
Abstract
Background:
Delayed-onset muscle soreness (DOMS) is a serious problem for people who do not exercise on a regular basis. Although the best preventive measure for diabetes and for maintaining a low hemoglobin A1c is exercise, muscle soreness is common in people with diabetes. For people with diabetes, DOMS is rarely reported in exercise studies.
Research Design:
One hundred twenty subjects participated in three groups (young, older, and type 2 diabetes) and were examined to evaluate the soreness in the abdominal muscles after a matched exercise bout using a p90x exercise video (Beachbody LLC, Los Angeles, CA) for core fitness. Next, three heating modalities were assessed on how well they could reduce muscle soreness: ThermaCare® (Pfizer Consumer Healthcare, Richmond, VA) heat wraps, hydrocollator heat wraps, and a chemical moist heat wrap.
Results:
The results showed that people with diabetes were significantly sorer than age-matched controls (P < 0.05). On a 100-mm VAS (100 mm = sorest), the average soreness for the people with diabetes was 73.3 ± 16.2 mm, for the older group was 56.1 ± 15.1 mm, and for the younger group was 41.5 ± 9.3 mm; these differences were significant (analysis of variance, P < 0.05). The greatest reduction in soreness after applying the modalities was using moist heat, both immediately after the modality and up to 2 days after the exercise. Right after the modality, moist heat reduced pain by 52.3% in the older subjects compared with 30.5% in the subjects with diabetes and 33.3% in the younger subjects. Skin blood flow in the abdominal area before exercise was greatest in the younger subjects and lower in the subjects with diabetes after heat application. Skin temperature at rest and after exercise was greatest in the diabetes group.
Conclusions:
Muscle soreness following exercise was greatest in people with diabetes, and the best modality of the three studied to reduce this type of soreness was chemical moist heat.
Introduction
Much is known about DOMS in young people, but little is known about DOMS in people with diabetes. Although the best preventive measure for diabetes and for maintaining a low hemglobin A1c is exercise, muscle soreness is common in people with diabetes without exercise. It is rarely reported in exercise studies in people with diabetes as well as any report of therapeutic means of minimizing soreness. Because cellular damage and repair are linked to tissue blood flow, 8,9 soreness should be worse and recovery longer in people with diabetes because of endothelial dysfunction.
A common defect in type 2 diabetes is impaired endothelial function, 10 –14 including reduced tissue blood flow and impaired blood flow response to stress. This is due to damage to endothelial nitric oxide synthetase or high concentrations of cellular free radicals. Both nitric oxide and prostacyclin (vasodilators released by vascular endothelial cells) are reduced in people with diabetes. 15 –19 The overall effect is reduced blood flow to tissue and impaired tissue healing. 8,9,20 –23 It might be expected that DOMS would be worse in people with diabetes, especially because nerve hypersensitivity can also be found in people with diabetes. 24 This becomes important to understand because the best method of reducing the effects of diabetes is exercise. 25
Although DOMS has been poorly studied in people with diabetes, there may be some comparisons that can be made from studies of DOMS and aging. 6 DOMS is greater in older compared with younger individuals, as is the muscle damage associated with even a single bout of exercise. 6,26 –28 There is evidence that proteolytic activity is reduced and production of free radicals is elevated in older individuals. 6,28 This elevated muscle damage prolongs healing time after excessive exercise. 6 With metabolic impairment and higher levels of free radicals in people with diabetes, 18 DOMS should be even more severe in this population than with aging alone.
Various strategies have been used to reduce DOMS. These include massage, heat, and ingestion of vitamin E and branched-chain amino acids, as well as other modalities. 29 In the present investigation we examined (1) DOMS in people with diabetes compared with controls and (2) the effect of three different heat modalities on reducing DOMS. The heat modality used most commonly clinically is hydrocollator heat wraps. 30 This local heat source reduces cytokines and pain. 31 –33 However, hydrocollator heat wraps are a clinical tool that cannot be used at home. A nonclinical alternative to proving heat at home is chemical, dry heat wraps, such as ThermaCare® (Pfeizer Consumer Healthcare, Richmond, VA) heat wraps. 34,35 Continuous low-level heat wrap therapy has also been shown to reduce acute, nonspecific low back pain, with results of greater pain relief, less muscle stiffness, and increased flexibility on day 1 of pain onset. 4,5 The increase in tissue temperature also promotes healing. However, recent articles show a newer modality for home use using a chemical moist heat source. 36 –38 Unlike hydrocollator heat wraps, these chemical heat wraps apply moist heat directly to the skin where latent and conductive heat provides rapid heat transfer deep into tissue. 37,38 Hydrocollator heat packs (Chattanooga E1, Chattanooga, TN) produce moisture, but much of the moisture is buffered by the six to eight layers of towels under the wraps. This mixes moist heat with conductive heat such that pure moist heat on the skin is not present. 38,39 In the present investigation, these three heat sources were compared on controls and people with diabetes to determine which gave the best pain relief.
Subjects and Methods
There were 120 subjects in this study. These were divided into three cohorts of 40 subjects. Within each cohort, subjects were divided randomly by random number table into four groups: 10 subjects to test dry heat (ThermaCare), 10 to test hydrocollator heat (a silica pack placed in 49°C water), 10 to test chemical moist heat (ThermaCare 24 cell product), and 10 controls for whom no heat was applied. The three cohorts were younger subjects, older subjects, and subjects with diabetes. All groups were at similar fitness levels. Younger subjects were in the age range of 20–45 years old, older subjects were 45–70 years old, and subjects with diabetes were 45–70 years old. All subjects in the younger and older cohorts were free of cardiovascular disease, neurological injuries/disease, or present orthopedic injuries. None of the subjects was taking any type of β-agonist or -antagonists or α-agonists or -antagonists. Subjects were excluded if they were hypertensive (maximum blood pressure, 145/90 mm Hg) or hypotensive (blood pressure less than 90/50 mm Hg) or if they were diagnosed with an impaired circulatory disease such as Raynaud's syndrome. All subjects were fit enough to follow a 16-min abdominal workout (Ab Ripper X; Beachbody LLC, Los Angeles, CA) and a 44-min core workout (Core Synergistics, Beachbody LLC) as described below. In the diabetes cohort, diabetes was controlled, and the average hemoglobin A1c was 7.4 ± 2.3%. The subjects had minimal cardiovascular disease and were within the same blood pressure range but could be taking renin or angiotensin converting enzyme inhibitors but not α- or β-blockers. The general characteristics for the subjects are given in Tables 1 –3. All protocols and procedures were approved by the Institutional Review Board of Azusa Pacific University (Azusa, CA), and all subjects signed a statement of informed consent.
BMI, body mass index.
BMI, body mass index.
