
Abstract
Background:
Obesity is a prevalent medical condition among the pediatric population. Metabolic and bariatric surgery is recommended to treat severe obesity. Resting energy expenditure (REE) plays a vital role in weight homeostasis. This study aims to assess the impact of sleeve gastrectomy (SG) on REE in pediatric patients with severe obesity while comparing REE values with body composition.
Methods:
Participants were recruited from the Pediatric Weight Management Clinic and Bariatric Surgery Clinic at Lucile Packard Children’s Hospital. REE was measured using indirect calorimetry. Body composition was assessed using dual energy X-ray absorptiometry scans. Data were collected prospectively and analyzed using a generalized linear model and correlation analyses.
Results:
Thirty-six participants with severe obesity were included. Correlation analyses showed significant differences in baseline REE/kg between age groups, with higher REE/kg in participants <16 years. No significant correlations were observed between pre-SG REE/kg and degree of weight loss post-SG. Pre-SG %lean body mass positively correlated with REE/kg. There was no significant change in REE/kg following SG with weight loss.
Conclusions:
SG remains an effective intervention for managing severe obesity. This study found no significant changes in REE after SG. Future research should focus on larger longitudinal studies to enhance understanding of the metabolic effects of SG in pediatric patients while optimizing strategies for improved health outcomes.
Background
Obesity is an increasingly prevalent medical condition among the pediatric population. 1 The overall incidence is reported as 19.3% and 20.9% in children and adolescents, respectively, with severe obesity estimated at 7.6%. 2 The American Academy of Pediatrics (AAP) recommends considering metabolic and bariatric surgery (MBS) to treat pediatric patients with severe obesity. 3 Resting energy expenditure (REE) is the metabolic rate required to maintain vital physiological functions of an individual at rest and plays a significant role in weight management. REE can be measured by indirect calorimetry (IC) and is generally expressed in kilocalories per day (kcal/day). REE is often used when developing personalized dietary intervention plans or to estimate calorie needs. 4 Traditionally, REE has been observed to decrease with conventional weight loss methods such as diet and exercise. Given that REE is influenced by body weight, reporting REE in kcal/kg provides a more precise understanding of REE when weight changes occur. 1
The effect of sleeve gastrectomy (SG) on REE is still uncertain in adults and has not been studied in patients under 16 years old.1,5 Previous studies have shown varied results on REE changes after SG, with some reporting increases, decreases, or no changes in REE.5–9 Notably, two studies focusing on individuals 16 years and older showed either no change or a slight increase in REE with limited participants.10,11 This study aims to describe REE profiles in pediatric patients with severe obesity before and after SG, while also comparing REE values with body composition. We believe that findings from this study will offer insights into the metabolic changes following SG in children and adolescents, thereby informing more effective clinical practices and personalized treatment plans for pediatric patients with severe obesity.
Materials and Methods
Participants
Study participants were recruited from the Pediatric Weight Management Clinic and Bariatric Surgery Clinic at Lucile Packard Children’s Hospital between October 2021 and December 2023. All treating physicians were informed about the research study and initially contacted the patients and their guardians during clinical encounters to discuss potential participation in the study (e.g., in the clinic, via telehealth visits, or by telephone). Study participants did not require additional support or compensation for the study as the data were already collected as part of the standard of care. Institutional Review Board approval from Stanford University (ID #60907) was obtained on April 22, 2021. Written informed consent and assent were obtained from all study participants and their guardians prior to enrollment, in accordance with the Declaration of Helsinki.
Inclusion Criteria
All pediatric patients (aged 2–25) with severe obesity receiving care through the Pediatric Weight Management Clinic and Bariatric Surgery Clinic at Lucile Packard Children’s Hospital were invited to participate in the study. Study participants consented to have their data, including IC, dual energy X-ray absorptiometry (DXA) scan, anthropometric measurements, and laboratory values, collected and analyzed.
Study Design and Analysis
IC was performed by the Pulmonary Function Laboratory at Lucile Packard Children’s Hospital, and body composition was measured using DXA scans. Data were collected prospectively. Data were collected from patient’s medical records in Epic and stored in REDCap, a secure and HIPAA-compliant web application for the management of surveys and databases. No additional risks were imposed on study participants. Data analysis was conducted by a biostatistician from the Stanford Quantitative Sciences Unit.
