
Abstract
Background:
Head start (HS) programs are required to collect children's height and weight data. Programs also communicate these results to families. However, no standardized protocol exists to guide measurements or communicate results. The purpose of this article was to describe the development of a measurement toolkit and best practices for communication.
Methods:
HS programs contributed to the development and pilot testing of a toolkit for HS staff to guide child measurement. We used a three-phase iterative approach and qualitative methods to develop and test the toolkit, which included a video and handout. In addition, we convened an advisory group to draft best practices for communication.
Results:
HS program staff appreciated the toolkit materials for their simplicity and content. The advisory group highlighted the importance of weight stigma and the need to be cautious in the way that information is communicated to families. The group underscored the role of emphasizing health behavior change, instead of focusing solely on BMI. Best practices were organized into (1) Policies and procedures for communicating screening results, (2) training for HS program staff to improve communication related to screening and health behaviors, and (3) other best practices to promote health behaviors and coordinate data systems.
Conclusions:
Our toolkit can improve anthropometric measurements of HS to ensure that potential surveillance data are accurate. Advisory group best practices highlight opportunities for HS to develop and implement policies, procedures, and trainings across the country to improve communication with HS families. Future research should test the implementation of these best practices within HS.
Introduction
Head start (HS) is a federal program designed to promote school readiness of preschool-aged children from low-income families. HS programs collect children's anthropometric data and communicate results to families to address obesity in enrolled children, as mandated by the Improving HS School Readiness Act of 2007.1,2 HS Programs Performance Standards are mandated federal regulations to ensure high-quality programs and services. They are broad to allow flexibility in tailoring to differences in programs and require programs to identify each child's health needs. As part of this process, HS requires that anthropometric measurements be collected. This includes height and weight data that are used to calculate BMI and plotted on the Center for Disease Control (CDC) BMI-for-age growth charts to determine the child's weight status (“underweight” “healthy weight,” “overweight,” or “obese”).
These aggregated data are entered into the annual Program Information Report within 45 days of enrollment and are used nationally for surveillance efforts over time and to inform program outcomes. 3 In addition, Performance Standards require that programs collaborate and communicate with parents about their children's health, including recommending children obtain necessary referrals, follow-up appointments, and treatment. 3 Despite these requirements, the 2016 Performance Standards do not include detailed measurement protocols necessary for consistency and accuracy of measurement. Furthermore, there is lack of guidance on how programs should be communicating this information to families.
Although anthropometric data are used to explore childhood obesity prevalence and trends and used to evaluate HS programming,4–6 measurement procedures are not standardized across the 1700 programs in the United States. As such, suboptimal data may skew surveillance and program outcomes.7,8 Survey results from 363 HS programs indicated that most programs believe collecting anthropometric data is important and helpful for improving children's health, 9 yet there was lack of consistency across procedures, protocols, and equipment.
In addition, respondents were concerned about family reactions to receiving measurement results and the lack of skills in communicating this information and connecting families to important health resources. Similar findings were reported in a recent qualitative study, which highlighted the need for training in precise measurement of children's height and weight, clarifying the referral/follow-up process, and better support for families to implement behavior change. 8 Additional studies have found a lack of consistency in communicating BMI information with families and highlighted the need for this communication to be sensitive and nonjudgmental.10,11
Although there is evidence on best practices for communicating with families about obesity and weight-related topics for health professionals in clinical practice settings, 12 it is unclear if these translate to individual community-based HS programs. Therefore, the purpose of this project was to (1) develop and test the acceptability and feasibility of a quality improvement toolkit for the measurement of height and weight in HS children and (2) engage experts to develop best practices regarding communicating this information with families. Misclassification of weight status due to inaccurate measurements can undermine the value of BMI screening, reporting, and surveillance data, as well as diminish HS parent trust, jeopardizing the important relationship with HS. The toolkit will help standardize anthropometric data collection across HS programs, which can improve surveillance, and the best practices will provide guidance to the National Office of HS to improve communication with families.
Methods
Overview of Project
Our interprofessional project team comprised researchers experienced in working with HS programs across multiple states.8,10,11,13 Additional team members included representatives from CDC's, Physical Activity and Obesity, and the National Office of HS. The CDC's representative provided important insight due to their role in promoting and supporting systems, policy, and screening related to nutrition, physical activity, and evidence-based family healthy weight programs. We developed and feasibility tested a toolkit for anthropometric measurement of preschoolers, 3–5 years of age, in HS and engaged an advisory board to develop best practices for communicating results and obesity risk with families.