BMI, body mass index.
Exercise video
The p90X is a series of exercise videos designed for both men and women that has been sold on television and in stores for the past several years (Beachbody LLC). The DVD includes 12 different exercise videos with various individuals doing each exercise differently, so the user could select low- or high-intensity variations of the exercise depending on their capability. Two workout videos (Core Synergistics and Ab Ripper X) were selected to emphasize the abdominal, low back, and hip flexor regions. The first video, Core Synergistics, lasted 44 min, followed by the Ab Ripper X video, which lasted 16 min, giving a 60-min total workout.
Skin temperature
Skin temperature was measured using a Flir (Stockholm, Sweden) thermal camera (model TC660). The thermal image was taken of their abdominal region from approximately 1 m away and perpendicular to the skin. A thermocouple was used to check the temperature readings of the thermal camera at one skin location. The thermocouple was a type T thermocouple, which was connected to an IsoThermix (Columbus Instruments, Columbus, OH) to analyze and record the temperature. The IsoThermix was calibrated in a water bath prior to the experiments and checked against a standard thermometer. The thermal images were used to assess temperature at the same points that blood flow was measured as described below.
Skin blood flow
Skin blood flow was measured using a BioPac 150 system and an LDF100C laser Doppler blood flow module (BioPac Systems, Goleta, GA). The probe used was a TSD140. Skin blood flow was measured for 10 s at four locations: 2 cm below, to the left and to the right, and 4 cm above the umbilicus. The subjects were asked not to talk and to avoid movement while skin blood flow data were being collected. The repeatability of this flow probe was ±10%.
Heat modalities
Three heat modalities were used. For dry heat, a ThermaCare heat wrap was used. Hydrocollator heat packs, which are common in physical therapy settings, were also used. The silica-filled hydrocollator packs, heated in 49°C water, were wrapped in four towel layers prior to application on the subject. For moist heat, a chemical pack using iron oxidation similar to ThermaCare heat wraps was used, but it released moisture rather than dry heat.
All heating modalities were applied to a central location on the abdominal region. Moist heat and dry heat were applied for 1 h, whereas hydrocollator heat was applied for 30 min as is normally used clinically.
Comfort and soreness visual analog scale
Two visual analog scale (VAS) instruments were used to assess subjective soreness and comfort the day after the p90X video was completed. Each form had a 100-mm-long line marked with “not sore at all” and “extremely sore” at opposite ends. Each participant was directed to make a vertical slash along the 100-mm line to indicate his or her answer to each question. One VAS was for comfort of the modality, and the other was for soreness in the abdominal muscles.
Procedures
Subjects first rested for 15 min in a thermally neutral room. Baseline data were then collected on the abdominal area, including a thermal image, blood flow, and soreness VAS. They then participated in a 60-min workout video. All subjects were asked to attempt the most difficult variation of each exercise that they could. Subjects were given four 3-min breaks throughout the video to drink water and rest. All subjects were told that they were allowed to stop participation at any time, if the exercises became too strenuous. Heart rate was not used to monitor intensity.
Twenty-four hours post-exercise, thermal images of their abdomen and skin blood flow were measured. Each subject in the three cohorts was randomly placed into one of four groups (control, hydrocollator, dry, or chemical moist). For the controls, no heat was administered. Once the thermal image and skin blood flow was taken, each subject was given a plinth on which to lie and filled out the first VAS. The control group was asked to remain lying supine on the plinth for the duration of 2 h. They filled out the next set of VAS at 60 and 120 min. The moist and dry heat groups were asked to lie supine, and a heat pack was applied to their abdominal region. As with the control group, VAS instruments were filled out at the same time intervals. The hydrocollator group lay supine and had a hydrocollator pack placed on their abdomen with a total of four towel layers. They also filled out the VAS pre- and post-modality. For all groups, a comfort VAS was filled out along with the soreness VAS, and abdominal thermal photos and skin blood flow readings were retaken post-modality. VAS scores, skin temperature, and blood flows were repeated at 48 h.
Data analysis
Data analysis involved means, SDs, t tests, and analysis of variance (ANOVA). The level of significance was P < 0.05.
Results
Skin temperature
The results of the determination of skin temperature are shown in Figures 1 –3. As shown in Figure 1 for the younger group, skin temperature was, on average, 0.82°C higher 24 h after the exercise; this increase was significant (P < 0.01). Skin temperature did not change significantly after the next 2-h period for the control group, but for the hydrocollator group the temperature immediately decreased after the modality was removed by 5.7 ± 2.3°C. This decrease was significantly more than in the ThermaCare and moist heat groups (P < 0.05). Two hours after the modalities were applied (as shown in Fig. 1), the greatest skin temperature was in the moist heat group, for which temperatures were still 3.4 ± 1.3°C higher than the pre-modality data. By 2 days, skin temperatures were almost back to the starting temperatures for all groups.