The objective of this study was to analyze changes in energy expenditure following bariatric surgery to better understand the impact of bariatric surgery on metabolism and weight changes. Secondary outcomes included a descriptive analysis of REE values by age and sex assigned at birth, as well as correlations between REE values and body composition (fat and muscle mass). Primary data analyses were performed using a generalized linear model adjusted for sex to compare REE kcal/kg values between participants aged below and above 16 years old, measured versus predicted REE kcal/kg, REE kcal/kg values before and after SG, and baseline REE kcal/kg in relation to degree of weight loss post-SG. Predicted REE was calculated using the Harris-Benedict equation and the Breezing application by the Pulmonary Function Laboratory. A correlation graph was used to determine the relationship between the percentage of fat body mass, percentage of lean body mass, and REE kcal/kg.
Correlations were computed using the Pearson correlation implementation in the Python package (Version 3.7.7) and SciPy (Version 1.5.0). Differences in energy expenditure (REE kcal/kg) below or above 16 years of age were assessed using a generalized linear model implemented in the package statsmodel (0.13.2) and adjusted for sex.
Results
Sixty-two patients were assessed for eligibility. Of these, 15 declined to participate, 4 had incomplete consent forms, and 7 were lost to follow-up due to relocation, change in insurance/healthcare providers, and/or change in care plan. Data were collected from 36 participants with demographic data summarized in Table 1. For the 33 patients who completed IC before SG, the measured mean REE was 2749.7 kcal/day (range 1888–4199 kcal/day) with a predicted mean REE of 2471.6 kcal/day (range 1710–3954 kcal/day). The mean REE for weight was 20 kcal/kg (range 14.2–25.5 kcal/kg). Post-SG (n = 14), the measured mean REE was 2295 kcal/day (range 1589–3670 kcal/day), the predicted mean REE was 2318.2 kcal/day (range 1601–3454 kcal/day), and the mean REE for weight was 19.3 kcal/kg (range 16.1–26.7 kcal/kg). (IC was measured post-operatively between 2 and 10 months with a mean of 5 months.) Baseline DXA scans (n = 36) reported a mean percentage of fat body mass of 49.5% (range 39.8–60.3%), fat mass/ht2 of 25.3 kg/m2 (range 15.5–43.8 kg/m2), and lean mass/ht2 of 24.6 kg/m2 (range 17.7–34.1 kg/m2).
Demographic Characteristics
IC, indirect calorimetry.
Differences in energy expenditure pre-SG (REE kcal/kg) below or above 16 years of age were assessed using a generalized linear model adjusted for sex and showed a significantly higher REE in those <16-year-old compared with >16 years old [REE kcal/kg ∼ Age_group + Sex, βAge_group = −2.0249; 95% confidence interval (−3.844; −0.206), p = 0.029] (Fig. 1). We observed a positive correlation between pre-SG % lean body mass and REE kcal/kg (r2 = 0.541; p = 0.0012). However, a negative correlation was found between pre-SG REE kcal/kg and % fat body mass (r2 = −0.408; p = 0.0183) (Fig. 2). Higher pre-SG REE kcal/kg did not correlate with greater weight loss post-SG (Fig. 3). Lastly, there was no statistical difference between pre- and post-SG REE kcal/kg (n = 14) (Fig. 4).
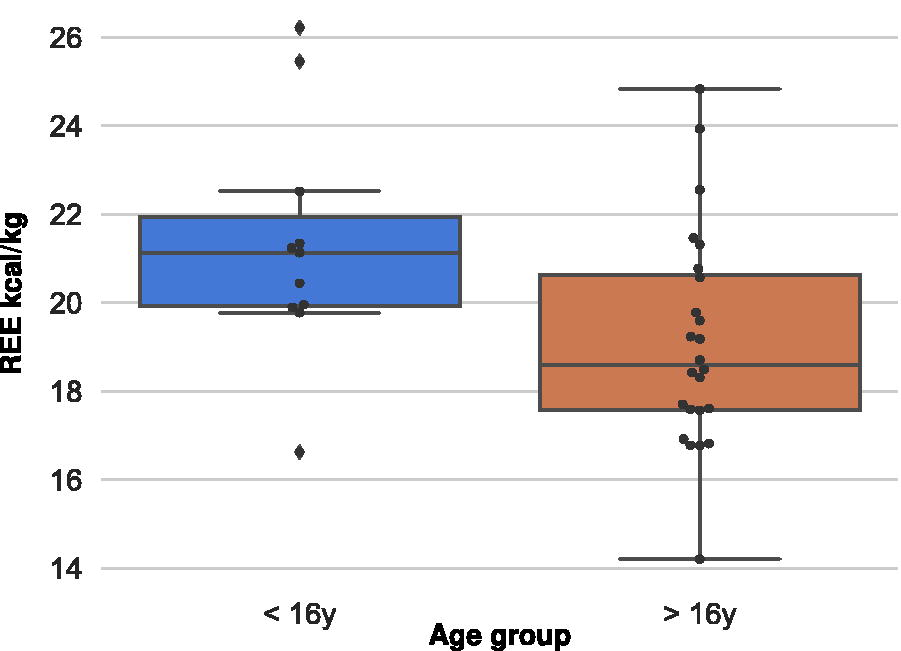
Box and whisker plot of REE kcal/kg pre-sleeve gastrectomy between age groups [REE kcal/kg ∼ Age_group + Sex, βAge_group = −2.0249; 95% confidence interval (CI) (−3.844; −0.206), p = 0.029)]. REE, resting energy expenditure.

