
Abstract
Background:
Performance of vibration-controlled transient elastography (VCTE) is inadequately validated in pediatric nonalcoholic fatty liver disease (NAFLD). We aimed to assess the technical performance of VCTE in pediatric NAFLD and define the agreement between VCTE and reference standards of imaging and/or biopsy.
Methods:
This prospective study recruited participants with known or suspected NAFLD who underwent a research VCTE examination (FibroScan Mini 430). Ten valid VCTE liver stiffness measurements (kPa) and controlled attenuation parameter (CAP) (dB/m) measurements were obtained for each participant. Available clinically acquired MR elastography and magnetic resonance imaging proton density fat fraction (PDFF), liver ultrasound shear wave elastography, and biopsy served as references standards.
Results:
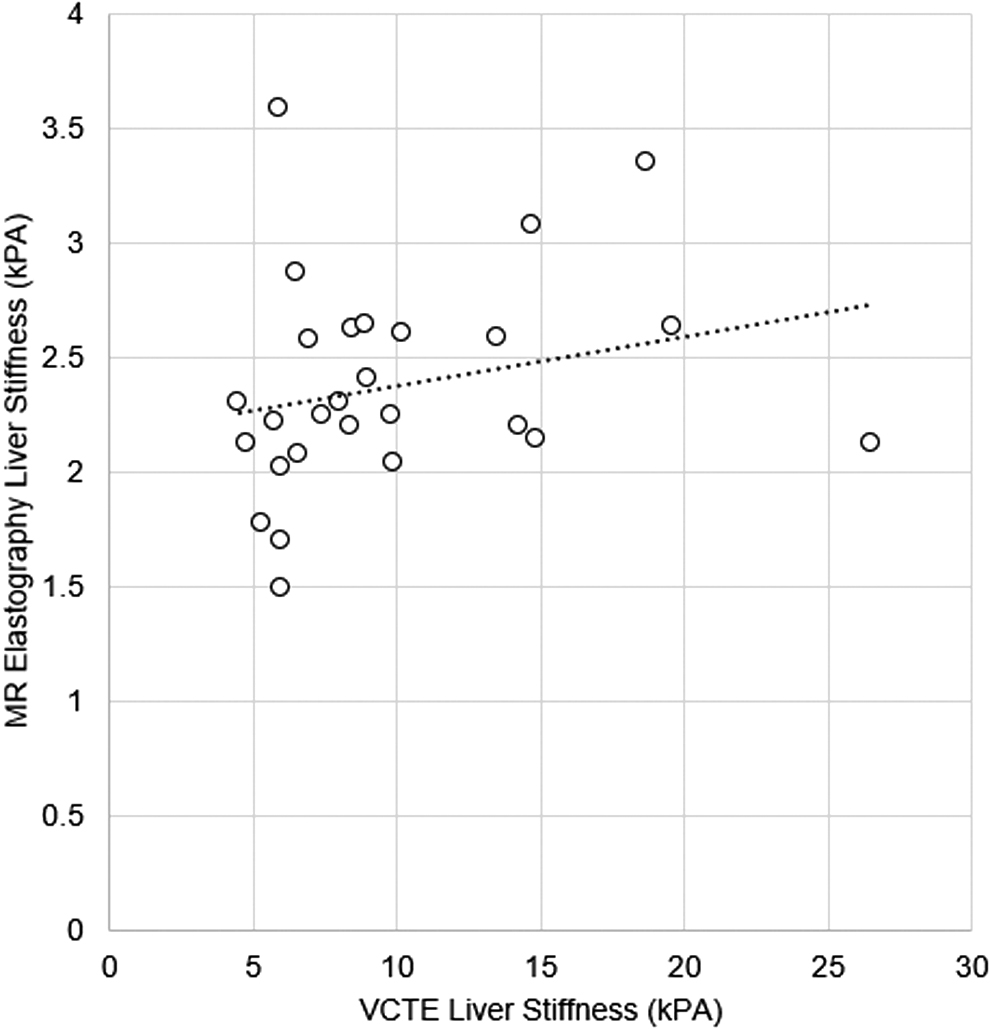
Eighty-four consecutive participants were included (55 males, mean age 15.0 ± 3.5 years, mean BMI 36.6 ± 9.4 kg/m2). VCTE examinations were complete in 80/83 participants. 37/83 participants were examined with an XL probe. There was no significant correlation between CAP and PDFF [n = 16; r = 0.17 (95% confidence interval [CI]: −0.34 to 0.61), p = 0.5] or between VCTE liver stiffness and MR elastography stiffness [n = 27; r = 0.31 (95% CI: −0.07 to 0.62), p = 0.10]. For prediction of any fibrosis stage ≥1 on biopsy (n = 9/15 participants), VCTE median liver stiffness >5.1 kPA had an area under receiver operating characteristic curve of 0.52 (95% CI: 0.26–0.78) with a sensitivity of 88.9% and specificity of 16.6% (p > 0.99).
