
Abstract
Objective :
To characterize the aggregate response benefit with upadacitinib versus dupilumab or placebo in patients with moderate-to-severe AD.
Methods :
Degree of skin clearance and itch response in 3 phase 3 studies (Heads Up [NCT03738397] and Measure Up 1/2 [integrated; NCT03569293/NCT03607422]) were assessed by the Eczema Area and Severity Index (EASI) and Worst Pruritus Numerical Rating Scale (WP-NRS), respectively, using mutually exclusive categories. The aggregate response benefit with upadacitinib over dupilumab or placebo was determined by summing incremental differences for each EASI or WP-NRS category across the full distribution of patient responses.
Results :
Comparisons across EASI improvement threshold distributions, EASI severity levels, and WP-NRS categories demonstrated an aggregate response benefit favoring upadacitinib over dupilumab as early as week 4 and continuing at weeks 16 and 24. Similar trends were observed for upadacitinib 15 and 30 mg versus placebo.
Conclusions :
The aggregate response benefit in skin clearance and itch reduction favored upadacitinib 30 mg over dupilumab and upadacitinib 15 or 30 mg over placebo. These benefits may translate to overall greater improvements in patient QoL.
Capsule Summary
We report a unique method to compare differences in efficacy between treatment groups from clinical studies across the full range of clinical responses for multiple binary assessment categories and summarize the differences between 2 treatments as a single metric, an aggregate response benefit.
Incremental differences and aggregate response benefits favor upadacitinib over dupilumab across nearly all skin-clearance and itch-reduction categories.
Higher aggregate response benefit for upadacitinib over dupilumab as early as week 4 highlights the rapid onset of skin clearance and itch reduction with upadacitinib.
Brief Summary
Using a novel method to assess efficacy, aggregate response benefit, upadacitinib was favored across the full range of clinical response over dupilumab or placebo
INTRODUCTION
Atopic Dermatitis® (AD) is a chronic inflammatory disease characterized by numerous skin manifestations including skin sensitivity and dry skin, eczematous lesions, and intense pruritus.1,2 AD is associated with substantial disease burden that limits participation in activities and impairs psychosocial health and health-related quality of life (QoL) of both patients and their families.1–4 Severity of AD was also linked with higher disease burden. In surveys of patients with AD, those with higher disease severity reported a greater negative effect on their lives and higher therapeutic needs.3,4 Greater improvements in skin clearance and itch, which patients with AD reported as highly important, 5 are associated with greater improvements in health-related QoL. 6
AD can be challenging to treat, and systemic therapies are required for patients with moderate-to-severe AD whose symptoms are not sufficiently managed with topical and phototherapies. Dupilumab is a subcutaneously administered monoclonal antibody that inhibits interleukin 4 and interleukin 13 and is approved for the treatment of moderate-to-severe AD.7,8 In 2 phase 3 trials evaluating the efficacy of dupilumab versus placebo (SOLO 1 and SOLO 2), dupilumab demonstrated greater efficacy for both itch and skin clearance endpoints than placebo after 16 weeks of treatment. 7
Upadacitinib is an oral selective Janus kinase (JAK) inhibitor with greater potency for JAK1 than for JAK2, JAK3, or tyrosine kinase 2.9,10 In phase 3 studies, upadacitinib demonstrated greater efficacy in itch and skin clearance endpoints both with and without concomitant topical corticosteroid therapy in adults and adolescents with moderate-to-severe AD than placebo over 16 weeks of treatment.11,12 Upadacitinib 30 mg also demonstrated superiority over dupilumab through 16 weeks of treatment in adults with moderate-to-severe AD in the phase 3 Heads Up study. 13
Clinical trials evaluating patients with AD typically compare efficacy across treatment groups using prespecified mutually exclusive binary assessments (eg, ≥75% improvement in Eczema Area and Severity Index [EASI 75]), often over varying response levels (eg, EASI 50, EASI 75, EASI 90, and EASI 100). However, efficacy characterized over a series of binary assessments may convolute the overall response benefit across the polychotomous efficacy distribution (ie, across the full range of clinical responses for multiple binary assessment categories).