Scatter plot of pre-sleeve gastrectomy REE kcal/kg and % body fat mass. , <16 years;  , >16 years;
, >16 years;  , male; ×, female.
, male; ×, female.
Scatter plot of pre-sleeve gastrectomy REE kcal/kg and weight loss post-sleeve gastrectomy. , <16 years; , >16 years; , male; ×, female.
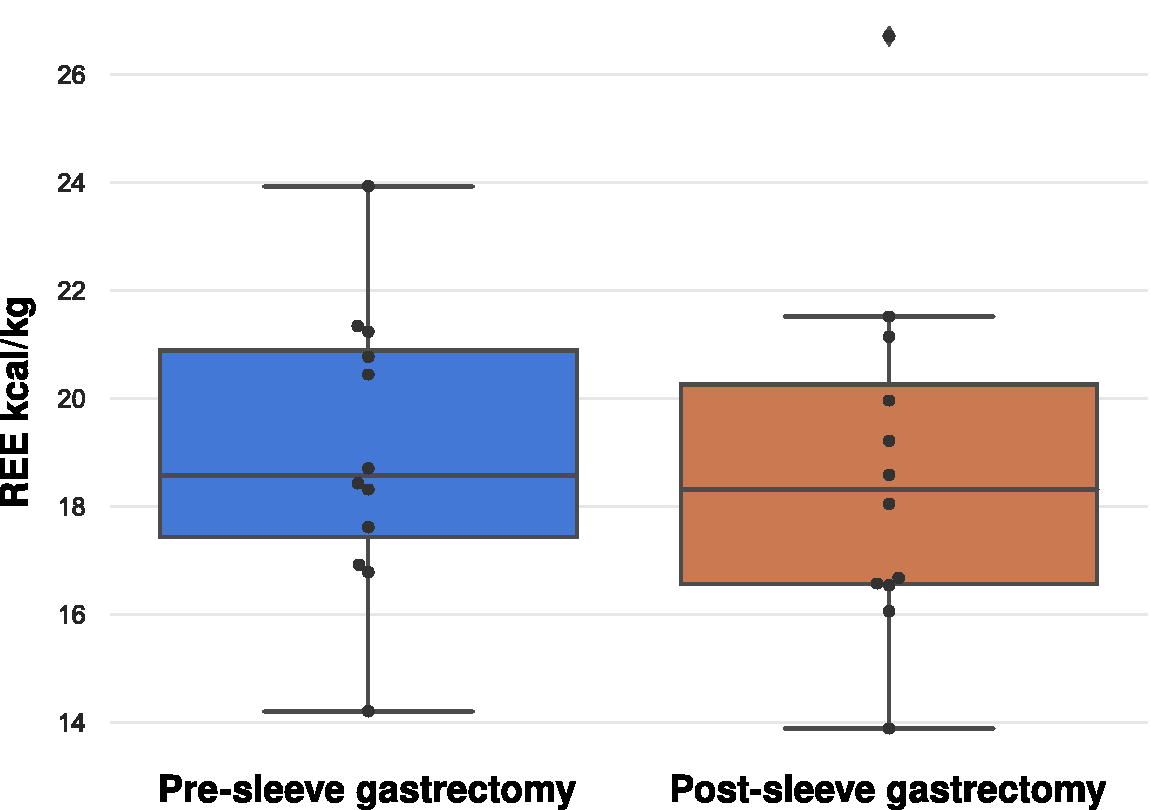
Box and whisker plot of REE kcal/kg before and after sleeve gastrectomy. Paired t-test p-value = 0.69 (N = 14).
Discussion
This study aimed to investigate the changes in REE among pediatric patients with severe obesity who underwent SG and to explore the relationship between REE and body composition. The results provide valuable insights into the metabolic adaptations following SG in a pediatric population, contributing to a better understanding of the impact of bariatric surgery on energy metabolism in this unique demographic.