Conclusions:
Complete VCTE examinations could be obtained in most pediatric patients with NAFLD. Neither VCTE liver stiffness nor CAP correlated well with measures of liver fat or stiffness by established imaging modalities and biopsy.
Introduction
Currently, nonalcoholic fatty liver disease (NAFLD) is the most common cause of chronic liver disease in children. 1 In some patients, NAFLD may lead to worsening fibrosis, and can even progress to cirrhosis during adolescence. While liver failure due to NAFLD is rare in childhood, NAFLD is the fastest rising indication for liver transplantation in young adults.2,3 Noninvasive imaging methods are increasingly used to evaluate chronic liver disease.4–7 Imaging methods that have been used to evaluate pediatric NAFLD include vibration-controlled transient elastography (VCTE) liver stiffness and controlled attenuation parameter (CAP), ultrasound shear wave elastography (SWE), ultrasound attenuation and backscatter, MR elastography, and magnetic resonance imaging (MRI) liver proton density fat fraction (MRI-PDFF). 8
FibroScan® (Echosens, Paris, France) is an FDA-approved, point-of-care ultrasound technique that uses transient elastography to measure liver tissue stiffness (in kilopascals) and simultaneously provides a measure of the CAP. 9 Liver stiffness has been linked to histologic fibrosis severity, 1 and the CAP has been linked to histologic liver steatosis severity. 10 These techniques have increasingly been implemented in pediatric clinics evaluating youth with liver disease, despite limited validation. Thresholds for abnormal liver stiffness and attenuation indicative of steatosis in children and adolescents with NAFLD are inadequately defined, due to a paucity of studies comparing VCTE and CAP to liver biopsy and other noninvasive imaging modalities in pediatric populations with NAFLD. 11
The primary purpose of our study was to assess the technical performance of VCTE and the CAP in a prospective real-world pediatric cohort with known or suspected NAFLD, including patients with severe obesity. Secondarily, we aimed to determine the agreement between VCTE or the CAP and the clinical reference standards of liver MRI and/or biopsy.
Methods
This was a prospective cross-sectional study that was approved by the Institutional Review Board at Cincinnati Children's Hospital Medical Center. All research activities were conducted in a Health Insurance Portability and Accountability Act compliant manner. Written informed consent was obtained in person from participants ≥18 years of age and from guardians of participants <18 years of age. In addition, written assent was obtained from participants 11–17 years old.
Participants were recruited as a convenience sample between September 2020 and May 2021 at a single pediatric academic medical center (Cincinnati Children's Hospital Medical Center; Cincinnati, OH). Outpatients (between the ages of 2–23 years old) presenting for evaluation at a fatty liver disease clinic or presenting for clinically indicated ultrasound or MR elastography examinations of the liver for suspected fatty liver disease were prospectively recruited. Inclusion criteria consisted of suspected or presumed NAFLD. Suspected NAFLD was defined as a patient with overweight/obesity and chronically elevated liver enzymes and/or imaging evidence of hepatic steatosis. Presumed NAFLD was defined as a patient with hepatic steatosis that has undergone testing, which has excluded other causes of liver disease.
Exclusion criteria included nonfasting status (minimum of at least 2 hours since last oral intake as postprandial stiffness values have been shown to return to baseline levels within 120 minutes after meal intake),12,13 known ascites, active medical device implant, inability to cooperate with the VCTE examination, and pregnancy.
Research VCTE Examinations
VCTE and CAP examinations were performed by one of two FibroScan-certified technicians (M.D. [author], M.M. [non-author]) using a FibroScan Mini 430 (Echosens) with M or XL probes. The XL probe is not labeled for use in patients <18 years of age. Its use in this study is investigational. Technicians were blinded to clinical data when obtaining VCTE measurements. For participants <18 years of age, thoracic circumference was measured, and if ≤75 cm, the examination was not performed as the manufacturer recommends the S1 or S2 probes in patients this size. For participants <18 years old with a thoracic circumference >75 cm and for participants ≥18 years of age, the examination was begun using the M probe.