For example, 2 treatments may have similar EASI 50 response rates, yet Treatment A may have a higher EASI 75 response rate than Treatment B, whereas Treatment B may have a greater EASI 90 response rate than Treatment A (Fig. 1). Similarly, 1 treatment may provide substantially greater efficacy over another, though the total benefit may be less clear when fragmented across multiple binary assessment comparisons. Characterizing the total aggregate response benefit across the whole polychotomous efficacy distribution can help mitigate these challenges.
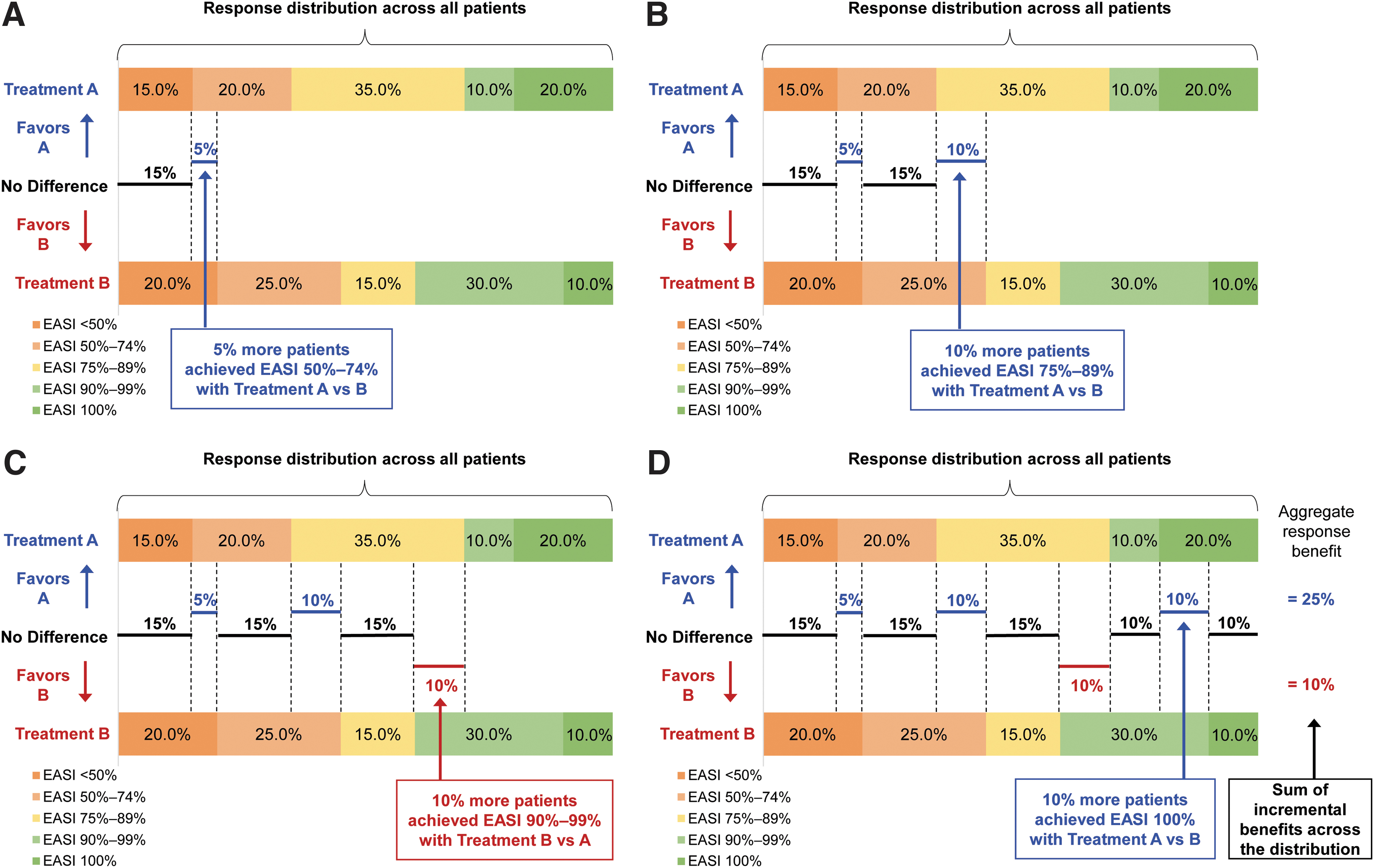
Explanation of incremental and aggregate response benefit calculations. (A) Incremental response benefit for EASI 50%–74%; (B) incremental response benefit for EASI 75%–89%; (C) incremental response benefit for EASI 90%–99%; (D) incremental response benefit for EASI 100% and overall aggregate response benefit. EASI, Eczema Area and Severity Index.