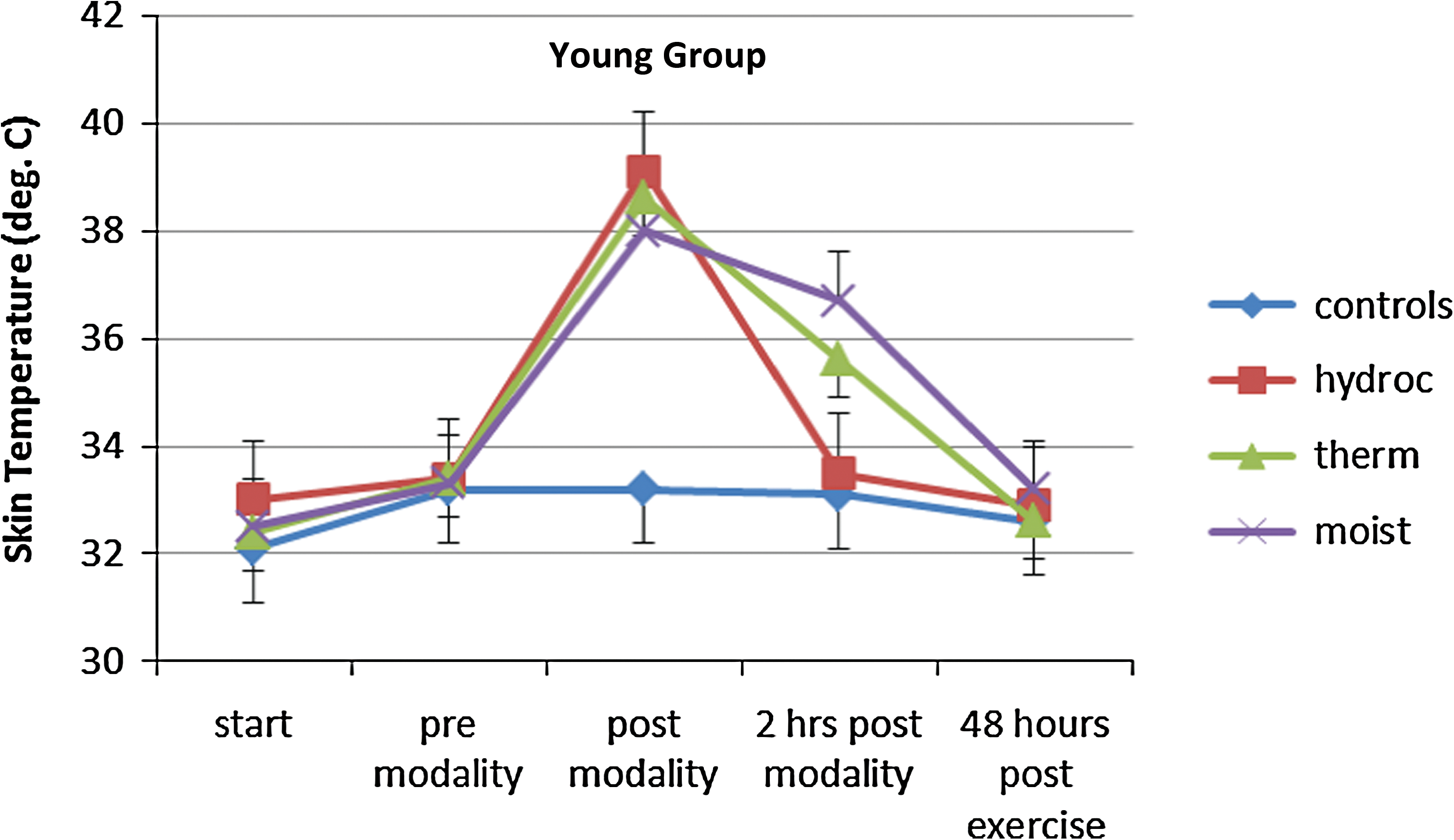
Skin temperature in the younger group of subjects measured with a thermal camera for 10 control subjects (diamonds), 10 subjects who used hydrocollator heat wraps (squares), 10 subjects who used ThermaCare heat wraps (triangles), and 10 subjects who used moist heat wraps (×) before exercise (start), 24 h after exercise and before the modality was applied (pre modality), after the modality was applied (post modality), 2 h after the modality was applied, and 48 h after the exercise measured at four locations on the abdominal area. Data are mean ± SD values. Color images available online at
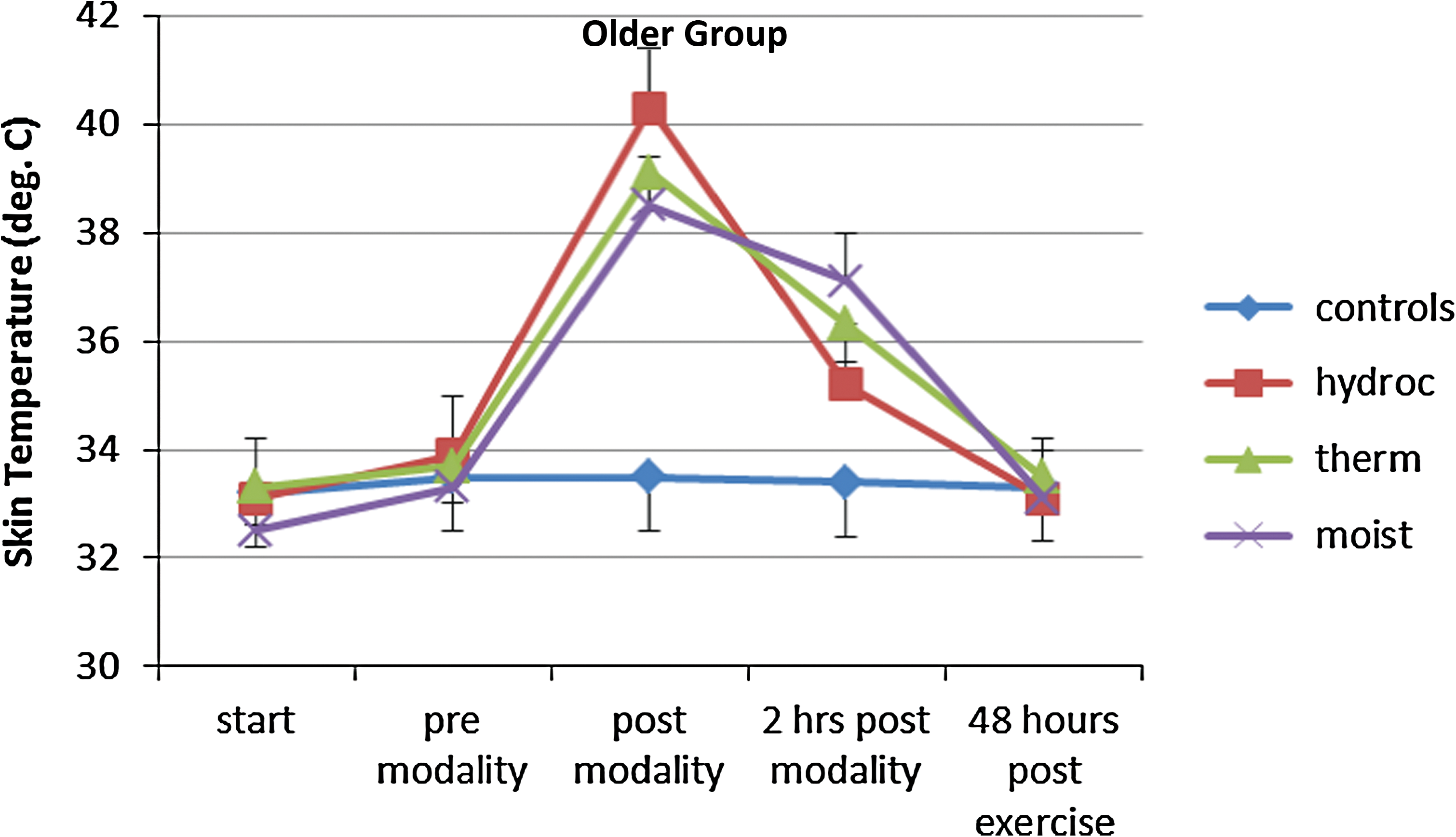
Skin temperature in the older group of subjects measured with a thermal camera for 10 control subjects (diamonds), 10 subjects who used hydrocollator heat wraps (squares), 10 subjects who used ThermaCare heat wraps (triangles), and 10 subjects who used moist heat wraps (×) before exercise (start), 24 h after exercise and before the modality was applied (pre modality), after the modality was applied (post modality), 2 h after the modality was applied, and 48 h after the exercise measured at four locations on the abdominal area. Data are mean ± SD values. Color images available online at
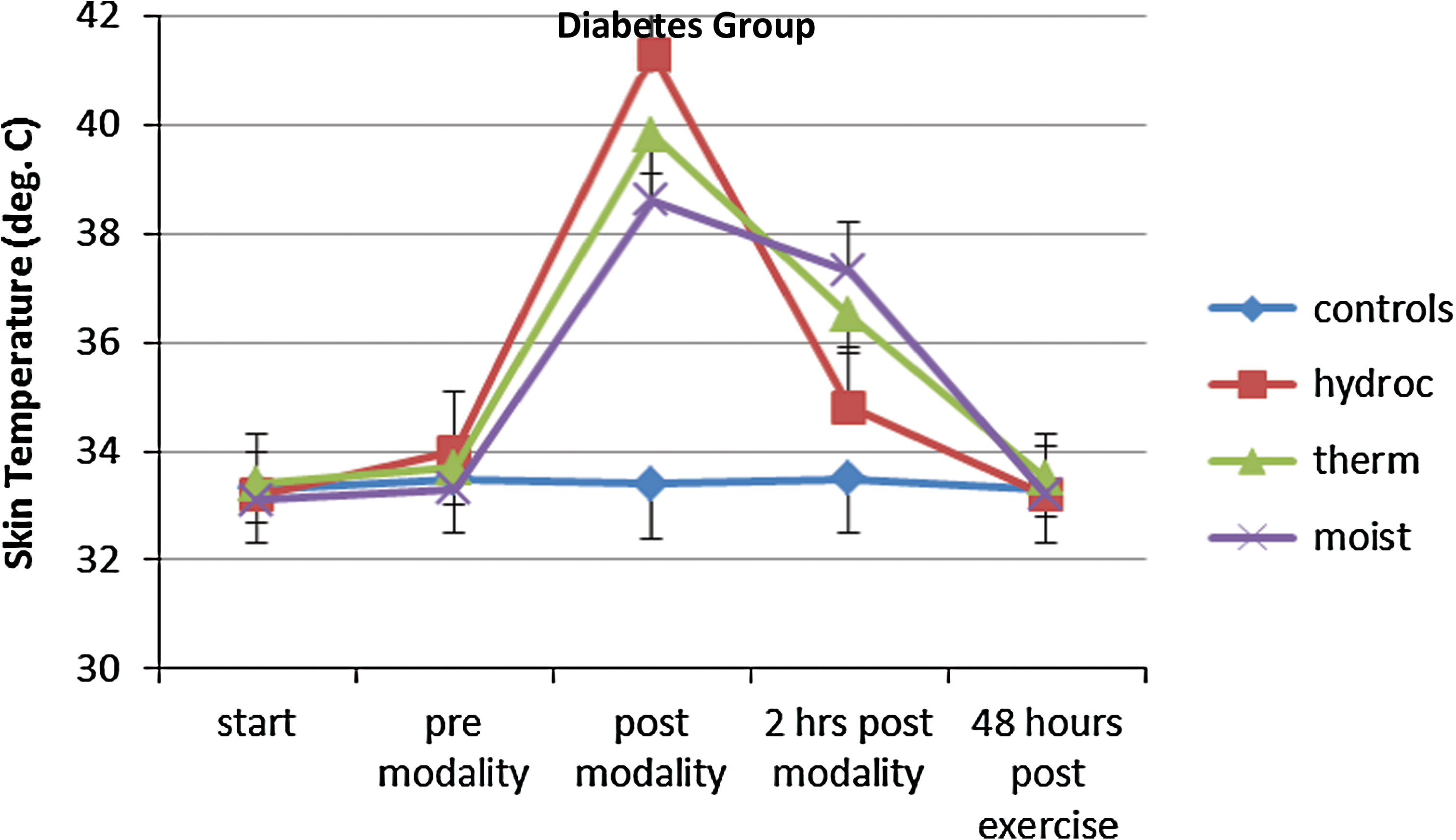
Skin temperature in the diabetes group of subjects measured with a thermal camera for 10 control subjects (diamonds), 10 subjects who used hydrocollator heat wraps (squares), 10 subjects who used ThermaCare heat wraps (triangles), and 10 subjects who used moist heat wraps (×) before exercise (start), 24 h after exercise and before the modality was applied (pre modality), after the modality was applied (post modality), 2 h after the modality was applied, and 48 h after the exercise measured at four locations on the abdominal area. Data are mean ± SD values. Color images available online at