At examination start, the FibroScan Automatic Probe Selection measured the skin-to-liver capsule distance (SCD) and recommended a switch to the XL probe if the SCD was ≥2.5 cm. Repeated measurements were performed during suspended respiration until 10 valid values (indicated by the device) for liver stiffness (kPa) and CAP (dB/m) were obtained, with an interquartile range (IQR)/median of <30%. Any measurement in a nonliver area was automatically invalidated by the device. Specific VCTE protocol details are provided in Supplemental Material (online).
The following measures were recorded: thoracic circumference if <18 years of age, automated probe selection (M or XL), number of valid and total measurements (valid + invalid), stiffness IQR/Median, and time required to perform each examination. The frequency of technically successful examinations (defined as a ratio of valid:total measurements ≥60%), and incomplete examinations (10 valid measurements unable to be obtained within 15 minutes) were also recorded. 5
Medical Record Review
Clinically acquired liver MR elastography and proton density fat fraction (PDFF), and liver ultrasound SWE, performed as previously described14–16 and liver biopsy results were extracted from the electronic medical record (Epic, Verona, WI). Measures relevant to fibrosis were recorded if within 1 year of the research transient elastography examination, as liver fibrosis generally progresses slowly in children with NAFLD. 3 Measures relevant to steatosis were recorded if within 3 months of the research transient elastography examination, to maximize stability of measurements. Liver profile laboratory data within 1 year of VCTE were also recorded with AST to platelet ratio index (APRI) retrospectively calculated for this study based on clinical laboratory data. 17
Statistical Analysis
For performance analysis of VCTE, liver stiffness >5.1 and 7.4 kPa were considered indicative of fibrosis stage ≥1 and ≥2, respectively, 5 and CAP >249 dB/m was considered indicative of steatosis grade ≥1. 11 Clinically acquired MRI and biopsy served as reference standards. For MRI, a liver shear stiffness of >2.8 kPa and a liver PDFF >5% were considered abnormal. 18 For biopsy, fibrosis stage and steatosis grade were scored according to the Nonalcoholic Steatohepatitis Clinical Research Network scheme. 16 Fibrosis stage ≥2 was considered clinically significant. 16 We additionally assessed agreement with liver ultrasound SWE (secondary analysis) with a shear wave speed (SWS) >1.56 m/s considered abnormal. 14
Participant demographics and clinical characteristics, VCTE, MRI, and biopsy, measures were summarized using means, medians, standard deviations, and IQRs, as appropriate. Stiffness and steatosis measures were analyzed as continuous and categorical (normal vs. abnormal) outcomes. Pearson correlation (r) was used to assess univariate associations between variables. The Kruskal–Wallis test was used to compare medians between categorical biopsy scores and VCTE measures. Paired t-tests were used to compare means between groups. Two by two tables were constructed to calculate sensitivity and specificity of VCTE compared to reference standards. All analyses were performed with MedCalc Statistical Software version 20.009 (MedCalc Software Ltd, Ostend, Belgium). A p-value <0.05 indicated a statistically significant difference.
Results
We enrolled 84 consecutive participants, 55 (65%) male and 29 (35%) female. One participant (age 11, male) was excluded due to a thoracic circumference ≤75 cm, resulting in an analysis sample of 83 unique participants (Table 1). Examinations were incomplete in 3/83 participants, ages 15, 15, and 19 years, two of whom were males. Incomplete examinations were due to >15 minute acquisition time in two participants (one with obesity class II and one with obesity class III) and equipment malfunction in one participant.
Study Sample Demographics and Summary Statistics for Liver Transient Elastography, Controlled Attenuation Parameter, Magnetic Resonance Imaging, Ultrasound, and Biopsy
Biopsy was scored according to NASH Clinical Research Network Scoring System. 14
ALT, alanine aminotransferase; APRI, AST to platelet ratio index; AST, aspartate aminotransferase; CAP, controlled attenuation parameter; GGT, gamma-glutamyltransferase; MRI, magnetic resonance imaging; NA score, NAFLD Activity score; PDFF, proton density fat fraction; SD, standard deviation; SWE, shear wave elastography; VCTE, vibration-controlled transient elastography.
Performance of VCTE
Complete liver stiffness and CAP examinations were obtained for 80/83 participants (96%; mean age 15.0 ± 3.5 years, mean BMI 36.6 ± 9.7 kg/m2). A majority (94%, 78/83) of the sample had obesity (BMI percentile-for-age ≥95th, if <20 years, or BMI >30 kg/m2 if ≥20 years of age) with 45% (38/83) meeting criteria for obesity class 1, 20% (16/83) class 2, and 29% (24/83) class 3, using pediatric criteria. 19 Among the 80 participants with completed examinations, 43 (53%) were examined with an M probe and 37 (47%) with an XL probe. Of the 37 participants requiring an XL probe, 81% (30/37) were <18 years of age. In the subset of participants <18 years of age with complete examinations (n = 64/80), the XL probe was recommended by the automatic probe selection tool in 47% (30/64).