Herein we propose an approach to assess the aggregate response benefit by evaluating incremental differences across polychotomous efficacy distributions, then apply this method to describe the benefits of upadacitinib compared with dupilumab and placebo in skin clearance and itch reduction using data from phase 3 clinical trials. These data are important for informing shared decision making between health care providers and their patients.
METHODS
Patients, Study Design, and Treatment
In this post hoc analysis, we evaluated data from 3 multicenter phase 3 studies investigating the efficacy of upadacitinib in patients with moderate-to-severe AD: Heads Up (NCT03738397), 13 Measure Up 1 (NCT03569293), 11 and Measure Up 2 (NCT03607422). 11 Study designs and eligibility criteria were previously described.11,13 In the Heads Up study (a double-blind double-dummy active-controlled study), patients were randomized 1:1 to receive upadacitinib 30 mg or dupilumab 300 mg for 24 weeks. 13
In Measure Up 1 and Measure Up 2 studies (double-blind placebo-controlled studies), patients were randomized 1:1:1 to receive upadacitinib 15 mg, upadacitinib 30 mg, or placebo for 16 weeks. 11 Data from the Measure Up 1 and Measure Up 2 studies were pooled for this analysis (Measure Up 1/2). The study protocol was reviewed and approved by central and local independent ethics committees and/or institutional review boards at each study site, and patients provided written informed consent.
Assessments
The degree of skin clearance was assessed by the percent improvement from baseline in EASI at weeks 4, 16, and 24 for patients in the Heads Up study and at week 16 for patients in the Measure Up 1/2 studies. Skin clearance efficacy distributions were partitioned into 5 mutually exclusive categories using EASI improvement thresholds commonly used in clinical studies: EASI <50%, EASI 50%–74%, EASI 75%–89%, EASI 90%–99%, and EASI 100%. Similarly, absolute EASI scores were categorized using the following EASI severity thresholds: clear (EASI 0), almost clear (EASI 0.1–1.0), mild (EASI 1.1–7.0), moderate (EASI 7.1–21.0), and severe (EASI >21.0). 14
Itch was assessed by Worst Pruritus Numerical Rating Scale (WP-NRS) scores at baseline and at weeks 4, 16, and 24 (Heads Up study) or at week 16 (Measure Up 1/2 studies) and partitioned using mutually exclusive severity categories informed by thresholds previously used in the literature: moderate-to-severe (≥4), mild (2–3), and absent/minimal (0–1).15–17
Calculating the Aggregate Response Benefit
The aggregate response benefit of 1 treatment over another was calculated by summing the incremental differences between the polychotomous efficacy distributions of the 2 treatment groups. This procedure is summarized in Figure 1. In this hypothetical example, 15% and 20% of patients achieved EASI <50% with Treatment A or Treatment B, respectively. Therefore, the bottom 15th percentile of patients had the same outcome, regardless of which treatment they received (EASI <50%); the next 5% of patients achieved the next higher response level with Treatment A (EASI 50%–74%) than with Treatment B (EASI <50%), demonstrating a 5% incremental difference favoring Treatment A over Treatment B (Fig. 1A).
