-to-face modalities combined and as stand-alone interventions were equally effective in improving obesity outcomes among children and adolescents.28,29,33–35 Lipana et al. found that the telemedicine group was more successful overall in weight outcomes as participants reported being more motivated to receive interventions, due to being located in a rural community. 27 One study found face-to-face intervention to be more effective than telehealth in reducing BMI percentile. However, BMI z-score outcomes were not statistically different between the groups. 29
Secondary Outcomes
Nutrition and physical activity
Lipana et al. reported more improvements in reducing obesity as demonstrated via an enhancement in nutrition, physical activity, and screen time for telemedicine participants than face-to-face. 27 Another study found that dietary intake (assessed based on dietary glycemic load) was significantly different from baseline in the combined telehealth and face-to-face intervention group. However, physical activity did not change throughout the study in either group. 35 One study found no significant difference between groups for improving nutrition or physical activity. 29
Telemedicine feasibility and satisfaction
Overall, there was no significant difference in satisfaction scores between telemedicine and face-to-face weight management interventions.27,31,35 However, study participants in both rural and urban areas found telemedicine to be more feasible and convenient.27,31,35 Davis et al. found that 100% of participants attended all telehealth sessions and reported being “very satisfied” or “highly satisfied” with telehealth attributes. 28 Tripicchio et al. asked participants to rate their experience on how helpful telehealth sessions were in achieving behavior change. All participants reported being “very satisfied” or “extremely satisfied” with telehealth and would highly recommend the online sessions to other families. 30
In addition, providers and researchers noted that telemedicine is effective in using clinician's skill set and time, helping avoid patient travel from underserved areas to clinic and satisfaction in using the equipment.32,33 Importantly, in two of the studies, families were satisfied with the telemedicine innovative approach and accepted using telehealth for treatment.29,30
Discussion
Findings in this review suggest that both telehealth and face-to-face weight management interventions for children and adolescents reduce obesity; however, the evidence is lacking in which modality is more effective. While few studies were found on this topic and are limited in scope, sample size, and outcomes, they show promise as a potential avenue for further research.
Telehealth is becoming the norm in providing pediatric weight management treatment. 21 This modality can help improve access to care in rural communities and those in disproportionately burdened populations.16,38 Although telehealth is an effective treatment for pediatric obesity, this review finds it does not replace face-to-face visits. Face-to-face intervention helps build rapport and improve obesity outcomes as it removes some obstacles related to telehealth. 13 A review of the literature suggests considerations for a hybrid model as it may be beneficial as clinics continue social distancing practices.16,21,39 Face-to-face clinic visits with an adjunct telehealth component can help bridge the gap between initial treatment and ongoing follow-up.40,41 This model potentially could leverage telehealth for additional check-in appointments during or after program completion and improve show rates helping to sustain BMI and BMI z-score reduction.40,41 However, virtual challenges need to be addressed to maximize its effectiveness in reducing pediatric obesity.12,16,38
Concerns including digital technology disparities in lower income households, and virtual approaches to meet the patients' social and linguistic needs should be considered as this can become a potential barrier to care.16,42 Also, identifying platforms that safeguard security and meet privacy regulations can better facilitate virtual visits for nutritional care and improve collaboration among practitioners. 16 Furthermore, consideration should focus on telehealth pay or reimbursement as it affects program development and continuation. 38 These challenges, if unaddressed, can potentially widen obesity disparities, leaving this population at high risk for morbidity and mortality.16,38
This review did not examine the efficacy of the recommended guidelines for weight management treatment of pediatric obesity.14,15 Ensuring pediatric weight management interventions incorporate the recommended obesity treatment guidelines, including duration time, has been shown to improve outcomes in this population.14,15,40,43 While this review did not examine the literature on effective post-treatment weight management modalities, evidence suggests that a post-treatment protocol can help ensure the well-being of children through helping maintain obesity reduction benefits long term.39,41
It is recommended that future research comparing the efficacy of various technological modalities (i.e., smartphones, websites) for childhood obesity treatment be conducted as interventions are evolving. 20 More rigorous trials are needed to identify effective ways to deliver fully or mostly virtual interventions that promote retention, adherence, and healthy weight.13,16 Also, valid and reliable methods to objectively monitor cardiometabolic health and weight outcomes in children remotely are needed. 16 While all the studies in this review did include family involvement,27–36 more studies that compare different types and levels of family involvement related to various cultures, ethnicities, and backgrounds may be an important next step in research as well.44,45
Lastly, this review did not target the young childhood age group. Early childhood is the ideal stage of life to intervene in the prevention of childhood obesity. 46 It is recommended that research be conducted regarding prevention interventions as healthy lifestyle practices can be introduced at a younger age, rather than attempting to change unhealthy habits in older age groups.46,47 Overall, this review highlights the preliminary work in this area, thereby identifying a potential outlet for future clinical practice and investigation.