As shown in Figure 2 for the older group, skin temperatures were, on the average, greater 24 h after the exercise, increasing by 0.57 ± 1.8°C more; this increase was significant (P < 0.01). The skin temperature at rest before the exercise averaged significantly higher by 0.5°C in the older than the younger cohort. Skin temperature did not change significantly after the next 2-h period in the control group, but in the hydrocollator group it increased by 6.4 ± 1.3°C after the modality was removed. Skin temperature was significantly less in the ThermaCare and moist heat groups. For all three heat groups, the temperature increase in the older cohort was significantly greater than in the younger cohort (P < 0.05, ANOVA). Two hours after the modalities were applied (as shown in Fig. 2), the greatest skin temperature was in the moist heat group, for which temperatures were still 3.8 ± 1.1°C higher than the pre-modality data. By 2 days, skin temperatures were almost back to the starting temperatures for all groups.
The same general pattern was seen for the subjects with diabetes as was seen for the older group. As shown in Figure 3, for the group with diabetes, skin temperature was averaging 0.37 ± 0.5°C higher 24 h after the exercise; this increase was significant (P < 0.01). Skin temperature did not change significantly after the next 2-h period for the control (no modality) group, but for the hydrocollator group the temperature right after the modality was removed increased by 7.3 ± 3.1°C; the increase was significantly less in the ThermaCare and moist heat groups (P < 0.05). Also, the temperature increase instantly after the modality was significantly higher than was seen in the older and the younger groups (P < 0.05). As seen in Figure 3, the greatest skin temperature was in the moist heat group 2 h after the modalities were applied, in which temperatures stayed 4.0 ± 1.4°C higher than the pre-modality data. The group with diabetes had a greater skin temperature with moist heat 2 h after the modality was applied than the older and younger groups (P < 0.05). By 2 days, skin temperatures were almost back to the starting temperatures for all groups.