Continuing this process for the next response level (ie, EASI 50%–74%), there is a 10% incremental difference favoring Treatment A over Treatment B (Fig. 1B). However, for the next response level (EASI 75%–89%), there is a 10% incremental difference favoring Treatment B over Treatment A (Fig. 1C). Finally, when considering EASI 90%–99%, there is a 10% incremental difference favoring Treatment A over Treatment B (Fig. 1D). Summing these incremental differences across the entire distribution results in an aggregate response benefit 25% for Treatment A and 10% for Treatment B; the difference between these 2 values yields a total aggregate response benefit of 15% in favor of Treatment A.
For skin clearance, the aggregate EASI response benefit between patients who received upadacitinib 30 mg daily and those who received dupilumab 300 mg every other week (in the Heads Up study) or those who received upadacitinib 15 mg or placebo (in the Measure Up 1/2 studies) was calculated. This procedure was also applied to assess itch, using WP-NRS score categories of 0–1, 2–3, and 4+ to calculate the aggregate itch response benefit.
Statistical Analysis
Data were descriptively reported, with no statistical comparisons between treatment groups or response categories. Nonresponder imputation incorporating multiple imputation to handle missing data due to COVID-19 was used for handling intercurrent events (ie, the occurrence of rescue medication use) and missing data.
RESULTS
Patients
A total of 673 patients were randomized in the Heads Up study (upadacitinib, n = 342; dupilumab, n = 331) and 1683 patients were randomized in the Measure Up 1/2 studies (integrated; upadacitinib 15 mg, n = 557; upadacitinib 30 mg, n = 567; placebo, n = 559). Patient demographics and baseline characteristics were consistent across treatment groups in each study, as previously reported.11,13 In the Heads Up study, baseline EASI and WP-NRS scores were similar across treatment groups and substantially improved by weeks 4, 16, and 24 with numerically lower EASI and WP-NRS scores (ie, greater improvement) with upadacitinib 30 mg than with dupilumab (Table 1).
Absolute Eczema Area and Severity Index and Worst Pruritus Numerical Rating Scale Scores by Treatment Group (the Heads Up Study; Observed Cases)
DUPI, dupilumab; EASI, Eczema Area and Severity Index; SD, standard deviation; UPA, upadacitinib; WP-NRS, Worst Pruritus Numerical Rating Scale.
Similarly, in the Measure Up 1/2 studies, EASI and WP-NRS scores were comparable at baseline across treatment groups with substantially lower scores by weeks 4 and 16 with upadacitinib 30 mg or upadacitinib 15 mg than with placebo (Supplementary Table S1).
Aggregate Skin Clearance Benefit With Upadacitinib
Comparisons across the distribution of EASI thresholds demonstrated differences favoring upadacitinib over dupilumab as early as week 4 of the Heads Up study (Fig. 2). A larger proportion of patients achieved incrementally greater skin clearance with upadacitinib than with dupilumab across all the EASI thresholds. The aggregate response benefit of upadacitinib 30 mg treatment at week 4 compared with dupilumab treatment was 79.3%. Although EASI improvements among patients receiving dupilumab were numerically higher at weeks 16 and 24 relative to week 4, the total proportion of patients who achieved greater skin clearance across EASI thresholds with dupilumab was 59.6% and 27.3% lower relative to upadacitinib 30 mg at weeks 16 and 24, respectively. There were no instances across thresholds where dupilumab treatment resulted in incrementally greater skin clearance.
