
Abstract
The COVID-19 pandemic has been associated with increases in pediatric obesity and widening pre-existing disparities. To better understand the pandemic's long-term impacts, we evaluated trends in obesity across different demographic groups during the pandemic through December 2022. Using a retrospective cohort design, we analyzed electronic health record data from a large pediatric primary care network. Logistic regression models fit using generalized estimating equations estimated odds ratios (ORs) for changes in the level and trajectory of obesity across 2-year month-matched periods: prepandemic (June 2017 to December 2019) and pandemic (June 2020 to December 2022). Among a cohort of 153,667 patients with visits in each period, there was a significant increase in the level of obesity at the pandemic onset [OR: 1.229, 95% confidence interval (CI): 1.211–1.247] followed by a significant decrease in the trend for obesity (OR: 0.993, 95% CI: 0.992–0.993). By December 2022, obesity had returned to prepandemic levels. However, persistent sociodemographic disparities remain.
Introduction
Rapid increases in pediatric BMI occurred during the COVID-19 pandemic.1–3 Younger school-aged children experienced the largest increases,1–3 and pre-existing disparities in obesity by race/ethnicity and insurance status widened following the onset of the pandemic. 1 As we continue to understand the long-term public health impacts of the COVID-19 pandemic, a better understanding of the disparities in the pandemic's impact on specific pediatric populations is needed to guide obesity prevention and management efforts. Through a large pediatric primary care network and building upon prior work, 1 we aimed to evaluate trends in obesity across different demographic groups during the COVID-19 pandemic through December 2022.
Methods
Using a retrospective cohort design modeled after an interrupted time series, 4 we analyzed electronic health record (EHR) data from Children's Hospital of Philadelphia's (CHOP) pediatric primary care network, which included 31 urban, suburban, and semirural clinics in the Philadelphia region. We examined 2-year month-matched periods: prepandemic (June 2017 to December 2019) and pandemic (June 2020 to December 2022).
We excluded data early in the pandemic (March 1, 2020, to May 31, 2020) due to extremely low visit volume related to pandemic restrictions. Our cohort consisted of patients 5–17 years of age (defined as age at the start of the pandemic, March 1, 2020), who had at least one preventive visit during each of these two analytic periods, at which both height and weight measurements were collected. We used the R package growthcleanr to exclude biologically implausible measurements. 5 Our binary outcome was obesity, defined as a BMI at or above the 95th percentile based on CDC age- and sex-adjusted growth curves. 6
Using Stata version 16 and R version 3.6.2, we first plotted the observed monthly prevalence of obesity over the prepandemic and pandemic periods. Next, we fit logistic regression models using generalized estimating equations with an exchangeable correlation structure and robust standard errors, accounting for repeated measures at the patient level. These models evaluated changes in obesity levels (intercepts) and trajectories (slopes) between the prepandemic and pandemic periods. Covariates were a binary pandemic indicator (prepandemic, pandemic; estimating the change in level), time (in months) as a continuous variable (estimating the prepandemic trend), and the pandemic/time interaction (estimating the change in trend). We also adjusted for primary care clinic site and calendar month to account for potential seasonality.