Blood flow
The results of the measurements of blood flow are shown in Figures 4 –6. Figure 4 illustrates the blood flow in the younger cohort of subjects. For the younger control group, the average blood flow was 81.3 ± 9.2 flux before the exercise and did not change significantly throughout the 2-day period as shown in Figure 4. The greatest increase in skin blood flow was in the moist heat group, in which the blood flow from before to after the modality increased by 503.1 ± 83.2 flux. Blood flow remained elevated 2 h after the modality started but was back to normal by 48 hours post-exercise. Blood flow was nearly as high with the hydrocollator heat packs but was significantly elevated above rest for the ThermaCare product. The differences in peak blood flow immediately after the modality was significantly different among the three groups of subjects (ANOVA, P < 0.05). The skin blood flows 2 h post-modality were not significantly different between the hydrocollator and control groups, whereas the ThermaCare group still had elevated blood flow above the pre-modality skin blood flows for that group.
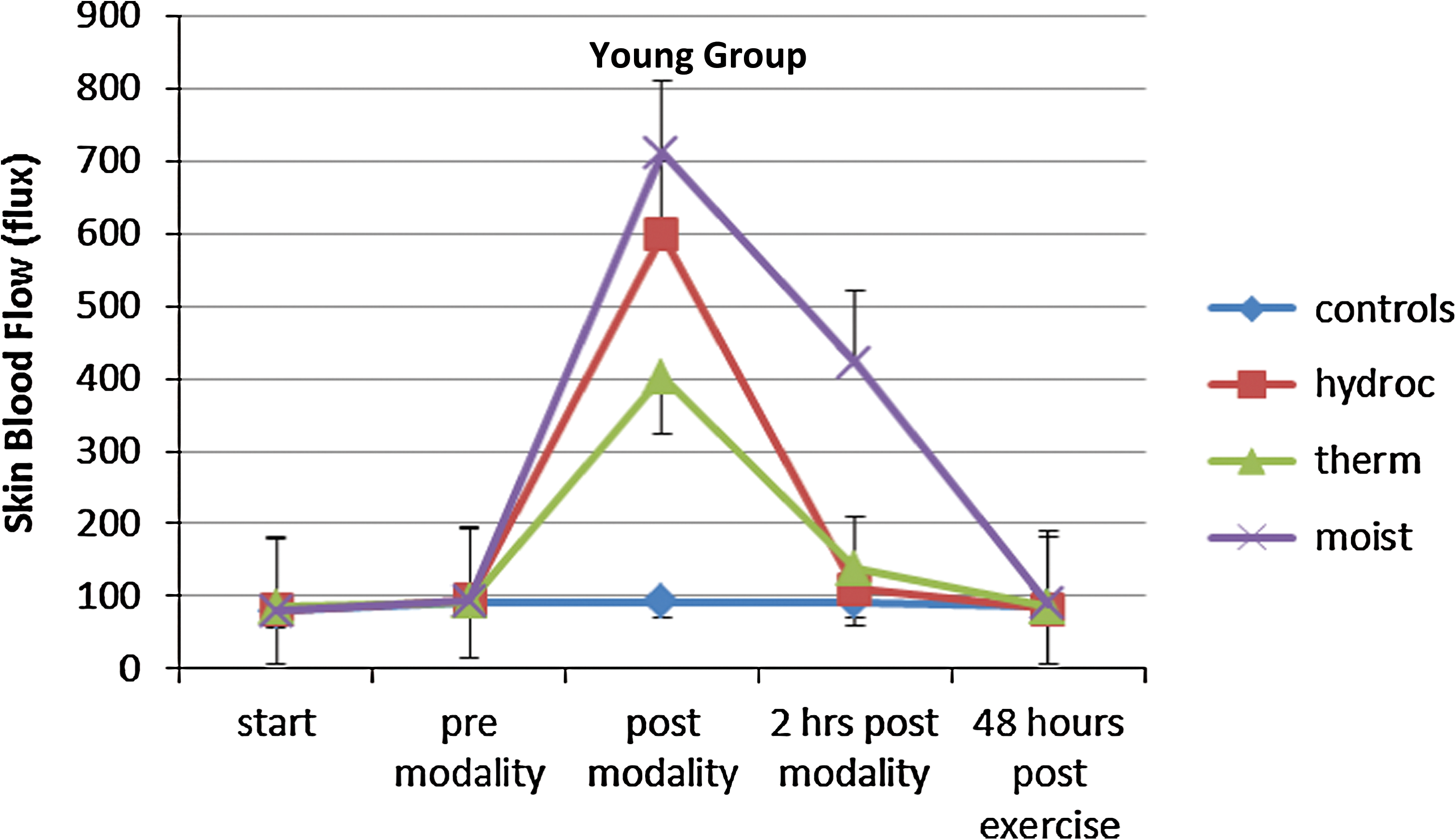
Skin blood flow in the younger group of subjects measured with a laser Doppler flow meter for 10 control subjects (diamonds), 10 subjects who used hydrocollator heat wraps (squares), 10 subjects who used ThermaCare heat wraps (triangles), and 10 subjects who used moist heat wraps (×) before exercise (start), 24 h after exercise and before the modality was applied (pre modality), after the modality was applied (post modality), 2 h after the modality was applied, and 48 h after the exercise measured at four locations on the abdominal area. Data are mean ± SD values. Color images available online at

Skin blood flow in the older group of subjects measured with a laser Doppler flow meter for 10 control subjects (diamonds), 10 subjects who used hydrocollator heat wraps (squares), 10 subjects who used ThermaCare heat wraps (triangles), and 10 subjects who used moist heat wraps (×) before exercise (start), 24 h after exercise and before the modality was applied (pre modality), after the modality was applied (post modality), 2 h after the modality was applied, and 48 h after the exercise measured at four locations on the abdominal area. Data are mean ± SD values. Color images available online at
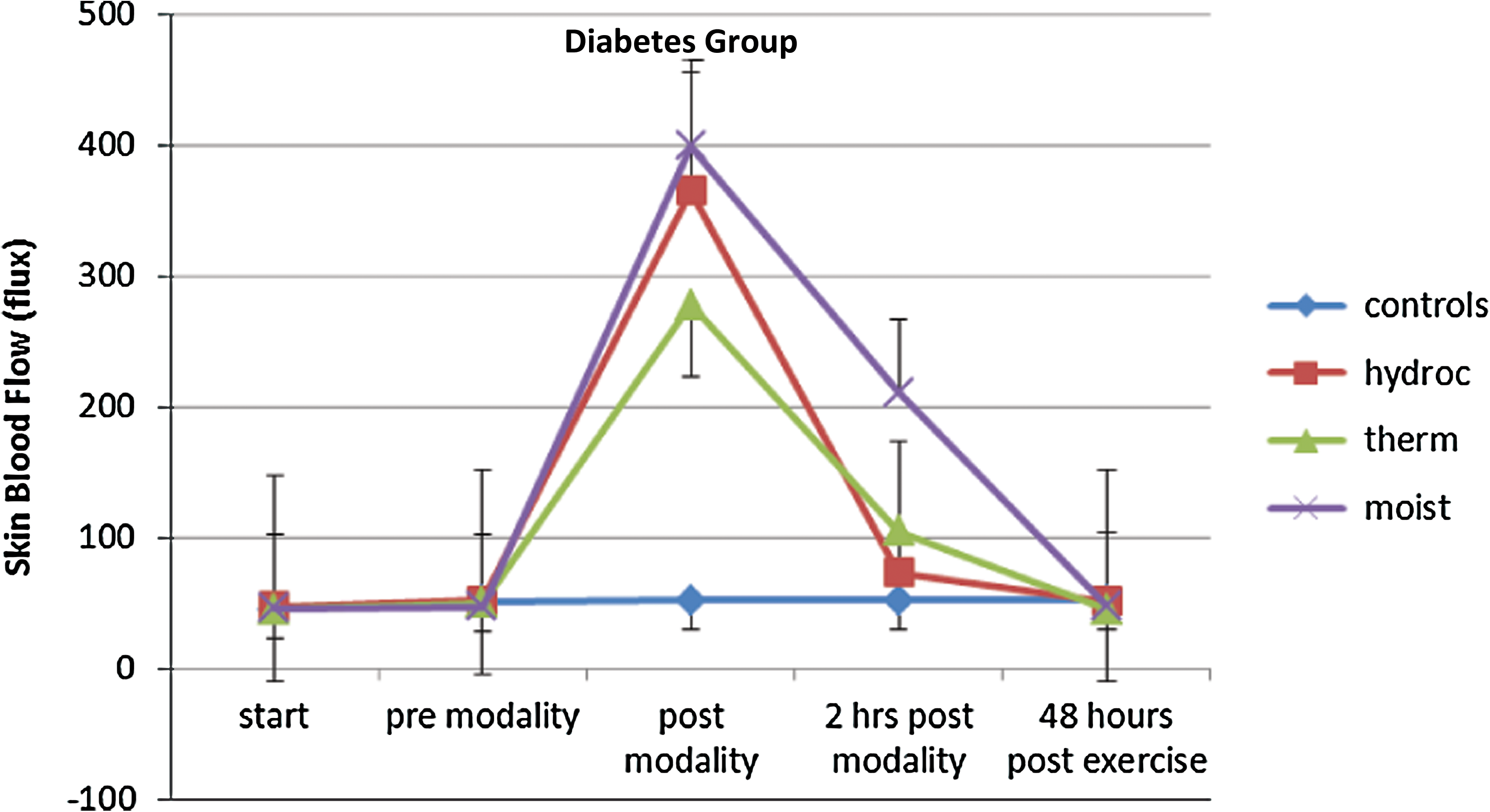
Skin blood flow in the diabetes group of subjects measured with a laser Doppler flow meter for 10 control subjects (diamonds), 10 subjects who used hydrocollator heat wraps (squares), 10 subjects who used ThermaCare heat wraps (triangles), and 10 subjects who used moist heat wraps (×) before exercise (start), 24 h after exercise and before the modality was applied (pre modality), after the modality was applied (post modality), 2 h after the modality was applied, and 48 h after the exercise measured at four locations on the abdominal area. Data are mean ± SD values. Color images available online at