Examinations were technically successful for 66% (53/80) of participants, as defined as a ratio of valid:total measurements ≥60%. There was no difference in BMI between participants with technically successful (mean = 35.6 ± 7.8 km/m2) vs. unsuccessful (mean = 38.7 ± 12.8 km/m2) examinations, p = 0.17. Similarly, no difference was seen in thoracic circumference (mean for unsuccessful = 108.6 ± 28.6 cm, mean for successful = 112.0 ± 16.5 cm, p = 0.50) or type of probe (M vs. XL), p > 0.99.
Comparison of VCTE With MRI, US, and Histology Assessments of Liver Severity
A total of 28 MRI examinations, 12 SWE ultrasound examinations, and 15 liver biopsies were performed within 1 year of the research VCTE examination and were used for stiffness comparisons; 16 MRI examinations and 6 liver biopsies were performed within 3 months of the research examination and were used for steatosis comparisons.
Univariate Associations Between Imaging Measures: Liver Stiffness, CAP, MRI, and Ultrasound-SWE
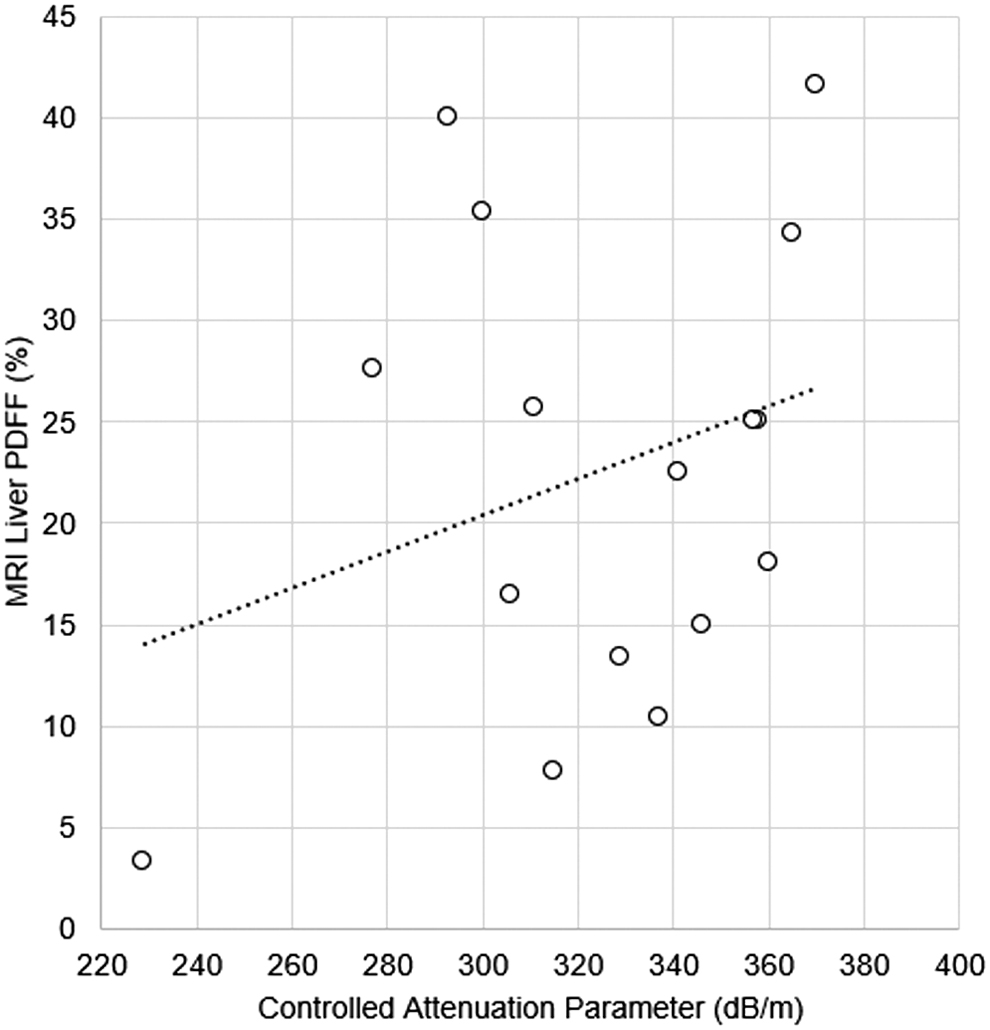