The development of the toolkit was organized into three phases: (1) formative; (2) development; and (3) pilot testing. During each phase, individual program-level HS staff across multiple states were engaged and their feedback was integrated to ensure grounding, relevance, applicability, and quality within HS program structure and process. Simultaneously, we identified experts to join an advisory group to discuss best practices related to the communication of height and weight measurements to families who participate in HS. The Institutional Review Board at the first author's institution determined approval was not required because the project was not considered human subjects research (i.e., data were related to HS programs, not people).
Development of the Toolkit to Guide Anthropometric Measurements
Phase 1: Formative phase
We first conducted 10, 45-minute virtual meetings with different HS staff across the country (Table 1) to better understand how height and weight were measured and communicated by their respective programs, to gather information about their current training procedures, and to identify any challenge, success, or opportunity for improvement. Staff were recruited through a flier, which was shared with HS program contacts in RI, NC, OK, and OH, and the National HS office, which shared the flier with state-level Program Collaboration Directors to disseminate in their respective states. The participants were compensated with a $50 gift card.
All meetings were conducted by the research team using a team-approved guided script.
Due to the nature of this project, only program-level data were collected.
North Carolina, Ohio, and, Oklahoma and Rhode Island were chosen due to relationships with HS programs in the given states among the members of our project team.
HS, head start.
Phase 2: Toolkit development
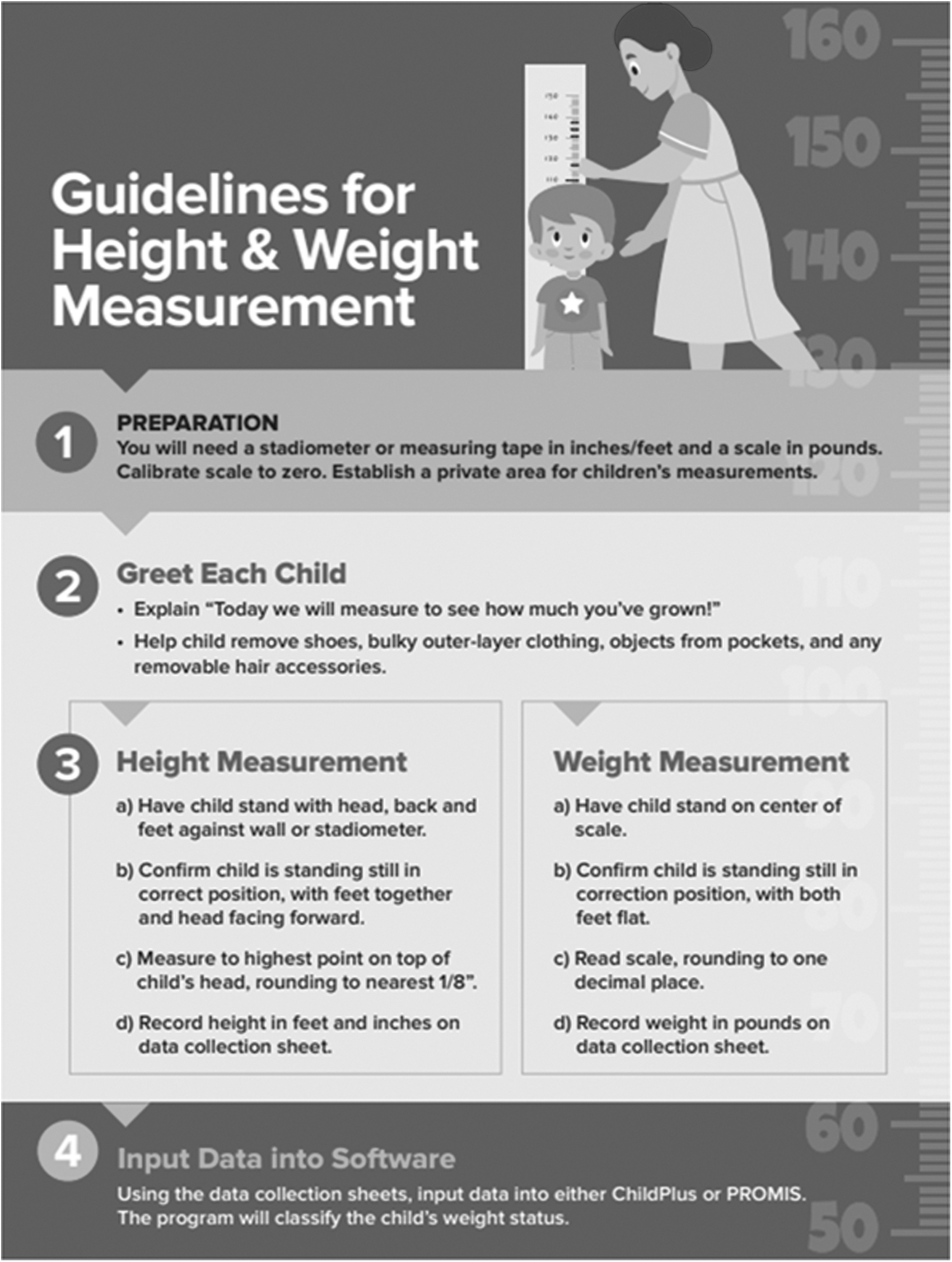
With input from HS staff from Phase 1, we identified the need for a toolkit that contained a training video and a handout that could be stored with scales and stadiometers. We created a video script informed by literature and CDC's best practices, which included (1) use of appropriate equipment, (2) removal of extra clothing/accessories, (3) correct child positioning, (4) precision level of recording measurements, and (5) collecting measurements in a private space, if possible. 14 The handout included simple instructions, images, tips, and common mistakes (Fig. 1). We invited HS program staff back to a second round of group meetings (Table 1) for feedback, which was then incorporated and prepared for feasibility testing.
Initial toolkit.
Phase 3: Feasibility testing of the toolkit
The same HS program staff from phase 1 and 2 were invited to participate in feasibility testing (Table 1). Programs received the toolkit materials and were asked to use them during their pre-service training with staff responsible for anthropometric measurements. Following the training, staff were invited to participate in a 30-minute semistructured interview to provide feedback on the use of the toolkit. Questions included how the training was received by staff, the ease or difficulty of incorporating the toolkit into their overall training, and how toolkit materials impacted staff knowledge, attitudes, and measurement techniques.
