
Abstract
The Editor-in-Chief of Childhood Obesity officially retracts the article entitled, “Body Mass Index and Gut Microbiome: A Cluster-Randomized, Controlled, Pilot Feasibility Study,” by Frenn M, Salzman N, Lam V, Holtz M, Moosreiner A, and Garnier M. (Child Obes. 2023 Feb 2 ahead of print. doi: 10.1089/chi.2022.0171).
After the Online Now (epub) publication of the paper, the Editor of the journal received an email from a reader with concerns regarding fundamental flaws in the study. The journal’s Editor-in-Chief provided this letter to the authors of the article and provided an opportunity to respond. The authors addressed several of the comments but defended their main analysis.
The Editor made the decision to retract the paper based on the following: (a) the distinction between a weakness or limitation in research vs invalid or incorrect methods is important; (b) weaknesses and limitations can be addressed by acknowledging them, whereas errors merit correction of the scientific record; and (c) the author response did not indicate that their original paper used correct and valid methods and it was therefore judged to be unreliable and meriting retraction.
The Editor-in-Chief of Childhood Obesity asked highly experienced statisticians to re-review the paper in conjunction with the complainant’s statements. The statisticians all are considered experts in their field and familiar with the issue being debated and have no affiliation or relationship with the complainants or the authors. After carefully examining the article, the statisticians agreed that flaws exist, most importantly that clustering and nesting should be accounted for in the statistical analysis given the cluster randomized design, thereby rendering the results biased and invalid.
Based on the statisticians’ assessments of the published article and the authors’ reanalysis, the Editor of Childhood Obesity is no longer confident in the results and, though the authors are not in agreement, officially retracts the article from the literature.
See the official Retraction Notice (10.1089/chi.2022.0171.retract) to view the original letter from the complainant, and the authors’ responses, which are included as supplemental material for clarity.
Introduction/Background
From 2017 to 2020, in, the United States, obesity prevalence was highest among Hispanic (26.2%) and non-Hispanic Black (24.8%) children and adolescents, which decreased with increasing family income. 1 Internationally, the prevalence in disadvantaged subpopulations may continue to increase, although patterns differ among countries. 2 The social determinant burden demands attention. 3
Altering gut microbiota with prebiotic fiber offers a potential intervention. Predominance of Firmicutes phyla vs. Bacteroidetes has been associated with higher body fat (BF) and BMI in adults 4 and children. 5 Prebiotic consumption was associated with growth of Bifidobacterium of the Actinobacteria phyla, while reducing the growth of Firmicutes. 4 When Canadian children with overweight/obesity were given the prebiotic fiber, oligofructose-enhanced inulin (OI), they had intestinal bacteria associated with reduced body mass z-scores, BF%, and serum triglycerides. 6 Conversely, Polish youth randomly assigned to 12 weeks of OI or placebo demonstrated no significant differences in body composition (BC). 7
More studies are needed examining the relationship of the gut microbiome with obesity in children. 8 Intake of a prebiotic plus calcium treatment sustained the BMI in youth with normal weight, limiting excess weight gain. 9 Calcium also acts as a prebiotic to foster gut microbiota found in animals with normal weight. 10 Further study combining prebiotic fiber plus calcium with physical activity (PA) and diet change was recommended to understand effects on gut microbiota. 11 High dietary fat (DF) has been associated with higher levels of Firmicutes (higher in those with obesity), while PA 12 has been associated with gut microbiota found with weight loss. 4
Although other factors such as structural racism and implicit bias may affect children with obesity,13,14 it is important to examine whether administration of a prebiotic fiber and calcium along with Project FUN, a culturally tailored online nutrition and PA program,15–17 is feasible and whether there are changes in stool microbiota and BC in groups at high risk for obesity.