There was no significant correlation between CAP and MRI-PDFF [n = 16; r = 0.17 (95% confidence interval [CI]: −0.34 to 0.61), p = 0.5] at a median interval of 41.5 days (IQR: 5.25, 74.25) between examinations (Table 1 and Fig. 1
Univariate Associations Between VCTE Measures and Liver Biopsy Measures
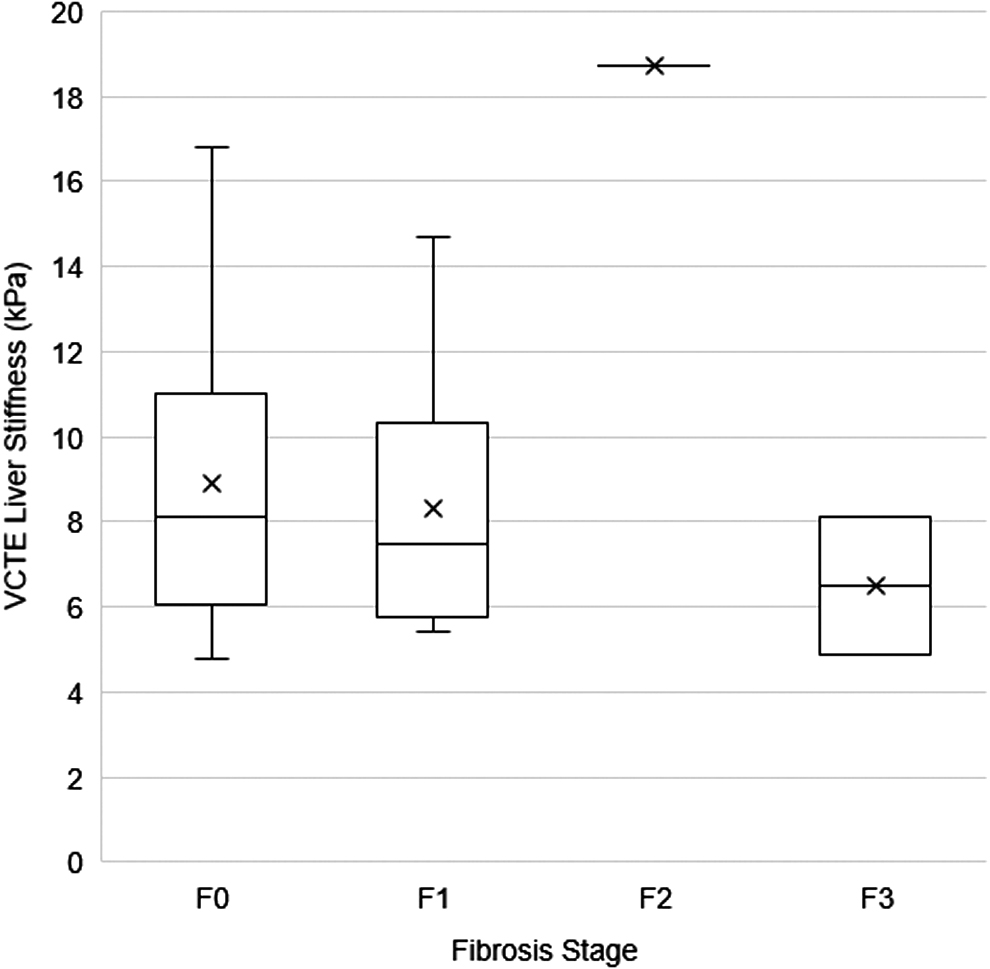
The median interval between liver biopsy and CAP measurement was 45 days (IQR: 34, 83) and between biopsy and VCTE was 151 days (IQR: 73, 207). When biopsy scores were analyzed as continuous measures, mean of median CAP and biopsy steatosis score did not significantly correlate [n = 6; r = 0.39 (95% CI: −0.61 to 0.91), p = 0.44] nor did mean of median liver stiffness by VCTE and biopsy fibrosis stage [n = 15; r = −0.04 (95% CI: −0.54 to 0.47), p = 0.86]. Similarly, when biopsy results were treated as categorical variables, CAP did not significantly differ by steatosis grade (p = 0.32) (Fig. 4) nor did liver stiffness by VCTE by stage of liver fibrosis (p = 0.15) (Fig. 5).