Figure 5 illustrates the blood flow in the older cohort of subjects. For the older control group, the average blood flow was 59.5 ± 15.2 flux before the exercise and did not change significantly throughout the 2-day period (as shown in Fig. 5). The resting blood flow was significantly less than in the younger groups of subjects (P < 0.01). The pattern of response, although less at each examination point in Figure 5, was similar to that of the younger subjects shown in Figure 4. Here, the greatest increase in skin blood flow was for the group using moist heat, in which the blood flow from before to after the modality increased by 423 ± 79.5 flux. Blood flow remained elevated 2 h after the modality started but was back to normal by 48 h post-exercise. Blood flow was nearly as high with the hydrocollator heat packs but s8ignificantly elevated above the resting value for the ThermaCare product. The differences in peak blood flow immediately after the modality were significantly different among the three groups of subjects (ANOVA, P < 0.05). The skin blood flow 2 h post-modality was not significantly different between the hydrocollator and control groups, whereas the ThermaCare group still had elevated blood flow above the pre-modality skin blood flows for that group.
Figure 6 illustrates the blood flow in the cohort of diabetes subjects. For the diabetes group, the average blood flow was 45.7 ± 11.8 flux before the exercise and did not change significantly throughout the 2-day period as shown in Figure 6. The resting blood flow was significantly less than in the younger or older group of control subjects (ANOVA, P < 0.01). The pattern of response, although less at each examination point in Figure 6, was similar to that for the younger subjects shown in Figure 4 and the older subjects shown in Figure 5. Here, the greatest increase in skin blood flow was for the group using moist heat, in which the blood flow from before to after the modality increased by 352 ± 38.7 flux. Blood flow remained elevated 2 h after the modality started but was back to normal 48 h post-exercise. Blood flow was nearly as high with the hydrocollator heat packs but significantly elevated above the resting value for the ThermaCare product (P < 0.01). The differences in peak blood flow immediately after the modality were significantly different among the three groups of subjects (ANOVA, P < 0.05). The skin blood flow 2 h post-modality was not significantly different between the hydrocollator and control groups, whereas the ThermaCare group still had elevated blood flow above the pre-modality skin blood flows for that group.
Muscle soreness
The results of the muscle soreness VAS are shown in Figures 7 –9 for the younger, older, and diabetes cohorts, respectively. The younger and older groups had no soreness or discomfort prior to the exercise, whereas the diabetes group (Fig. 9) showed some soreness before the study started. The 10-cm scale in Figures 7 –9 is converted to and shown in millimeters on the ordinate. The average soreness for the diabetes cohort was significantly higher after the exercise than was the case for the older and younger groups (ANOVA, P < 0.01). The average for the diabetes group was 73.3 ± 16.2, for the older group was 56.1 ± 15.1, and for the younger group was 41.5 ± 9.3; these differences were significant (ANOVA, P < 0.05) as shown in Figures 7 –9. For all three groups of subjects, the greatest reduction in soreness after the modality was moist heat both immediately after the modality and up to 2 days post-exercise. The greatest reduction in pain was in the older subjects. For this group, after the modality, moist heat reduced pain by 52.3%, compared with 30.5% in the subjects with diabetes and 33.3% in the younger subjects. ThermaCare reduced pain by 32.2% in the older subjects, 19.1% in the subjects with diabetes, and 25.1% in the younger subjects. The hydrocollator was almost as effective as moist heat, but the effect was not maintained even 2 h after the modality.