Project FUN, an online Health Promotion/Transtheoretical Model intervention, has been shown to decrease intake of DF and increase PA among 4th- through 8th-grade, low- to middle-income, culturally diverse children.15–17 School settings offer a feasible and cost-effective opportunity to help children mitigate the risk of obesity.18–20
There is an urgent need to address the alarming rates of overweight and obesity in Hispanic and Black children.3,21 Therefore, it is important to examine whether African American and Latinx youth from low-income families respond to the prebiotic fiber with calcium and online intervention found beneficial in adults and predominantly Caucasian youth. It is also important to examine whether such an intervention is feasible and effective. Please see Figure 1 for the conceptual model guiding this study.
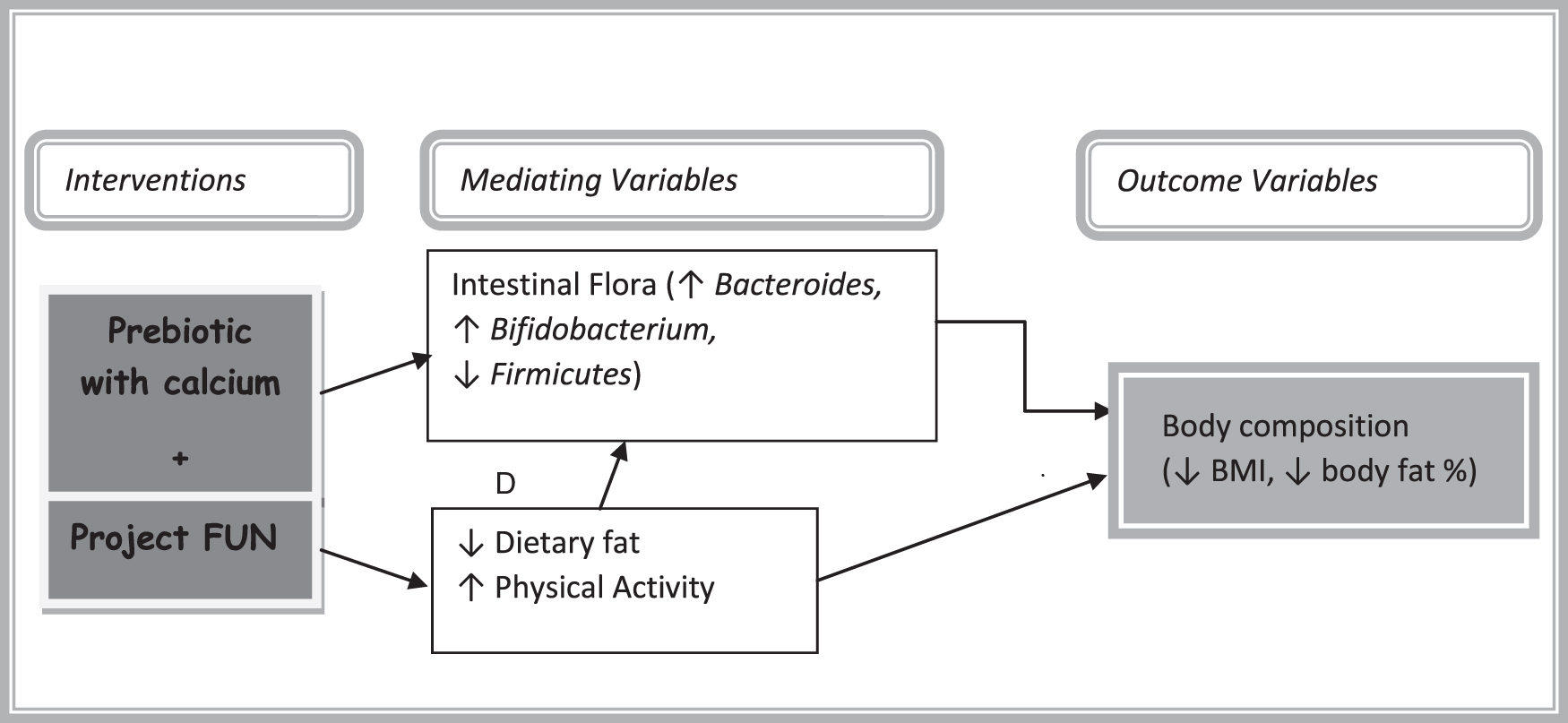
The objective of this study was to determine the feasibility, acceptability, and initial efficacy of combining the prebiotic and calcium treatment with Project FUN on BC and intestinal microbiota among 4th- and 5th-grade children whose social determinants placed them at higher risk for obesity. This aim was addressed through testing the following hypotheses:
Since this was a pilot, community-based efficacy study, the following feasibility, acceptability, and descriptive research questions were also addressed:
Methods
A cluster-randomized controlled trial (RCT) feasibility study was conducted to determine the level of participant engagement for future trials. Consenting participants were cluster randomized by classroom (seven intervention groups/five control groups). Research assistants (RAs) blinded to treatment conditions were trained and monitored by the principal investigator throughout the study.