Data Analysis for Phases 1–3
All meetings and interviews were informed by guides developed by our project team and were recorded and transcribed using Zoom. 15 We utilized rapid qualitative analysis 16 to summarize meeting notes from the formative and developmental phases of the toolkit. The team took thorough notes during each meeting and then immediately summarized, identifying major themes that emerged. These themes were then discussed with the larger project team during bi-weekly meetings and then summary data from each of the meetings were integrated into one document, and final themes were identified by the project team.
Two team members, trained in qualitative analysis, conducted thematic analysis 17 of the interview transcripts using deductive coding in NVivo. 18 A codebook was developed by the analysis team utilizing the interview script as a guide; these codes were used throughout the analysis. The analysis team coded five transcripts together with ongoing discussions on similarities and discrepancies. Upon reaching 100% consensus of the five co-coded transcripts, the remainder of the transcripts were individually coded by one team member.
Advisory Group—Communicating Height and Weight Data
Eleven experts, including academic researchers in obesity prevention, weight stigma, child development, and mental health; two pediatricians; one member from the Early Childhood Division of National HS; and one member from CDC were invited and participated in the advisory group. Experts were identified by an online search of publications and research in the field, as well as in discussions with the grant funders who helped identify relevant expertise. The advisory group participated in three 60–90-minute Zoom meetings along with the research team members.
The first meeting was dedicated to introducing the project and having an initial discussion on height and weight communication, including guiding questions such as “What is valuable in communicating weight status information with families?,” “What are areas of concern in communicating this information with families?,” “How do we minimize risk and adverse experiences?,” and “How could we improve the process?”
During the second meeting, members were divided into groups to help draft initial ideas for best practices. Based on the first two meetings, the research team then drafted an initial set of best practices. During the third meeting, members reviewed and revised the draft best practices. The research team then integrated these changes and shared the final draft for further comments. The updated best practices were shared with the senior National HS Program Specialist, who suggested adding a secondary guidance document to help operationalize the best practices.