Univariate Associations Between VCTE and Laboratory Data
There was weak correlation between liver stiffness by VCTE and serum gamma-glutamyl transferase [n = 68; r = 0.25 (95% CI: 0.01–0.42), p = 0.03] at a median 5 day (IQR: 0, 87) interval, and between liver stiffness by VCTE and alanine aminotransferase levels [n = 71; r = 0.25 (95% CI: 0.02–0.46), p = 0.03] at a median 3.5 day interval (IQR: 0, 56.5). There was no significant correlation between liver stiffness by VCTE and APRI [n = 61; r = 0.19 (95%CI: −0.05 to 0.42), p = 0.12]. There was no significant correlation between CAP and APRI [n = 49; r = 0.41 (95% CI: −0.17 to 0.39), p = 0.41] or alanine aminotransferase levels [n = 58; r = 0.20 (95% CI: −0.06 to 0.43), p = 0.37].
Diagnostic Performance of VCTE for Categorical Prediction of Abnormal MRI or Ultrasound
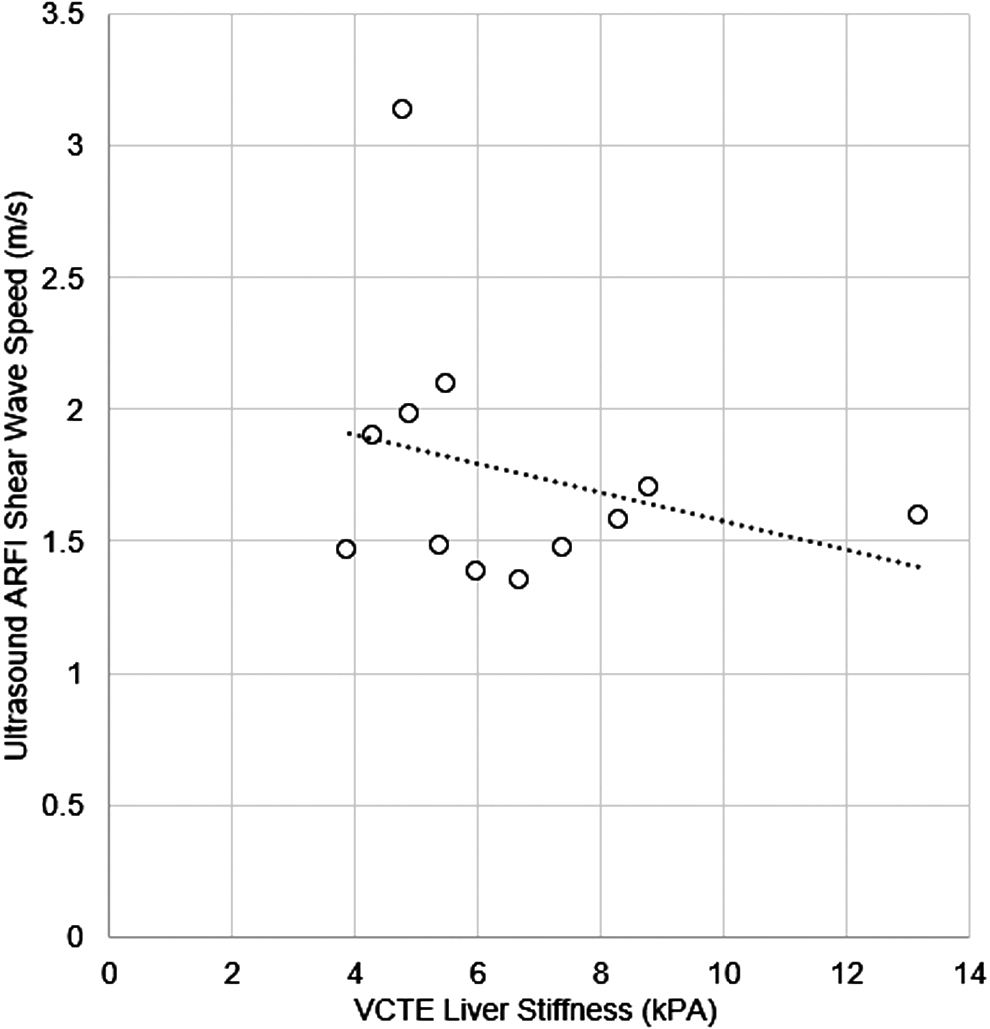
For prediction of liver PDFF >5%, median CAP >249 dB/m had an area under receiver operating characteristic curve (AUROC) of 1.0 (95% CI: 0.79–1.0) with sensitivity and specificity of 100%, but with a nonsignificant p-value (p = 0.06) (Table 2). For prediction of a liver MRI shear stiffness >2.8 kPA, VCTE liver stiffness >5.1 kPa had an AUROC of 0.57 (95% CI: 0.37–0.76) with sensitivity of 15% and specificity of 100% (p > 0.99). For prediction of ultrasound liver SWS >1.56 m/s, VCTE liver stiffness >5.1 kPa had an AUROC of 0.38 (95% CI: 0.13–0.69) with sensitivity of 57% and specificity of 20% (p = 0.57) (Table 2).