Sample
The sample included 4th–5th-grade students at two private urban schools where 98% were eligible for free or reduced-fee lunch. The Wisconsin Private School Choice Programs allow children to attend private school if family income does not exceed established limits. 22 Of the 123 consenting participants, 56% were male; 71% Latinx; 15% African American; and 14% other. Three percent were with underweight; 49% with normal weight; 22% with overweight; and 25% with obesity.
Consenting Latinx (n = 20) and African American (n = 8) participants completed the microbiome analysis. Of these, 54% were male; 6.5% with underweight; 38.7% with normal weight; 32.3% with overweight; and 2.6% with obesity.
Measures
BMIp and BF% (measured with the Omron HBF-306C handheld bioimpedance monitor) were measured in privacy outside classrooms without shoes or jackets. Weights to the nearest tenth of a pound were collected using a Seca model 8761321004 scale. Heights in stocking feet were measured to the nearest 100th of an inch with a stadiometer (Seca Model 213, Hanover, MD).
BMIp was calculated using the school algorithm, including birth date, measurement date, height, and weight. 23 Four-point Quadscan bioimpedance and 24-hour diet recall were measured in a subgroup. Pearson's correlation between the handheld and 4-point bioimpedance measurements was n = 123, r = 0.73, p < 0.001. Bioimpedance is safe, convenient for BC analysis, and reliable, 24 with acceptable comparability with dual energy X-ray absorptiometry (DXA) in field studies. 25
Data were kept on a password protected computer using only participant ID.
DF% Self-Report
A 21-item, five-option response format, DF intake measure 26 was used. Internal consistency in this study for the total score was α = 0.86.
Physical Activity
The average of a two-item, 7-day PA measure 27 was used.
Microbiota
Stool sample collection was explained with written instructions (in English and Spanish) sent home with participants. Samples were returned at room temperature in sample containers and protective bags within FedEx paid mailers addressed directly to the laboratory. Genomic markers of stool samples were analyzed by Roche 454 pyrosequencing of fecal 16S rDNA and validated by quantitative polymerase chain reaction (PCR).
Procedures
The protocol was institutional review board approved. English and Spanish consent forms were explained by bilingual RAs to parents waiting for parent–teacher conferences and sent home with students. Parents denied their child had taken an antibiotic in the last month since antibiotics can change intestinal flora, although none required exclusion for this reason or for illness preventing participation. Students with parental consent then provided written assent in the fall of 2012.
Using a table of random numbers, classes were assigned to the intervention or usual school program (allocation not concealed). Both groups were measured before the intervention and after 12 weeks. Intervention group participants submitting stool samples received $5 pretest and $25 post-test gift cards.
The intervention group received OI, 4 g, twice/school day in 4 oz. of orange juice with calcium for 12 weeks, 9 starting in January 2013. We started with 1 g, then increased the next day by a gram to reach the 4-g dose. Although other prebiotic fibers could have been considered, this is one deemed generally considered safe by the US Food and Drug Administration.
Intervention group students completed Project FUN individually (password protected) in the school computer laboratory. Project FUN was used because it has been tailored and shown prior efficacy in the populations of interest as well as because fidelity to the intervention could be evaluated online and in workbooks.15–17 The control group participated in usual school activities, only completing pre- and postmeasures, although no stool samples were collected.