The research team created the operationalization document and shared with the advisory group to receive feedback. The final best practices were shared with the Health Program Specialist from the National office of HS; the Health and Nutrition Managers and Advisory Board of a key partner program in Ohio; the HS Collaborative Advisory Board in Oklahoma; and the North Carolina HS Association annual conference. Feedback was then incorporated into the final best practices.
Results
Toolkit Formative Phase 1—Collecting Height and Weight Data
Overall themes of meetings with HS program staff included needing better equipment for measurements and the lack of standardized procedures. For example, staff from different programs described variable methods in how measurements were obtained, where some used stadiometers and some used wall-mounted height posters. Some teachers described the measurement process as relatively easy because kids were excited, while others described it as time-consuming, particularly for locations with many children. Teachers emphasized that student absence, staff turnover, and classroom behavior presented additional challenges to data collection because of COVID-19. They also highlighted the need for standardized training and materials on why accurate measurements are important and how data are utilized.
Toolkit Development Phase 2—Collecting Height and Weight Data
After viewing the video (9:28 minutes) and handout, staff expressed an appreciation for the length (brevity) and simplicity, describing it as “easy to understand.” In addition, participants enjoyed the script-like approach, walking the child through the entire process of measurement, and the emphasis on dos and don'ts for measuring, particularly for shoes, jackets, and hair accessories.
However, several participants mentioned barriers to applying best practices in their setting. For example, program size limited the feasibility of conducting measurements in a private setting and having a consistent measurement team. They also highlighted the need for additional information on troubleshooting various challenging scenarios. Based on this feedback several additions were made to the video and handout [i.e., voiceover to emphasize the importance of removing jackets/shoes, pop-up text relevant to cultural considerations, testimonial from an HS staff member, zoomed-in imagery of measurement scale and guidelines for measurement conversions, and a guide for equipment (Figs. 2–4)].

Modified toolkit (First Page).

Modified toolkit (Second Page).
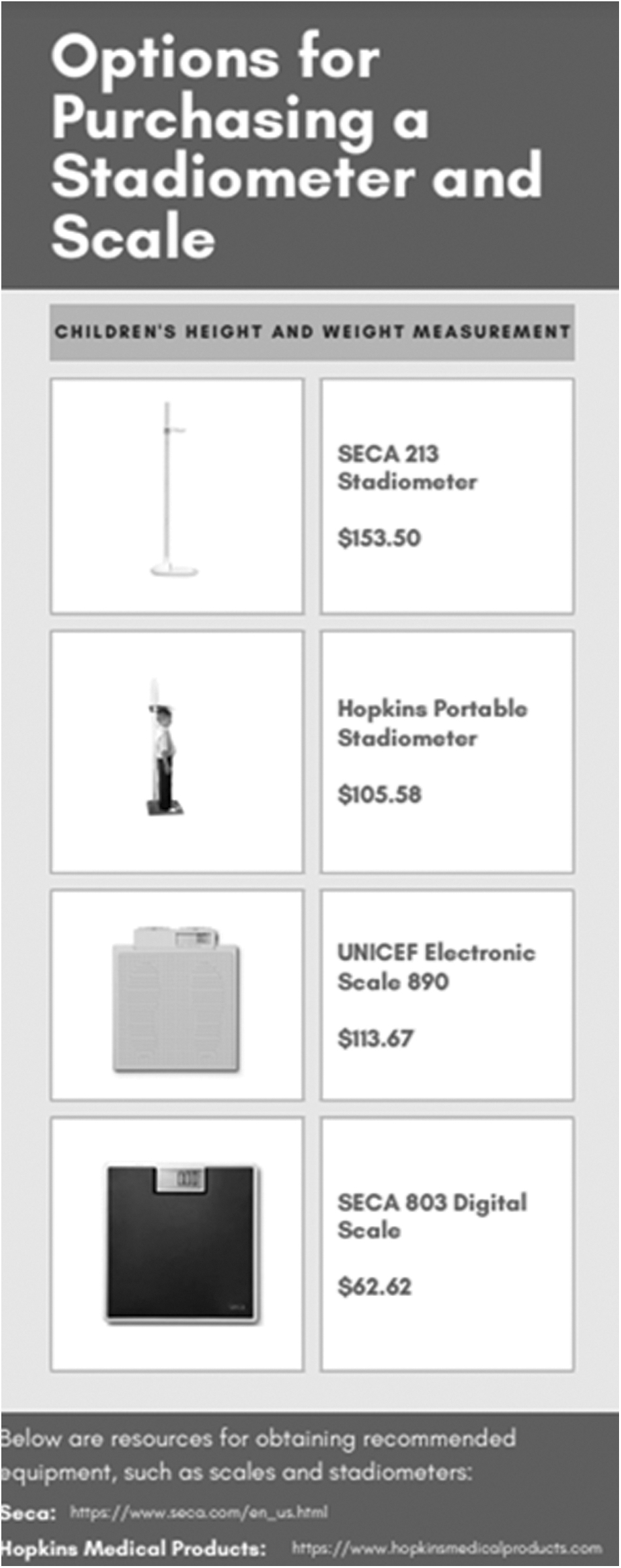
Recommendations for stadiometers and scales.