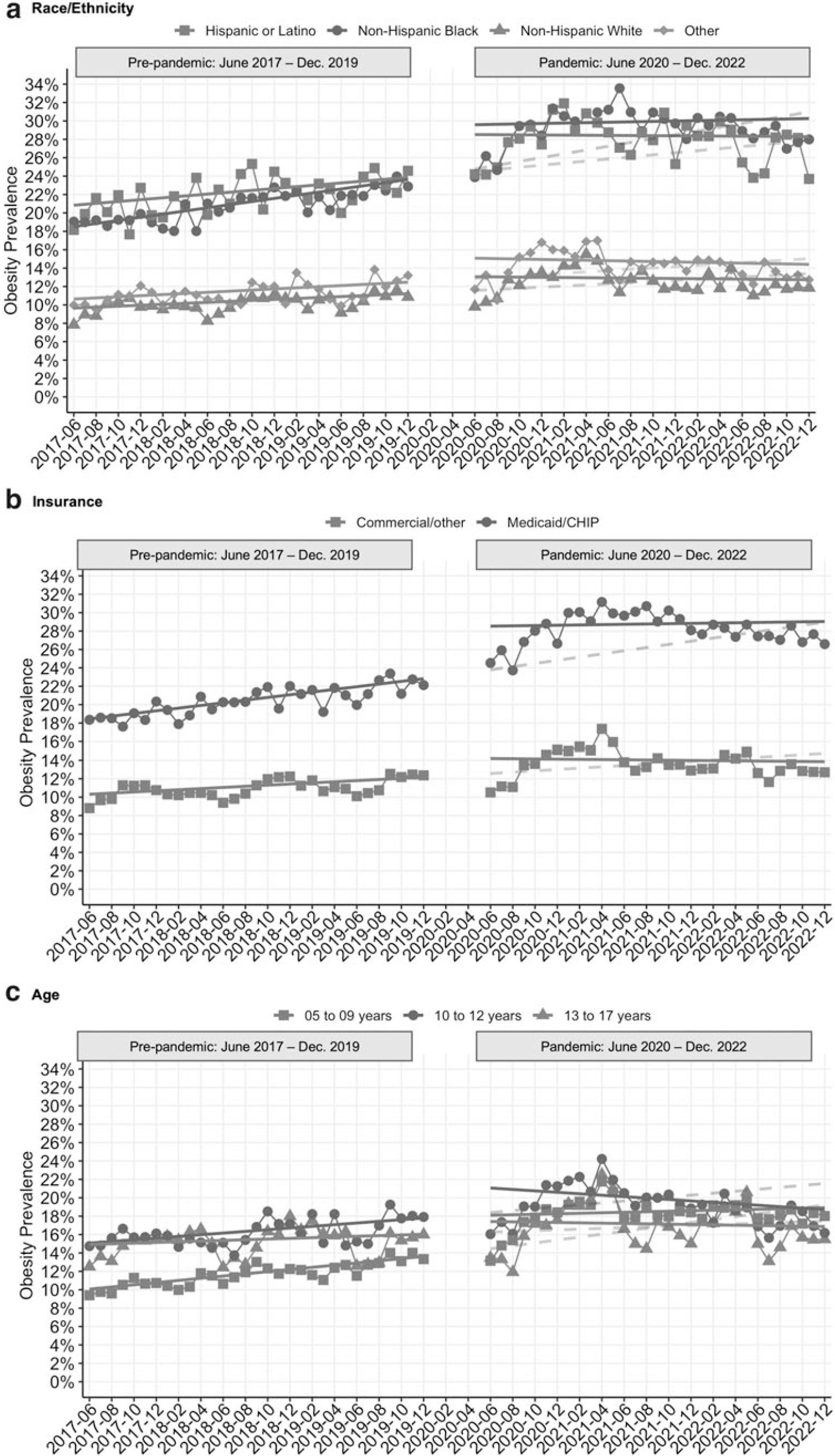
We examined changes in obesity overall and separately by race/ethnicity (Hispanic or Latino, non-Hispanic Black, non-Hispanic white, or other), insurance (public vs. commercial/other), and age (5–9, 10–12, and 13–17 years old). CHOP's Institutional Review Board determined this study exempt from review.
Results
Our cohort included 153,667 patients who had 613,740 primary care preventive visits: 317,423 visits during the prepandemic period and 296,317 visits during the pandemic period. Patients were seen an average of 4 times [standard deviation (SD) = 1.1] during the study period. The mean age of our cohort at the last visit was 10.8 years (SD = 3.5) and it included 48.9% female patients, 32.9% publicly insured patients, 8.5% Hispanic or Latino patients, 25.8% non-Hispanic Black patients, and 49.3% non-Hispanic white patients (Supplementary Table S1).