Analysis
Change scores were calculated for BC, DF, and PA for all participants. For intervention group participants submitting pre- and 12-week postintervention stool samples, DNA was isolated from stool samples, amplified, and barcoded. The 16S rRNA gene sequence analysis by 454 pyrosequencing was used. A single representative sequence was selected from each operational taxonomic unit, which was then assigned a taxonomic identity by comparison with the Greengenes 16S rRNA reference sequence databases 28 using a confidence level of 0.8 and the default assignment method (which is based on the Ribosomal Database Project classification system 29 ). Abundance of specific bacterial groups was determined by quantitative PCR.
Imputations for missing data were done with the R 30 package, mice, 31 and path analysis was used to analyze data. 32 Latent change scores were used to estimate the mean difference between time points. 33
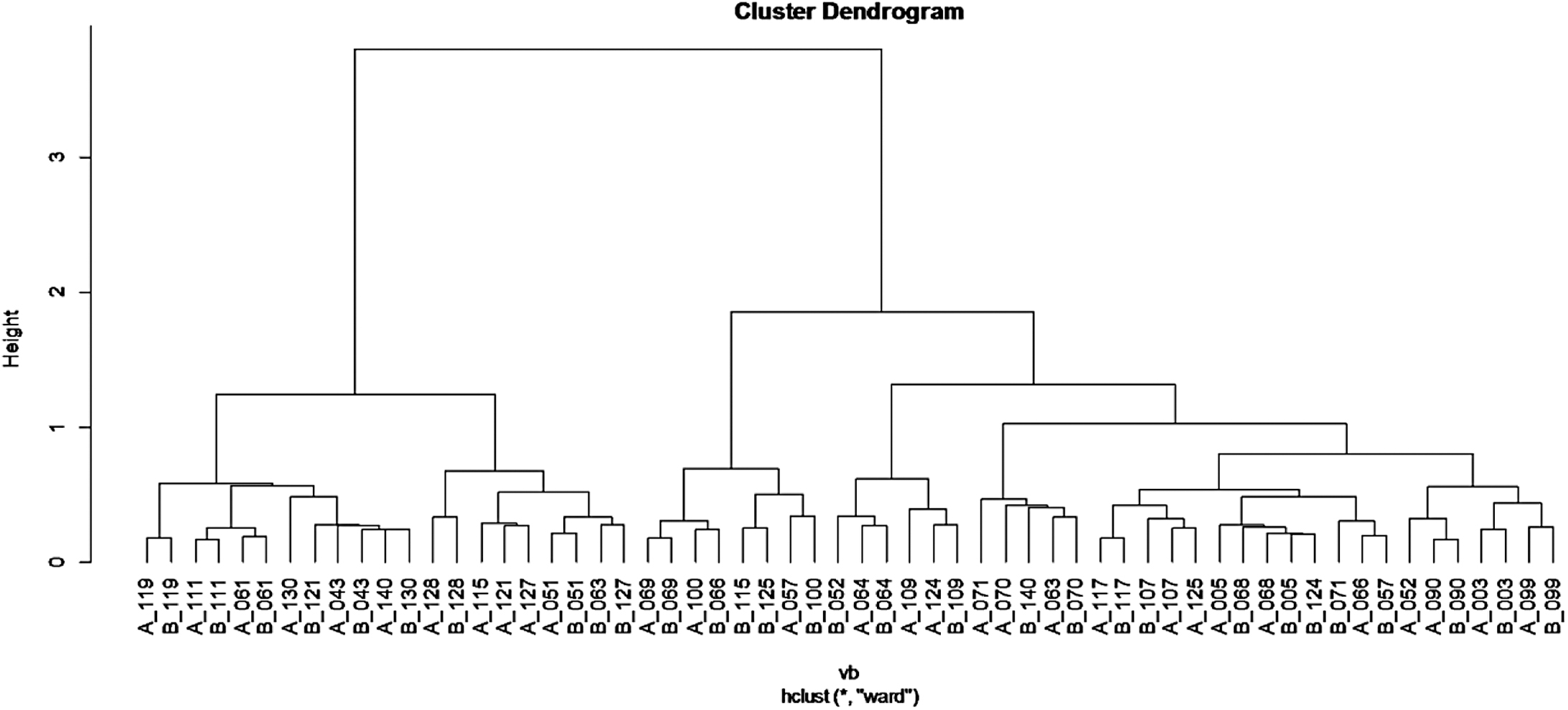
Microbiome data were analyzed using the Vegan 34 and Ecodist 35 packages in R 3.0.2. 30 The Bray–Curtis dissimilarity index was used to assess differences between samples, and results were visualized using hierarchical clustering (using Ward's method) and nonmetric multidimensional scaling ordination plots. Statistical significance for differences in microbiome diversity between pre- and postprebiotic treatment groups was determined using Adonis. 36 Normalized data were then log-transformed to examine treatment-induced changes in the microbiome.