Toolkit Pilot Testing Phase—Collecting Height and Weight Data
Interview themes were organized according to the interview guide as follows: (1) overall experience, (2) main insights, (3) video feedback, (4) handout feedback, (5) barriers, and the next steps. Details are provided in Table 2.
Qualitative Analysis from Pilot Training Interviews
Overall experience
HS staff in both the trainer and trainee roles expressed appreciation for the training. Participants commented that they appreciated receiving this training on measurement, particularly considering how long they had been employed by HS before being trained. One participant stated, “I found it exciting because … I've been with HS for 33 years and this is the first I ever heard of a training on [height and weight].”
Main insights
Trainees mentioned how the training highlighted the importance of conducting measurements, along with recognizing how crucial it is for these measurements to be accurate—“It helped you learn how to get accurate height and weight for the children.” Furthermore, they thought that the training was incredibly useful and filled a training gap. Many said the training would be ideal either as a refresher for the seasoned staff or as a beginner training for those who are newly hired—“It was … a really good refresher, I think, for everybody.”
Video and handout feedback
Interviewees appreciated the simplicity and enjoyed the process flow of the video, guiding staff through the step-by-step process to ensure accurate measurements—“The whole thing, it was basically step by step. It was perfect.” That said, a few mentioned the quality of the video needed to be improved, particularly with respect to sound quality and backdrop. Participants also appreciated the handout for its simplicity and believed it would help them conduct measurements and engage children—“I really think that's useful too, not just for us, but for the visuals for the children as well.”
Barriers and opportunities for further improvements
Some of the major barriers that participants shared were related to equipment and children's behavior. For example, they discussed how some of the equipment they use was outdated or flimsy, while others expressed a desire to have access to the equipment used in the video (stadiometer and digital scale).
Trainees also noted it could be difficult to get a proper measurement for children who are fidgety or developmentally or mentally differently abled. Participants mentioned how sensitive the topic of weight can be and how difficult it can be to speak with parents about their child's weight, and as a result, many expressed the need for additional tools to explain why measurements are conducted. Many requested similar training to help teach and train staff on the best ways to communicate sensitive information to families—“They (teachers) need to be able to explain how it came to that measurement and also explain why it's important that they know, and ways that they can address that cause it is, I think it's really difficult.”
Advisory Group Best Practices for—Communicating Height and Weight
The advisory group highlighted the issue of weight stigma and the need to be cautious in the way that information is communicated to families. The group also discussed the importance for best practices to be adapted to different cultures, as needed. In addition, the importance of promoting healthy behaviors at this young age was also critical.
The best practices were organized into three categories: (1) policies and procedures for communicating height and weight screening results with families; (2) training to improve communication related to height and weight screening and health behaviors; and (3) other best practices to promote health behaviors and coordinate data systems (Table 3). Along with these best practices, we drafted appendices detailing suggested language to be used in communication with families, resources for connecting families with child nutrition programs, tips for promoting healthy behaviors for children and families, and suggested training and workshops for HS staff. A draft of the final best practices and the operationalizing of these documents can be found in Supplementary Appendix SA1.