Diagnostic Performance of Liver Vibration Controlled Transient Elastography and Controlled Attenuation Parameter Measures for Categorically Abnormal Magnetic Resonance Imaging or Ultrasound and for Prediction of Abnormal Steatosis and Fibrosis on Liver Biopsy
The MRI liver shear stiffness threshold of 2.8 kPA is based on the prior study by Trout et al. 18
The ultrasound liver SWS threshold of 1.56 m/s is based on the prior study by Alves et al. 14
Values not calculable due to small sample size.
AUROC, area under receiver operating characteristic curve; CI, confidence interval; NA, not applicable; SWS, shear wave speed.
Diagnostic Performance of VCTE for Categorical Prediction of Any and Significant Fibrosis on Biopsy
For prediction of fibrosis stage ≥1 (n = 9/15 participants), VCTE median liver stiffness >5.1 kPa had an AUROC of 0.52 (95% CI: 0.26–0.78) with sensitivity of 88.9% and specificity of 16.6% (p > 0.99) (Table 2). For prediction of fibrosis stage ≥2 (n = 3/15 participants), VCTE median liver stiffness >7 kPa had an AUROC of 0.50 (95% CI: 0.23–0.76) with sensitivity of 67% and specificity of 33% (p > 0.99) (Table 2).
Discussion
Our study provides a real-world assessment of VCTE liver stiffness and the CAP in children and adolescents undergoing evaluation for confirmed or suspected nonalcoholic fatty liver disease. When performed by trained operators, VCTE performed with M or XL probes had a very low frequency (3.6%) of incomplete examinations (unable to obtain 10 valid measurements), but 34% of examinations were technically unsuccessful (ratio of valid:invalid measurements <60% 5 ) according to previously defined criteria. Of note, the mean number of measurement attempts required to obtain 10 valid measurements in our sample, the majority with obesity, was 20 (with a maximum of 80 measurements required in a single participant with class 3 obesity).
Choice of probe size is an important consideration for VCTE examinations. 20 In our study, the XL probe was automatically recommended by the device for nearly half of participants <18 years old, validating use of this probe for this age group, and highlighting the importance of obtaining regulatory approval for use in adolescents <18 years of age. Severe obesity is common among children in the United States, and limiting VCTE assessment to the M probe in this age group could result in inaccurate assessments of liver stiffness, due to increased SCD.3,21
In general, VCTE is considered to be feasible in most children with very low reported frequencies of incomplete examinations.4,22 Specific to children with fatty liver disease, our 3.6% frequency of incomplete examinations (inability to obtain 10 valid measurements) was lower than a recent study by Mandelia et al, who reported incomplete examinations in 10% (5/51) of their sample. Notably, BMI percentile was significantly higher among participants with failed examinations (p = 0.005) in their sample. 23 Our study suggests that technically unsuccessful examinations (valid:total measurements <60%) may also be more common in children with obesity, particularly those with severe obesity.22,23
Nobili et al reported only a 4% (2/52) frequency of technically unsuccessful examinations in their study of children with confirmed nonalcoholic steatohepatitis (NASH), both occurring in participants with BMI >35 kg/m2. 5 However, their sample had a reported mean BMI of ∼24–27 kg/m2 at mean age of 13–14 years, whereas our cohort had mean BMI of 37 ± 10 (mean BMI z-score 2.2) with mean age of 14.9 years.
In our study, liver stiffness measured by VCTE did not have a consistent relationship with liver stiffness measured by MRE or SWE. Likewise, predictive performance of VCTE for detecting a categorically abnormal MRE or SWE liver stiffness was only moderate (AUC = 0.57 and 0.38, respectively). 5 Results were similar when compared with biopsy staging of fibrosis, with VCTE liver stiffness having only moderate predictive performance for ≥ stage 1 fibrosis (AUC = 0.52, 89% sensitivity, 17% specificity). These results conflict with existing literature.1,24–26 Specifically, a meta-analysis of pediatric studies of VCTE reported a summary sensitivity of 95% and a specificity of 90% for the diagnosis of significant liver fibrosis (stage ≥2) when compared to biopsy. 27 It is important to note, however, that this meta-analysis included only two studies of pediatric cohorts with biopsy-confirmed NAFLD, both conducted at the same institution.