After the pandemic onset, we observed an increase in the prevalence of obesity in our cohort, which peaked at 22.6% in April 2021 before declining back toward prepandemic levels. By December 2022, obesity prevalence was similar to prepandemic levels (17.0% in December 2022 vs. 15.3% in December 2019). The regression results reflect this pattern, showing a significant increase in the level of obesity at the onset of the pandemic [odds ratio (OR): 1.229, 95% CI: 1.211–1.247] followed by a significant decrease in the trend for obesity relative to the prepandemic period (OR: 0.993, 95% CI: 0.992–0.993). See Figure 1 and Supplementary Table S2. All demographic subgroups followed a similar pattern. Although obesity rates returned to prepandemic levels, persistent disparities remain by both race/ethnicity and insurance status. See Figure 2 and Supplementary Table S2.

Discussion
Despite an initial uptick in the prevalence of obesity in our large primary care network during the pandemic, obesity had returned to prepandemic levels by December 2022. These results may be due to adverse effects that early pandemic shutdowns had on diet and activity levels. The COVID-19 pandemic likely exacerbated all the risk factors for weight gain, similar to risk factors for weight gain associated with summer recess. 7 These risks include increased food insecurity, consumption of highly processed, calorie-dense foods, screen time, and sedentary activities. 7
Alternatively, it may be that patients with obesity were more likely to have health concerns that warranted an office visit early in the pandemic, and these results could reflect pandemic-related changes in health care-seeking behaviors rather than a true change in obesity prevalence. Although obesity rates have returned to prepandemic levels, persistent disparities remain. There is much work to be done to improve obesity rates for all pediatric groups.
Clinical guidelines now recommend intensive health behavior lifestyle treatment, motivational interviewing, metabolic and bariatric surgery, and pharmacotherapy in the evaluation and treatment of obesity and overweight children. 8 While clinical and health system change will likely play a role in addressing the obesity epidemic among children, the pandemic continues to expose the need for larger policy changes that systematically address the complex environmental determinants of dietary habits and physical activity. Population-level measurements of obesity appeared to dramatically increase and then decrease during the pandemic, likely independent of any dramatic change to clinical interventions.
More work is needed to improve access to healthy school lunches and reduce food insecurity, 8 eliminate agriculture policies that distort market forces and promote obesity (such as agricultural subsidies),9,10 and promote physical activity through community-based changes in the built environment.11,12 Our previous analysis identifying the widening disparities in pediatric obesity underscored the importance of such efforts ∼1 year into the COVID-19 pandemic. 1 Although obesity rates have now returned to prepandemic levels, the pre-existing disparities persist and continue to emphasize the need for action now.
A strength of this study is the use of EHR data from a large, diverse pediatric network. However, our sample consisted of a limited geographic area and could only account for obesity rates among patients who came in for primary care visits. Thus, these results may not be reflective of the general pediatric population. In addition, there are several biases in using EHR data, including selection bias from patients who have more contact with the medical system, who then have more opportunities to receive diagnoses,13–15 the need to consider the context in which EHR data are collected, 16 and general data quality assurance issues, including data inaccuracies (e.g., misclassification) and incompleteness (e.g., the presence of uncaptured covariates).17,18
Our study potentially overcame these limitations by identifying a cohort of patients who had BMI measures across both time periods analyzed, leveraging data that are routinely and systemically captured as part of preventive care visits, and, using data cleaning methods to eliminate biologically implausible measurements. 5 Another potential issue with our analysis is the adjustment for only one level of clustering, the patient level, whereas the true underlying clustering pattern could be more complex (e.g., additional clustering on the practice and physician levels). We considered a mixed-effects model to additionally account for patient-level clustering, but this particular data set faced convergence issues when fitting the model.
Footnotes
Authors' Contributions
Dr. Jenssen conceptualized and designed the study, drafted the initial article, and reviewed and revised the article. Ms. Kelly designed the data collection instruments, collected data, carried out the initial analyses, and reviewed and revised the article. Drs. Dalembert, McPeak, Mayne, Shu and Fiks, and Ms. Powell conceptualized and designed the study, coordinated and supervised data collection, and critically reviewed the article for important intellectual content. All authors approved the final article as submitted and agree to be accountable for all aspects of the work.
Funding Information
No funding was received for this article.
Author Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.