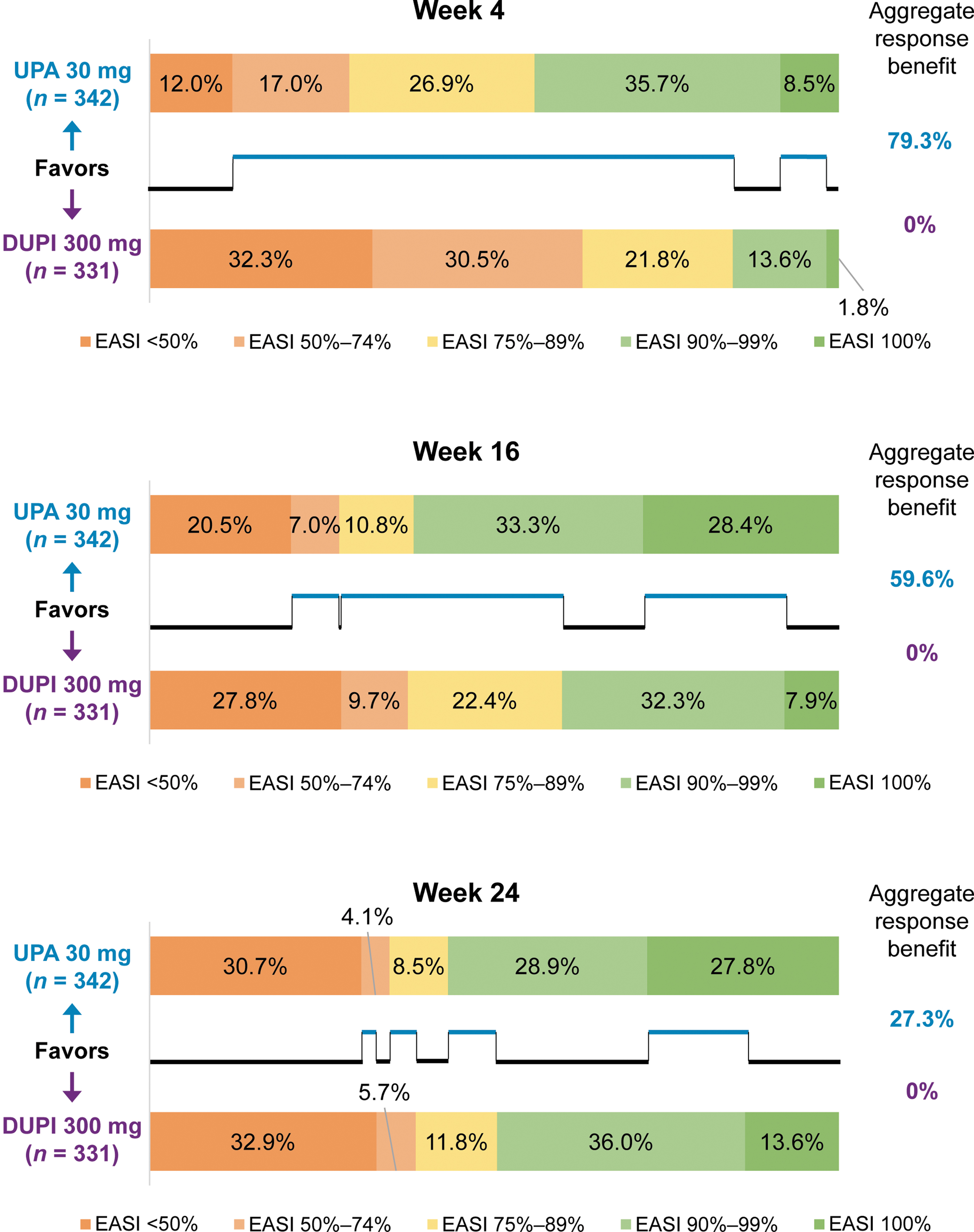
Differences in response across EASI threshold increments and aggregate response benefit in skin clearance with upadacitinib 30 mg compared with dupilumab. Missing data imputed using nonresponder imputation incorporating multiple imputation to handle missing data due to COVID-19. DUPI, dupilumab; EASI, Eczema Area and Severity Index; UPA, upadacitinib.
In the Measure Up 1/2 studies, a larger proportion of patients achieved incrementally greater skin clearance at week 16 with either dose of upadacitinib than with placebo across all the EASI thresholds (Supplementary Fig. S1). The aggregate response benefit across the EASI threshold increments with upadacitinib 15 mg and 30 mg over placebo at week 16 was 74.6% and 82.5%, respectively. Patients receiving either dose of upadacitinib experienced significant improvement in EASI compared with placebo (EASI 75: upadacitinib 15 mg, 64.9%; upadacitinib 30 mg, 76.3% vs placebo, 14.8%; P < 0.001 for both comparisons), and the total proportion of patients who achieved greater skin clearance across EASI thresholds with upadacitinib 30 mg was 41.0% higher relative to upadacitinib 15 mg.