The soreness scale in the younger group of subjects for 10 control subjects (diamonds), 10 subjects who used hydrocollator heat wraps (squares), 10 subjects who used ThermaCare heat wraps (triangles), and 10 subjects who used moist heat wraps (×) before exercise (start), 24 h after exercise and before the modality was applied (pre modality), after the modality was applied (post), 2 h after the modality was applied, and 48 h after the exercise measured at four locations on the abdominal area. Data are mean ± SD values. VAS, visual analog scale. Color images available online at
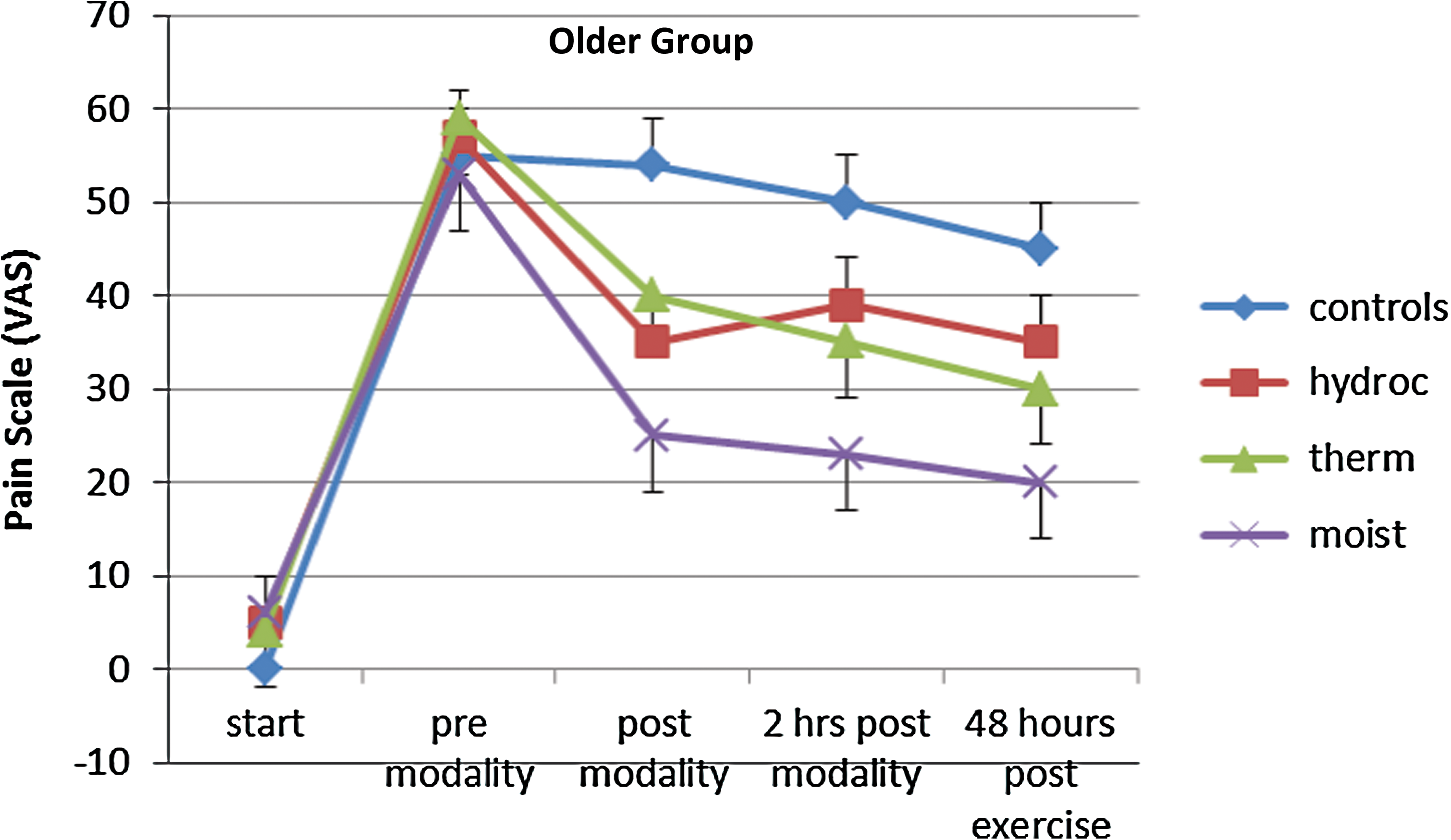
The soreness scale in the older group of subjects for 10 control subjects (diamonds), 10 subjects who used hydrocollator heat wraps (squares), 10 subjects who used ThermaCare heat wraps (triangle) and 10 subjects who used moist heat wraps (×) before exercise (start), 24 h after exercise and before the modality was applied (pre modality), after the modality was applied (post modality), 2 h after the modality was applied, and 48 h after the exercise measured at four locations on the abdominal area. Data are mean ± SD values. VAS, visual analog scale. Color images available online at
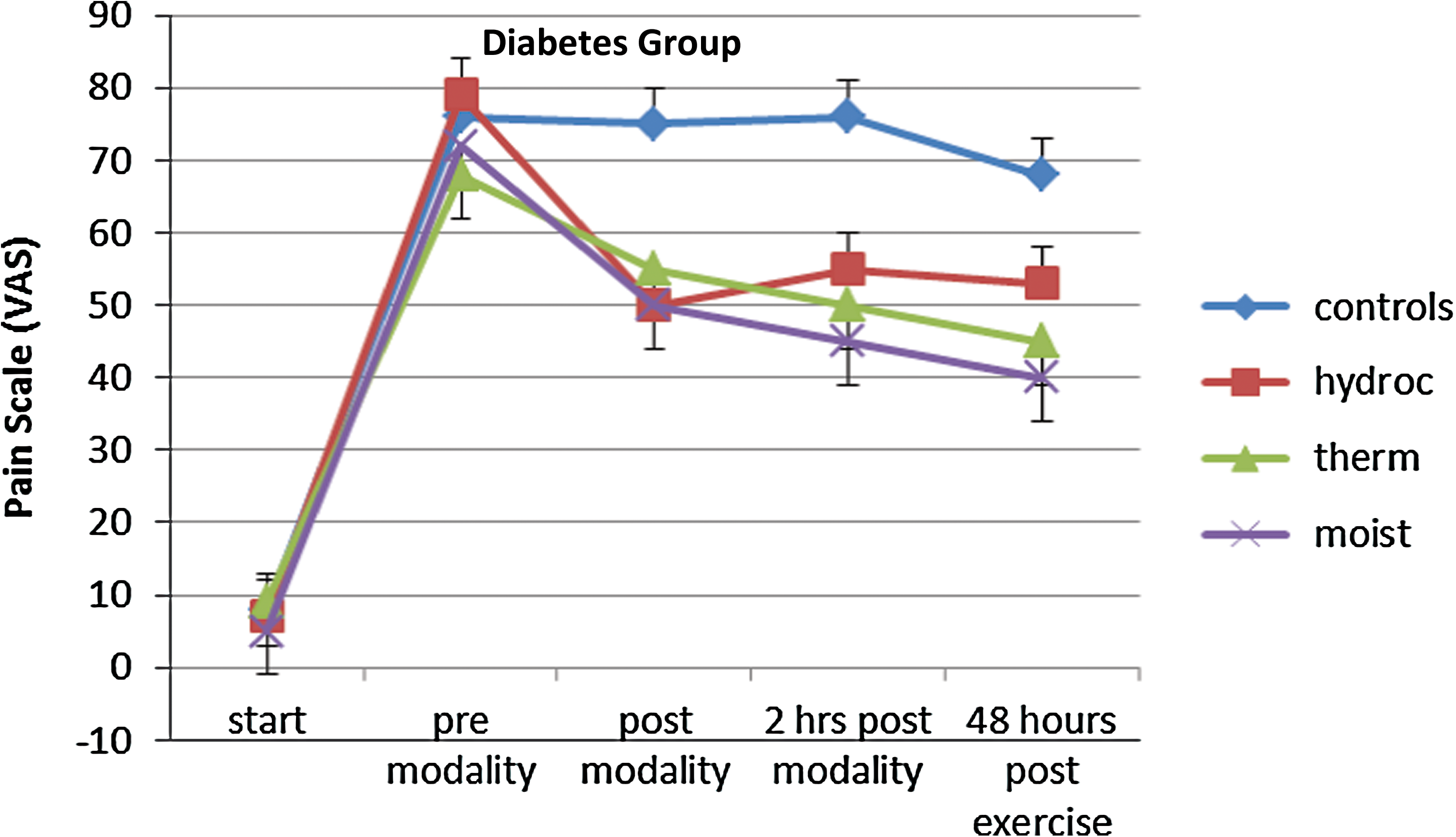
The soreness scale in the diabetes group of subjects for 10 control subjects (diamonds), 10 subjects who used hydrocollator heat wraps (squares), 10 subjects who used ThermaCare heat wraps (triangles), and 10 subjects who used moist heat wraps (×) before exercise (start), 24 h after exercise and before the modality was applied (pre modality), after the modality was applied (post modality), 2 h after the modality was applied, and 48 h after the exercise measured at four locations on the abdominal area. Data are mean ± SD values. VAS, visual analog scale. Color images available online at
Perception of warmth after the modality
As each of the modalities ended, the VAS scale for perception of warmth showed that, in the younger subjects, the perception of dry heat was 49.5 ± 8.2, of moist heat was 63.2 ± 11.1, and for the hydrocollator packs was 60.1 ± 8.2. There was no statistical difference between moist and hydrocollator heat, but both were significantly higher than ThermaCare.
Discussion
Diabetes causes whole-body inflammation 18 that results in increased nerve sensitivity, nerve death, 40 myopathies, and endothelial cell dysfunction. 16,17 Because of these factors and of the metabolic impairments associated with diabetes, exercise performance and training are impaired. 41 However, exercise is still the best means of increasing glycemic control due to reducing blood glucose, thus giving the individual with diabetes a better chance of coping with this disease and preventing its symptoms from getting worse. 42
In the present investigation, subjects participated in an intense exercise program involving a single bout of exercise to identify (1) the extent of muscle soreness and (2) if heat could reduce the soreness in people with diabetes compared with age-matched and younger subjects. Two widespread heat modalities were used: a clinical heat modality, hydrotherapy, 43 and a common home modality, ThermaCare dry heat. 3 –5 However, recent experiments published in the last few years showed that chemically generated moist heat is more effective in warming deep tissue than that seen with either of these standard therapy modalities, 30,36,37 and that is why all three modalities were tested in this study. This is highly relevant because chemical moist heat packs have not been tested on muscle soreness in people with diabetes.