Best Practices from Advisory Group
Discussion and Conclusion
HS is nationally recognized for its efforts toward preparing young children academically and social-emotionally and prioritizing their health and well-being, including people of color and others who have been historically marginalized, and adversely affected by persistent poverty and inequities. 19 Collecting height and weight data is part of these efforts. Although HS programs are required to report aggregate weight status classifications of enrolled preschool children, there is limited guidance on how data are collected, and research indicates most programs conduct these measurements on-site at least once per year.5,8–11,13
To overcome this gap, we developed a toolkit with systematic input from HS program staff to standardize these data. Staff who tested this toolkit found it feasible and useful. Given the lack of recommendations on how to communicate health behavior information to HS families, we also reported best practices, which upon future testing could be integrated into HS policies and practices at the national level with consideration for local and cultural contexts in which HS programs operate.
Our formative data showed programs did not have standardized training available to them on how to collect height and weight measurements and that they utilized a variety of data collection methods. These findings are consistent with our previous work,8–11,20 whereby a little over half of the HS health managers reported having a protocol in place, that different equipment was used to collect these measures, and that barriers such as student absence, staff turnover, and classroom behavior presented additional challenges to data collection. HS staff also identified the need to have protocols and trainings in place to help standardize procedures.
There has been growing attention to the use of BMI, highlighting the drawbacks of this metric to measure body fat in multiple groups, namely racial and ethnic minority groups, especially as it relates to screening at an individual level. 21 It is noteworthy to state that most children enrolled in HS programs across the country represent racial and ethnic minority groups. 22 Recently, the American Medical Association suggested that this metric be used in conjunction with other valid measures and noted that BMI is significantly correlated with the amount of fat mass in the general population, but loses predictability when applied on the individual level.23,24
Research should continue to explore alternate frameworks that de-emphasize BMI in favor of other more precise measures and measures that address healthy lifestyle behaviors regardless of body size. If using BMI, it is important to utilize sex-specific BMI-for-age percentiles to track growth trajectory in children over time rather than isolated assessment of one measurement, as recommended by the American Academy of Pediatrics. Nonetheless, at a population level, BMI continues to be the “best” screening tool for obesity and ensuring standardization of the process is critical, given that misclassification of BMI undermines the value of BMI screening and reporting.
Regarding our toolkit, HS staff reported that using a short video hosted on YouTube with a short, easy-to-use handout was simple to access, use, and integrate within existing pre-service training. In addition, we found that HS program staff appreciated the training toolkit, acknowledging its simplicity, educational nature, and process overview. The toolkit encourages programs to consider their own local and cultural context in a manner that supports equity and inclusion. While no other study to our knowledge has reported the development and feedback of a BMI toolkit and training for HS staff, we can draw from studies conducted within schools where BMI report cards were common practice. For example, one study 25 similarly provided school staff with height and weight training using a video and laminated cards, and found that staff who watched the training video were more likely to accurately measure student weight with trends for improved accuracy in height.
While training can enhance accuracy of measurements, we found that barriers such as equipment, space, and time were reported. Future efforts related to screening should consider ways to standardize equipment or update equipment. Furthermore, HS should continue to assess how BMI data are collected and used to maximize efficiencies. For example, HS programs can receive height and weight data from the child's primary care provider, but this is not done in a systematic way. Future efforts to coordinate data, referrals, and communication between primary care providers and HS are critical to support children's healthy growth and development.
There was a need for best practices on how to approach communication with families of preschool-aged children, especially in families representing communities that have been historically disadvantaged. 26 While several best practice recommendation documents have been published within the clinical setting on how to communicate height and weight information to children,12,27,28 there was none specific to HS. The advisory group highlighted the issue of weight stigma and the need to be cautious in the way that information is communicated to families. Using sensitive, person-first plain language was emphasized by the advisory group to avoid weight stigma.
These best practices are consistent with a recent report, which highlighted that too often “children and parents are blamed for a lack of responsibility regarding health problems associated with large body size.”29,30 This report highlighted how racial, ethnic, gender, and class-based biases play into the history of biometric approaches to the health risks of weight and can result in stigmatization. Clearly, weight stigma needs to be considered, as it can be experienced by children starting at a very young age and can contribute to negative well-being and detrimental mental health outcomes. 31
Furthermore, the committee emphasized focusing on behavior changes to encourage a healthy, active lifestyle, instead of focusing exclusively on BMI. Recommending that HS programs promote physical activity, healthy eating, and sleep is supported by literature highlighting the importance of encouraging healthy habits at a young age, 32 particularly among children from historically marginalized communities. 33 The best practices promoted by the committee, organized into policies and procedures, trainings, and improvements to promote health and coordinate data systems, are consistent with HS policies and practices.