Significance of differences across the cohort was determined by a one-sample t-test.
Results
The control group showed a greater increase in height than the intervention group (Table 1), confounding BMIp results. BF%, DF%, and total and saturated fat intake were reduced and PA was increased for the intervention group. Using Bonferroni correction for multiple tests would require a significance of .006 for each measure, so the hypothesis was not supported, although results were in the predicted direction.
Numbers include data available for that variable.
BF, body fat; DF, dietary fat; PA, physical activity; SD, standard deviation.
A post hoc power sensitivity analysis with GPower 37 showed that with n = 123, alpha = 0.05, and power = 80%, for a mean change over two time points, we were able to detect effect sizes of d = |0.25| or higher, and for a correlation, we were able to detect effect sizes r = |0.25| or higher.
A path analysis of pre/post changes in Firmicutes-to-Bacteroides ratios in stool samples suggested weak associations with the difference (post-pre) in BF%. Post-treatment BMI was associated with a lower pretest BMI, decrease in stool Tenericutes, and increase in Actinobacteria (R 2 = 0.466, Change BMI = 0.667–0.003*BMI_pre −2.603*Change_Tenericutes + 2.14*Change_Actinobacteria). Decrease in BF% was associated with higher pretest BF% (R 2 = 0.600, Change_bodyfat = 27.032 + 0.746*Body_Fat_pre). For the presented regression slopes, we reject the null hypothesis of the slope being equal to 0, p < 0.05.
We recruited participants from two schools for a total of 12 classrooms (7 intervention and 5 control classrooms). Of 241 children, 181 had parental consents returned (51%). All children with parental consent agreed to participate. All 78 assigned to the intervention classrooms completed the study without problems related to increased fiber intake. We received 43 pretest (55%) and 32 post-test (41%) stool samples.
No adverse effects were reported or observed. No participants withdrew from either group, although there were missing data for some variables if the child did not complete questionnaires or was not available on days that post measures were completed (6 children were missing in the intervention group and 1 was missing of 45 assigned to the control group).
To investigate if the treatment induced any changes in specific genera of bacteria, we quantified the treatment-induced changes in abundance (log abundance pretreatment – log abundance post-treatment) for the 183 identified taxonomy units of bacteria. Changes in abundance were examined across the 30 participants, and significance was determined using a one-sample t-test.
Results suggested that the prebiotic treatment resulted in a small increase in Lachnospiraceae-Anaerostipes (−0.24 log10; p-value 0.005) and small decreases in Ruminococcaceae-Anaerotruncus (0.20 log10; p-value 0.017), Erysipelotrichaceae-Erysipelotrichaceae (0.22 log10; p-value 0.007), and Erysipelotrichaceae-Turicibacter (0.22 log10; p-value 0.016), all members of the Firmicutes phyla.
Given the small magnitude of change (∼70% in either direction) and the relatively weak p-value, correction for multiple tests was not feasible, so we are not confident that these changes are indicative of the prebiotic treatment.