In the present investigation, subjects with diabetes had slight soreness in their muscles to begin with and then realized the greatest increase in soreness 24 and 48 h after the exercise compared with the other two groups. This was a vigorous exercise routine, and although the diabetes cohort certainly did not exercise as hard as the young group, they had almost twice as much DOMS. Pain in the arms, hips, and back is common in diabetes. 44 Lower leg pain is common in diabetes during exercise even without symptoms of vascular disease. 45,46 In some cases it is due to intermittent claudication. 46 However, it can be due to distal diabetic neuropathy with impaired cutaneous and vibration sensitivity, which is also common. 46 –48 Joint pain is also common when accomplishing exercise in people with diabetes. 49 Pain is usually worse after exercise as was seen in the present investigation. 48
To try and reduce pain clinically, hydrocollator heat packs are often used. This involves high temperatures being applied for a short period of time. 43 Heat activates transient receptor potential vanillin-4 and -1 voltage-gated calcium channels in the skin, inhibiting P2X2 purine pain receptors on tactile nerves. 16,30,38,50 However, because of the high temperatures and the brief duration of use of this type of hot pack, there is a risk of burns. Hydrocollator heat packs also have little effect on muscle temperature but do elicit an increase in skin blood flow (as seen here). 36,51 So even though pain relief is present when using these hot packs, it is rapidly lost, as is the increase in blood flow.
ThermaCare dry heat provides a safer level of continuous heat at a lower temperature, so these kind of heat packs can be left on for longer periods of time (up to 8 h), without skin burns, thus warming the skin and muscle to provide pain relief. 4,5,36 In the present investigation it provided an increase in skin circulation that was sustained after the heat wrap was removed. It also provided more sustained pain relief than that seen for hydrocollator heat wraps in all three groups of subjects.
However, previous studies have shown better heat penetration and greater blood flow with moist heat compared with the other two modalities. Dry heat limits the skin blood flow response to heat because of osmoreceptors in the skin reducing the blood flow response to heat when heat is dry. Combining heat with moisture increases the blood flow response to heat and allows faster heat penetration into deep tissue. 16,36,37 Therefore, in this study, skin blood flow was greater, whereas skin temperatures were lower, with moist heat compared with dry heat. Pain relief following the moist heat modality was much better than the other two modalities in all the three cohorts. Because people with diabetes are more susceptible to burns and skin damage, 5,36,51 moist heat seems to be a better form of heating than the other two modalities when the intention is to relieve pain that results from muscle soreness.
Footnotes
Author Disclosure Statement
No competing financial interests exist.