Analogous results were observed when comparing distributions of absolute EASI scores by severity. At 4 weeks of the Heads Up trial, a larger proportion of patients achieved incrementally greater skin clearance with upadacitinib 30 mg than with dupilumab (Fig. 3). The aggregate response benefit of upadacitinib at weeks 4 and 16 was 59.0% and 55.9% higher, respectively, relative to dupilumab. At week 24, the aggregate response benefit across absolute EASI thresholds was 32.5% higher with upadacitinib 30 mg compared with dupilumab (aggregate response benefit of 33.6% for upadacitinib and 1.1% for dupilumab).
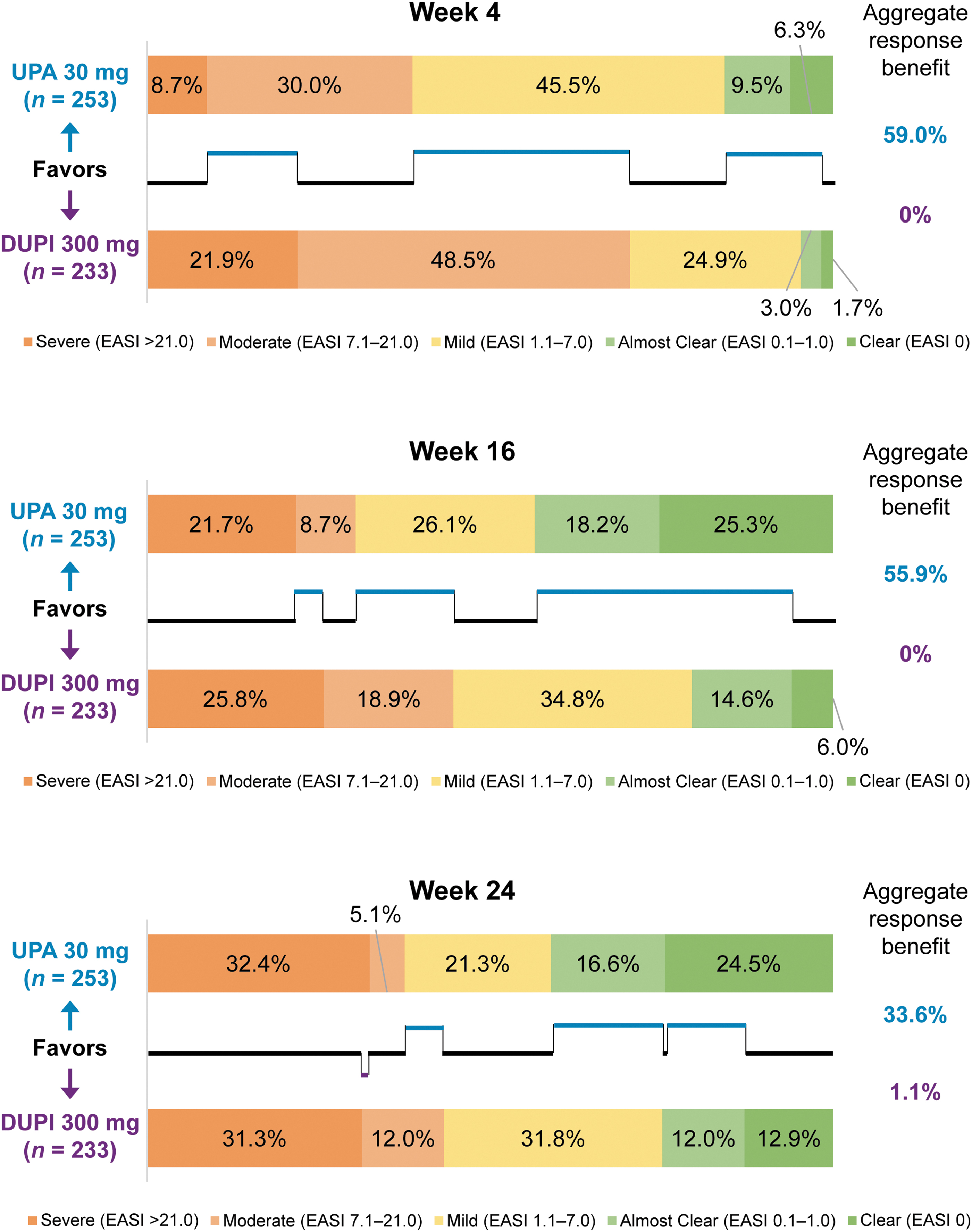
Differences in response across EASI severity level categories and aggregate response benefit in skin clearance with upadacitinib 30 mg compared with dupilumab. Missing data imputed using nonresponder imputation incorporating multiple imputation to handle missing data due to COVID-19. DUPI, dupilumab; EASI, Eczema Area and Severity Index; UPA, upadacitinib.