It will be critical to think of ways in which HS can continue to create more efficient systems that address the “whole child” (physical and mental well-being). For example, better connections to and communication with community care providers, primary care, and integration of community-based nutrition services at HS centers could help to provide a more cohesive, supportive environment to maximize the impact of HS in the social, emotional, and physical development of the children served. Future efforts are also needed to integrate the voices of families who bring their own lived experiences.
It is important to put these findings within the broader context of obesity prevention. First, prevention of obesity is quite complex and requires a multisector, multilevel approach. Among young children, a growing body of literature suggests that embedding nutrition and physical activity best practice standards 34 in the early care and education settings is associated with healthy lifestyle behaviors. However, we need to be mindful of families' access to healthy foods and neighborhood safety in carrying out these best practices safely. In addition, there is no evidence on what role BMI screening within this setting has on child behavior and obesity outcomes. We can draw from school-based studies, however. For example, a recent study found no significant difference in weight status after 2-year follow-up between students whose BMI information was reported to parents and those who were not. 35
In fact, students whose data were assessed had increased weight dissatisfaction compared to those without BMI screening or reporting. 35 However, the assessment of BMI in HS has been used to demonstrate the impact of HS on improving weight status of those children in the highest risk BMI categories. 7 The advisory board best practices are to promote health behaviors without focusing on BMI per se. Future studies can continue to assess the impact of these health behaviors on long-term health outcomes.
There were several limitations worth noting: (1) The data from HS staff who participated in this study was at a programmatic level and as such were unable to identify important individual-level factors; (2) the video was not professionally recorded and as such the sound quality was low; (3) the toolkit does not provide best practices on how to communicate with families; and (4) given the scope of the grant, it was not possible to incorporate the lived experiences of families and how they would inform communication recommendations. Future research should include the feedback of families from different backgrounds and embed this within the toolkit and best practices. With this feedback, future research should revise the toolkit to include best practices on communication with families and test the implementation of the best practices within HS.
Utilizing the findings from both the toolkit and the work of the advisory group, we plan to work with National HS to incorporate best practices for conducting anthropometric measurements and communicating to families. Our hope is that these best practices, along with suggestions for operationalizing them, can inform future research so that HS staff and programs nationally can implement them to improve health and well-being.
Impact Statement
Accurate measurement and classification of BMI are critical to screening, reporting, and surveillance in HS. We developed an evidence-based toolkit to address the barriers to accurate measurement and provide a resource for training, which can be further developed and evaluated for efficacy. Advisory group discussions yielded best practices for HS communication of BMI to families emphasizing a focus on health behaviors rather than weight.
Footnotes
Acknowledgments
We would like to thank all the HS teachers, health managers, and family advocates for their input throughout this process, along with Amy Lewis, MS, for assistance with videography. We would also like to thank the members of the advisory committee, including Natasha L. Burke, PhD, MA, Katherine W. Bauer, PhD, Caree Cotwright, PhD, MS, William Dietz, PhD, MD, Carrie Dooyema, MPH, MSN, RN, Neal M. Horen, PhD, MS, MA, Marti Kubik, PhD, MSN, Suzanne Lazorick, MD, MPH, Rebecca Puhl, PhD, MS, BAH, Loreene Ritchie, PhD, RD, and Ashley Weedn, MD, MPH, for their participation.
Authors' Contributions
A.T., B.M., E.G., V.S., and S.S.: Conceptualization and Methodology S.F. and A.T.: Writing-Original draft preparations. S.B.N., J.H., and M.B.: Writing-Reviewing and Editing.
Funding Information
Authors of this report are members of the Head Start BMI Subgroup of the Early Childhood Work Group, jointly supported by Healthy Eating Research (HER) and the Nutrition and Obesity Policy Research and Evaluation Network (NOPREN). HER is a national program of the Robert Wood Johnson Foundation; NOPREN is supported by Cooperative Agreement Number 5U48DP00498-05 funded by the Centers for Disease Control and Prevention's (CDC) Division of Nutrition, Physical Activity, and Obesity and Prevention Research Centers Program. This project was funded by Healthy Eating Research, a national program of the Robert Wood Johnson Foundation. This work was also funded by NC State Extension and The FEEd Lab at NC State University.
Author Disclosure Statement
No competing financial interests exist
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.