Microbiome biodiversity among individuals was large compared with pre-post differences. In some individuals, the microbiome changed significantly, while others had little change, resulting in no significant pre-post differences in stool microbiota for the sample as a whole.
This result led us to question if there are bacterial profiles that can serve as biomarkers for participants who are resistant to treatment-induced changes in the microbiome and if these biomarkers would correlate with, if not predict, the treatment's effect on physiology. To minimize data variance, we narrowed our analysis to the largest group of participants—those who were identified as Latinx.
Examination of the results (Fig. 2) revealed that participants were roughly separated into two groups: those with microbiome profiles that were “resistant” to treatment, as represented by participant 119 whose pretreatment (A_119) and post-treatment (B_119) samples clustered closest to each other compared with all other samples, and those with microbiome profiles that “changed” in response to treatment, as represented by participant 130 whose pretreatment (A_130) and post-treatment (B_130) samples clustered further apart.
We found five bacteria that exhibited different abundance levels between the “resistant” and “changed” groups: Clostridiales Family XIII, Turicibacter, Lachnospiraceae, Faecalibacterium, and Ruminococcaceae (Table 2). Of these, Clostridiales and Turicibacter were, respectively, two- and threefold higher in “changed” participants. Lachnospiraceae, Faecalibacterium, and Ruminococcaceae were, respectively, 2.4, 2.0, and 2.6-fold higher in “resistant” participants.
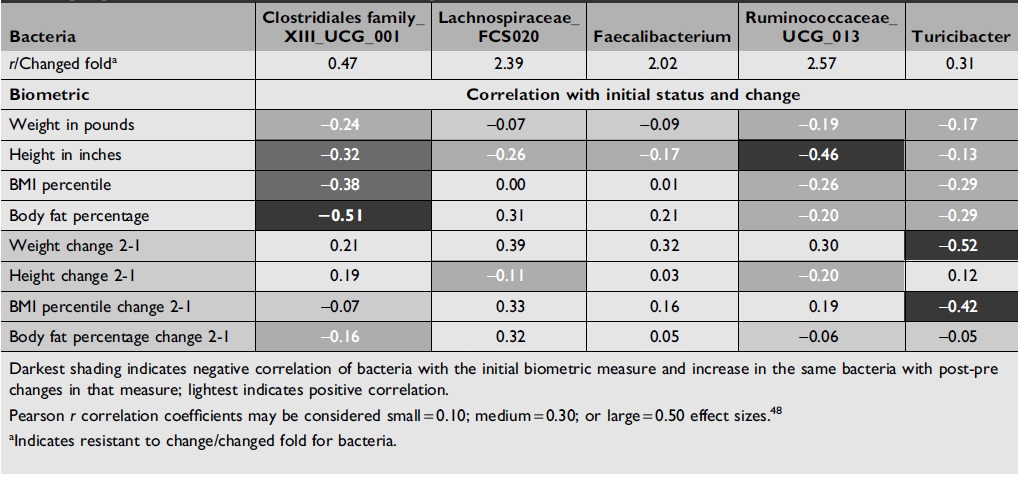
The higher levels of Lachnospiraceae, Faecalibacterium, and Ruminococcaceae correlated positively with changes in BMIp and weight, while Turicibacter had a negative correlation. No correlative trend with change in BMIp or weight was detected for Clostridiales.
Discussion
Congruent with the direction of our first hypothesis, but not at significant levels, we found that BF%, DF, and total and saturated fat intake were reduced and PA was increased for the intervention group, although further study with a larger sample is needed. Regarding our second hypothesis, Tenericutes is a phylum that may have emerged from Firmicutes, 38 but some species of Firmicutes in our sample increased and others decreased with respect to changes in BMIp and/or BF changes. An increase in Actinobacteria is broadly congruent with our second hypothesis, in that Bifidobacterium is a genus within the Actinobacteria phylum.
We demonstrated that administration of the prebiotic with calcium in addition to Project FUN, the online program, to improve DF and PA was feasible and acceptable without adverse effects in a population group experiencing increasing overweight and obesity. In terms of our second research question, we were able to recruit and retain participants.