One of those studies was a prospective study of 52 participants with biopsy-proven pediatric NASH, which reported AUCs of 0.98, 0.99, and 1.0, for detection of “any” (>stage 1), significant (>stage 2), or advanced fibrosis (>stage 3), respectively. 5
The discrepancy between our results and those of this prior study may relate to our sample, including significantly more participants with obesity, which we believe resulted in a higher proportion of technically unsuccessful examinations. In our analysis, we included all completed examinations and did not exclude technically unsuccessful examinations, as we wanted to assess real-world performance. Different windows of biopsy data relative to VCTE (within 1 year in our study vs. 6 months in the cited study) and a smaller sample size with biopsy in our study might also explain the discrepancy.
We found no consistent correlation between CAP and liver MRI PDFF, or between CAP and liver steatosis grade on biopsy. In our AUROC analysis of abnormal CAP to predict an abnormal MRI PDFF, we found no significance, which may be explained by the lack of a non-NAFLD control group. In a pediatric study of 69 children with diverse liver diseases, Desai et al showed that CAP detected the presence of biopsy-confirmed steatosis with 87% sensitivity and 83% specificity, and AUC of 0.93 at a cutoff of 225 dB/m. 25
Similarly, when compared to MRI-PDFF, Runge et al and Shin et al showed CAP to have sensitivity of 75% and specificity of 75% at threshold of 277 dB/m, and sensitivity of 99% and specificity of 80% at threshold of 241 dB/m for the detection of steatosis.24,26 Of note, despite showing good binary diagnostic performance of CAP, Shin et al showed only moderate correlation between CAP and MRI PDFF (r = 0.49, p < 0.001) with no correlation in the subgroup of participants with BMI >30 kg/m2.
The strengths of our study are a larger sample size than previous pediatric VCTE cohorts and enrollment of a real-world cohort, which included a high proportion of participants with severe obesity. Our study is limited by the fact that MRI, US, and biopsy data were not available within prespecified intervals for all participants. Further, there is the potential that changes in inflammation activity over the interval between examinations impacted diagnostic performance.
In conclusion, our study demonstrates that while it is feasible to obtain complete VCTE and CAP examinations in most patients in a pediatric fatty liver disease clinic, technical concerns and gaps in validation remain that complicate interpretation. The lack of regulatory approval for the XL probe for patients <18 years of age could result in use of inappropriate probe size in many patients with severe obesity, potentially leading to inaccurate VCTE measurements. Finally, neither VCTE liver stiffness nor CAP correlated well with measures of liver fat or stiffness by other established imaging modalities or biopsy, highlighting the need for further prospective comparative studies to determine optimal implementation and integration of these modalities in clinical care and research.
Impact Statement
In a prospective study of 84 children and adolescents, most with obesity, vibration-controlled transient elastography was feasible to obtain, but its measures of liver stiffness and controlled attenuation parameter did not correlate well with measures of liver fat or stiffness defined by established imaging modalities and biopsy.
Footnotes
Acknowledgment
This study was presented as abstract in the Society for Pediatric Radiology Annual Meeting in 2022.
Authors' Contributions
V.P.V.A.: research analysis and interpretation; drafting and revising of article; approval of final version to be published; and agreement to be accountable for integrity of work. A.T.T.: research analysis and interpretation; drafting and revising of article; approval of final version to be published; and agreement to be accountable for integrity of work. M.D.: research acquisition; revising of article; approval of final version to be published; and agreement to be accountable for integrity of work. M.M.: research acquisition; revising of article; approval of final version to be published; and agreement to be accountable for integrity of work. A.C.A.-C.: research acquisition; revising of article; approval of final version to be published; and agreement to be accountable for integrity of work.
K.S.B.: research acquisition; revising of article; approval of final version to be published; and agreement to be accountable for integrity of work. J.R.D.: research analysis and interpretation; drafting and revising of article; approval of final version to be published; and agreement to be accountable for integrity of work. S.A.X.: research acquisition, analysis and interpretation; drafting and revising of article; approval of final version to be published; and agreement to be accountable for integrity of work.
Funding Information
Funded by own institution (Cincinnati Childrens Hospital Medical Center).
Author Disclosure Statement
J.R.D. has received unrelated research funding from GE Healthcare and Perspectum. A.T.T. has received unrelated research funding from Perspectum. A.T.T. and J.R.D. have received related investigator-initiated research funding from Canon Medical System and Siemens Healthineers. S.A.X. and M.M. have received unrelated research funding from Target RWE. No conflicts of interest to report: V.P.V.A., A.C.A.-C., K.S.B., and M.D.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.