One of the key observations from this study is the difference in REE between younger and older adolescents. The higher REE observed in younger patients before surgery suggests that metabolic rates may be influenced by age-related factors, including growth and hormonal differences, possibly reflecting the higher energy demands associated with growth and development. In pediatric populations, growth and puberty significantly influence metabolism. 12 These higher baseline metabolic demands related to growth may help sustain REE post-operatively. However, in our study, this increase in REE/kg was not associated with higher weight loss post-SG, making this less of a factor contributing to weight loss. For clinicians, this may suggest that energy intake recommendations and physical activity guidelines should be tailored according to age.
This study also highlights the strong relationship between body composition and REE. Specifically, the positive correlation between lean body mass and REE reinforces the notion that muscle tissue is a primary driver of energy expenditure. This finding aligns with existing literature and suggests that preserving or increasing lean mass should be a key objective in managing pediatric obesity, particularly in the context of bariatric surgery.8–11 Interventions that focus on strength training and maintaining muscle mass may not only help sustain REE but also contribute to better overall health outcomes.
Conversely, the negative correlation between fat mass and REE indicates that higher levels of adiposity may be associated with lower metabolic rates when adjusted for body weight. This highlights the potential metabolic challenges faced by patients with higher fat mass and suggests that these patients may require more intensive post-surgical monitoring and intervention to achieve and maintain weight loss.
The finding that pre-surgical REE does not predict post-surgical weight loss is particularly noteworthy. This suggests that REE alone is not a sufficient predictor of surgical success, and other factors should be considered to predict weight loss outcomes. For researchers, this underscores the need for comprehensive studies that consider a broader range of variables when evaluating the effectiveness of bariatric surgery in pediatric populations.
Strengths and Limitations
Our study was conducted at a single center and was limited by the sample size (n = 36) and therefore may not be generalizable to other populations. Future research could benefit from larger sample sizes, which may be feasible through multicenter collaborations with standardization of follow-up protocols. Post-SG REE was measured at variable time points, introducing heterogeneity in the results. Given the metabolic changes that occur over time, future studies should focus on a longer follow-up period to obtain more insight. Missing data presented additional limitations when participants failed to complete diagnostic tests or care plan modifications occurred. Much of the study period occurred during the COVID-19 pandemic, which impacted data collection as many patients were unable to complete face-to-face follow-up for various reasons. While efforts were made to address this issue, the effects of the pandemic on the data may limit the generalizability of the findings. In addition, this study was conducted as a free-living study, and changes in REE and weight may not be solely due to SG as daily food intake and physical activity were not measured. These two factors are known to influence REE and could potentially confound the results. 13 Therefore, future research should include accounting for daily food intake and physical activity levels to provide a more comprehensive understanding of the mechanisms underlying changes in post-operative REE.
Conclusion
SG continues to be an effective intervention in managing severe obesity and decreasing metabolic risk factors in pediatric populations. Our study demonstrated that the changes in REE/kg following SG were not significant, despite successful weight loss. While our study highlights the importance of accounting for age and body composition when developing obesity treatment plans, it is also crucial to consider and investigate a variety of behavioral and physiological factors in future research. Future studies with larger sample sizes and more frequent or consistent REE measurements that explore the broader metabolic adaptations following SG would be both innovative and essential for understanding weight loss mechanisms. This research could provide valuable insights to optimize patient care and improve health outcomes.
Impact Statement
This is the first study including data from 36 pediatric patients with obesity undergoing SG. Although there was no difference in resting energy expenditure (REE) post-surgery compared with before, we observed higher REE with younger ages and identified that initial REE has no effect on weight loss amount post-surgery.
Footnotes
Acknowledgments
The authors would like to thank Sukhada Vaidya Mairal, Elvi Sanjines, the study participants, and their families for their time and support for this study.
Authors’ Contributions
L.K., M.B., J.S.A.P., and M.A.E.H.: Performed study design and conceptualization. L.K. and M.A.E.H.: Conducted a literature search and data curation. Y.L.G. and M.A.E.H.: Performed data analysis, generation of tables/figures, and data interpretation. L.K., P.K., Y.L.G., and M.A.E.H.: Developed, wrote, and edited the article. M.A.E.H.: Provided supervision for the study. L.K., P.K., Y.L.G., M.B., J.S.A.P., and M.A.E.H.: Reviewed and edited the article.
Data Availability
Data described in the article will not be made publicly available to protect pediatric patient privacy.
Author Disclosures Statement
All authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest. M.B. and J.S.A.P. served as co-directors of the Stanford University Adolescent Metabolic and Bariatric Surgery Program at the time this study was implemented and served as authors for the 2018 ASMBS Pediatric Metabolic and Bariatric Surgery guidelines.
Funding Information
Stanford Maternal & Child Health Research Institute (MCHRI) provided funding for this study but did not have any role or participation in the design, collection, analysis, interpretation, or writing of the article for this study.