Distribution comparisons across EASI severity categories at week 16 of the Measure Up 1/2 studies also showed incrementally greater skin clearance for upadacitinib versus placebo. At week 16, the aggregate response benefit of upadacitinib 15 mg and 30 mg over placebo was 77.7% and 85.3%, respectively (Supplementary Fig. S2). The total proportion of patients who achieved greater skin clearance across absolute EASI thresholds with upadacitinib 30 mg was 38.8% higher relative to upadacitinib 15 mg.
Aggregate Itch Benefit With Upadacitinib
Distribution comparisons across absolute WP-NRS scores also demonstrated incremental benefits favoring upadacitinib over dupilumab across all the itch categories (Fig. 4). At week 4, the aggregate response benefit across the WP-NRS score distribution was 56.5% higher with upadacitinib 30 mg relative to dupilumab. By week 24, the aggregate response benefit for itch was 25.8% higher with upadacitinib 30 mg than with dupilumab.

Differences in response across itch categories and aggregate response benefit in itch reduction with upadacitinib 30 mg compared with dupilumab. Missing data imputed using nonresponder imputation incorporating multiple imputation to handle missing data due to COVID-19. DUPI, dupilumab; UPA, upadacitinib; WP-NRS, Worst Pruritus Numerical Rating Scale.
Greater incremental itch reductions were also observed with upadacitinib than with placebo; distribution comparisons for WP-NRS categories at week 16 demonstrated an aggregate response benefit of 46.1% for upadacitinib 15 mg and 59.3% for upadacitinib 30 mg over placebo (Supplementary Fig. S3).
DISCUSSION
Comparisons across skin clearance and itch distributions demonstrated incremental differences and aggregate response benefits favoring upadacitinib 30 mg over dupilumab for nearly all categories of skin clearance and itch reduction assessed in this analysis. A higher proportion of responders was reported with upadacitinib 30 mg than with dupilumab for almost every one of the binary assessments for skin clearance and itch reduction at weeks 4, 16, and 24, suggesting a more robust response with upadacitinib, regardless of the degree of skin clearance achieved.
Taken together, the directional findings of these binary assessments align with the results demonstrating aggregate response benefits for upadacitinib 30 mg over dupilumab, suggesting a greater treatment benefit with upadacitinib across the entire response spectrum through a single metric. Higher aggregate response benefits for upadacitinib 30 mg over dupilumab at week 4 also highlight the rapid onset of skin clearance and itch reduction with upadacitinib, which is an important clinical benefit desired by patients with AD. 4
Our results demonstrate consistently favorable and clinically meaningful benefits (ie, differences in clinically relevant response categories such as EASI 75 vs EASI 90) for upadacitinib across the entire distribution of EASI thresholds and EASI severity levels, with similar trends observed across the entire distribution of itch categories in this study. The higher aggregate response benefits for skin clearance and itch reduction observed with upadacitinib in this study may translate into more profound improvements in overall health-related QoL and greater treatment benefit, given that correlations between higher clinical response and greater QoL improvements were previously reported.6,18
Our findings demonstrating incrementally greater responses for itch reduction with upadacitinib are especially valuable given that itch reduction was reported as the number 1 treatment goal in a cross-sectional study evaluating health-related QoL in patients with AD. 4
We developed a novel method to simplify evaluation of treatment differences across multiple clinical response thresholds. This method generates a descriptive metric describing the difference between 2 groups in a setting where the outcomes are ordinal, which complements the traditional approach of conducting comparisons between each level. With this method, differences between 2 treatments are calculated across several response levels for a particular clinical index and summed to calculate the overall benefit when using 1 treatment compared with the other.