There were no adverse effects of the prebiotic fiber with calcium. The prebiotic required shaking and stirring right before administration to prevent clumping, so it would be better included in baked goods usually eaten than in orange juice. Incorporation in usual foods would also reduce the time and cost of adding fiber to a beverage, as was done with this protocol.
We did not find significant changes in the stool microbiome with the intervention related to high biodiversity among participants. We mostly found small/medium correlations between the stool microbiome and BC.
High bacterial biodiversity without significant correlations with BMI z-score groups was also found by Borgo et al. 39 Children with obesity had significantly lower abundance of Akkermansia muciniphila, Faecalibacterium prausnitzii, Bacteroides/Prevotella group, Candida spp., and Saccharomyces spp. Since these associations were found with a larger sample (28 children with obesity and 33 age- and sex-matched children with normal weight), the current study may have been underpowered for this analysis.
Longer administration of prebiotic fiber and calcium may also be necessary for significant changes. A 16-week administration of 8 g/day OI in 22 (7–10-year-old) children with overweight/obesity compared with 20 controls given placebo showed significant decreases in body weight z-scores and BF%. Significant increases in Bifidobacterium and decreases in Bacteroides vulgatus were found within the group that consumed OI. 6
At this point, there does not seem to be a consistent pattern of microbiota associated with BMI, BF%, or change in response to inulin across studies.40–43 Diet and PA also affect microbiota 44 and were not controlled across studies. Microbiota patterns are established early in life with genetic and intrauterine influences, but tend to form an obesity-associated pattern with adoption of high DF and reduced PA. 45 A positive response to dietary fiber is dependent on the bacteria already inhabiting the intestine, which is determined by prior diet. 46
The current study was the first with Latinx and African American children. It is especially important to understand microbiota patterns and ways to reduce obesity in these groups since both obesity and associated microbiota patterns increase the risk for fatty liver disease, which is highest and often asymptomatic among Mexican American children. 45 Disparities in access to green spaces that may reduce the opportunity for PA have been associated with income and race. 47 PA is important for reducing obesity, but its prevalence is lower among Latinx children. 45
Small to medium effect sizes were found for some variables without statistical significance in this pilot study sample, warranting a larger study of this school-based intervention. Including prebiotic fibers in foods usually eaten by children with social determinants of high risk for obesity is suggested in larger community-based studies.
Limitations
Although this study offered trends in the expected direction, a larger sample is needed to reach adequate statistical power. Randomization by school should be conducted to avoid diffusion of the intervention and allocation concealment. Recall bias may have occurred with self-reporting.
Conclusions
Further research is needed to identify those individuals who respond to prebiotic fiber with reductions in BMI and BF or other physiologic improvements. A more consistent inulin delivery approach is needed with culturally congruent foods for those most at risk for obesity.
The combination of prebiotic fiber and an online health promotion/transtheoretical model intervention is feasible. Identifying characteristics of those with changes in the microbiome will help to target those with the best likelihood of improvement with this type of intervention for a larger study.
Footnotes
Impact Statement
To our knowledge, the current study was the first to include Latinx and African American children in a test of prebiotic fiber and an online program. It is especially important to understand microbiota patterns and ways to reduce obesity in these groups. Obesity and associated microbiota patterns increase the risk for fatty liver disease, which is highest and often asymptomatic among Mexican American children.
Authors' Contributions
M.F. and N.S. were involved in conceptualization, funding acquisition, investigation, and supervision. V.L. and M.G.-V. were involved in formal analysis. A.M. was involved in investigation (bioimpedance), training for 24-hour diet recalls, and measurement of prebiotic fiber. M.H. assisted with IRB protocol management. M.F. wrote the original draft. All authors were involved in manuscript review and contribution and gave final approval of the submitted and published versions.
Funding Information
This work was supported by the Clinical and Translational Science Institute of Southeastern Wisconsin and the Beneo Corporation. Beneo provided the prebiotic fiber and funding for the microbiome analysis, but did not control or influence the findings or report.
Author Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.