Strengths and Limitations
This review followed the recommendations for rigorous systematic review methodology. No country filters were applied to the literature searches. Four databases were used to include capturing gray literature ensuring a comprehensive search was undertaken. The quality of evidence of included studies was evaluated using the Study Quality Assessment Tool developed by the National Heart, Lung, and Blood Institute utilizing unique templates for evaluation. This increased the transparency of the quality of studies included.
However, there are limitations in this review. One of the limitations is applying a language filter. Authors reviewed only articles written in English due to a lack of translation resources. Another limitation is the limited number of studies included in this review. Interventions were limited to developed countries (the United States and Canada), although no country filters were applied in the search strategy. In addition, this review included nonrandomized-controlled trials (RCTs) due to the limited number of studies, specifically RCTs, found on telehealth pediatric weight management. This finding highlights the need for additional rigorous studies to address the shortcomings and establish evidence-based guidelines that can translate into clinical practice to manage obesity among children.
However, with the current COVID-19 pandemic and the increased use of telehealth in counseling, there is a likelihood for more opportunities to conduct rigorous research studies for obesity treatment via telehealth. Also, the results from this systematic review should be taken in the context of included countries as telehealth use in developed and developing countries may vary. In addition, the studies included in this review encompassed the years 2011–2018 when telehealth and the related technology were still in their infancy. However, the COVID-19 pandemic brought telehealth into the mainstream for patients, families, providers, and health systems 16 ; thus, there is more likely to have more robust weight management interventions using telemedicine and more rigorous study designs in the coming years.
In addition, this review excluded studies involving young children and community-based weight management interventions. Overall, there were a small number of articles found with varying aims of interventions. Furthermore, one reviewer did the screening and the quality appraisal of articles; this may have resulted in excluding potentially relevant studies. Also, the minimum follow-up period for included studies was either not precise or completed. As such, the results should be taken in the context of the specified intervention duration as 3 months weight management intervention or less is insufficient to measure change and/or maintenance in weight-related outcomes.
Conclusion
This systematic review found the evidence insufficient regarding the most effective modality to treat childhood obesity between clinic-based face-to-face and telehealth visits. All studies included examined weight management treatment interventions for school-aged children and adolescents conducted via face-to-face office visits or synchronous telehealth.27–36 While this review examined the efficacy of obesity interventions in children and adolescents, the growing prevalence reaffirms the importance of further research and practice implications for obesity treatment. 48 Hybrid weight management interventions that combine successful components of face-to-face and telehealth may be key in reducing childhood obesity and sustaining weight-loss outcomes post-treatment in this population.19,39 However, clinics should address digital technology disparities and internet privacy concerns before telehealth implementation. 16 This review suggests that telehealth combined with face-to-face interventions, may, with further research, positively impact weight-related outcomes in children and adolescents. It is recommended that future research and clinic-based weight management interventions target not only school-aged children and adolescents but the younger population as well.
Footnotes
Authors' Contributions
A.W. searched databases, extracted data, assessed the quality of articles, and drafted the article. A.W. and N.Y. participated in the (population, intervention, control, and outcomes) PICO format question, search strategy, and the structure of the review. N.Y. critically revised the drafts and edited the article.
Acknowledgment
Authors would like to thank Ms. Margaret Danowski, MLIS, Assistant Professor, Library Research & Instruction Services, Health Professions Librarian and Interim Art & Design Librarian, Central Michigan University Libraries, for assistance in database search strategy.
Ethical Standards Disclosure
No need for ethics approval.
Funding Information
No funding was received for this article.
Author Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.