Statistical analyses comparing percentiles between 2 treatment groups are commonly performed (eg, comparing medians); our unique approach builds on that practice by allowing for comparisons between percentiles across the entire polychotomous distribution and summarizing differences into a single metric (aggregate response benefit). This approach makes it easier to understand the overall differences between 2 treatment options across clinically relevant response levels rather than evaluating multiple binary assessments. The magnitude of differences is not considered in this method; refinements to the approach to accommodate magnitude are a potential area of future research.
Further study is also needed to evaluate the statistical properties and validity of this metric, including how it may be used for statistical inference. In our analysis, treatment with upadacitinib led to a shift of the overall distribution of responses; that is, most patients achieved an improved clinical response over dupilumab or placebo, even if they did not achieve specific binary thresholds of response. In the future, this method could be used across a wide range of clinical applications: to conduct pairwise comparisons among other AD therapies, to evaluate differences on other outcome measures, or to assess differences of treatments in other disease states.
Herein we present findings of the first analysis demonstrating aggregate response benefit across the entire distribution of clinical responses to upadacitinib. Our results are consistent with those from a recent meta-analysis, 19 which concluded that once-daily upadacitinib 30 mg was the most efficacious treatment for moderate-to-severe AD at the time of the primary endpoint (weeks 12 or 16) and at earlier timepoints, followed by once-daily upadacitinib 15 mg and once-daily abrocitinib 200 mg. 19 The methods we used in this study may facilitate easier communication of clinical trial data between health care providers and their patients and aid shared decision making to design individualized treatment plans and improve patient adherence and clinical outcomes.
Our results are limited to the thresholds selected for this study; although the included EASI thresholds are well established and widely used, a decision to include or not include any one of them (eg, EASI 50) would change the ultimate results. Similarly, different aggregate response benefits may be observed if more granular thresholds are applied (EASI 80, EASI 85, etc.). Furthermore, the methods used for evaluating the aggregate response benefit do not consider the magnitude of the difference and only consider whether 1 response for each group is higher or lower than the other.
Other limitations of this study include the post hoc nature of the analysis and relative short study durations (16–24 weeks). Skin clearance and itch reduction by sex, age, or other baseline characteristics were not assessed in this study. Safety was not evaluated in this analysis; however, safety data from the Heads Up study and Measure Up 1/2 studies were previously reported.11,13,20 The results presented herein are descriptive; statistical comparisons between treatments and improvement categories were not performed.
Clinical responses are also generally higher in head-to-head studies than in placebo-controlled trials. In addition, head-to-head comparisons between upadacitinib 15 mg and dupilumab were not performed. Finally, patient adherence to oral medications can be a challenge, which may affect the generalizability of these findings.
Overall, greater proportions of patients with moderate-to-severe AD achieved higher thresholds of skin clearance and itch reduction with once-daily upadacitinib 30 mg than with dupilumab (in the Heads Up study) and with upadacitinib 15 mg and 30 mg than placebo (in the Measure Up 1/2 studies). When considering the full distribution of response levels, the aggregate response benefit of upadacitinib 30 mg compared with dupilumab was most prominent at week 4 (>50% for both skin clearance and itch reduction) and persisted with a reduced difference through week 24 (>25% for both skin clearance and itch reduction).
Achieving substantial levels of skin clearance and itch reduction with upadacitinib is likely to translate into overall QoL improvements for patients with AD. These findings may aid shared decision making between health care providers and their patients in the development of individualized treatment plans.
SUPPLEMENTARY MATERIAL
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.