
Abstract
Background:
Diabetic foot ulcers are associated with significant morbidity. Conventional treatment modalities are often of limited success in promoting complete wound closure. The aim of the present study was to examine the efficacy of noninvasive ozone–oxygen therapy in the treatment of diabetic foot ulcers.
Methods:
Diabetes patients with a Wagner classification stage 2 or 3 ulcer or a stage 4 ulcer after debridement of at least 8 weeks in duration were included in this double-blind, randomized, placebo-controlled clinical trial. Patients received conventional treatment in combination with either ozone–oxygen treatment or sham treatments for 12 weeks, and after an additional 12 weeks, wound status was re-examined.
Results:
In total, 61 patients (62% male, 62.6±9.8 years old) participated in the study; 32 were randomized to ozone treatment, and 29 to placebo. The proportion of subjects with full wound closure did not differ significantly by treatment assignment (41% vs. 33%, P=0.34). Among the 34 subjects who completed the study per protocol (PP) (16 in the ozone group, 18 in the placebo group), a significantly higher rate of complete wound closure was observed in the ozone group (81% vs. 44%, P=0.03). Among PP patients with wound size ≤5 cm2, the rate of total wound closure was 100% versus 50% in the sham treatment group (P=0.006). A nonsignificant, 55.5% relative increase in healed wound area was detected in the ozone group versus the placebo group (4.2±4.9 cm2 vs. 2.7±1.5 cm2, P=0.23).
Conclusions:
Among PP patients, ozone treatment in addition to conventional treatment was superior to conventional treatment alone in promoting the complete healing of diabetic foot ulcers.
Introduction
Diabetic foot ulcers result from both neuropathy and angiopathy. The neuropathy leads to loss of sensation and foot deformity, which predisposes the foot to increased localized pressure, callus formation, and eventual tissue breakdown and ulcer formation. Micro- and macrovascular changes lead to decreased perfusion, interfering with satisfactory wound healing. Poor metabolic control further delays healing. Wounds in diabetes commonly become infected with Gram-positive organisms, such as Staphylococcus aureus, and infection with other microorganisms, including Gram-negative bacteria and anaerobes, is also observed. 3 Wound infection threatens the integrity of the foot and may ultimately lead to amputation, particularly in limbs with poor perfusion.
Foot ulcers in people with diabetes are associated with prolonged healing time, wound infection, and repeated hospitalizations, all posing a burden on the healthcare system. It has been estimated that the cost of treating a diabetes patient with a leg wound is 5.4 times greater than the cost of treating a diabetes patient without such a wound, 4 with hospitalization accounting for approximately 80% of the cost of care. 5
Conservative treatment for diabetic foot ulcers is based on off-loading the affected foot, debridement of the wound, wound dressing, treatment of infection, and revascularization of the limb when indicated, as well as optimization of metabolic control. 6 Conservative treatment is successful in the majority of severely infected wounds, but the duration of treatment is often prolonged. 7,8
Recent technologies evaluated to promote the healing and closure of diabetic foot wounds include the vacuum-assisted closure system, which appears to have good results with surgical wound closure; 9,10 however, it appears to be less effective in treating diabetic foot ulcers. 11 Hyperbaric oxygen has been demonstrated to be effective in the treatment of foot ulcers in those with and without diabetes, 12,13 although results in diabetes patients are more controversial. 14 Ozone has been used to treat leg ulcers for many decades, 15 but its efficacy in treating foot wounds in diabetes has not been thoroughly evaluated. The purpose of the present study was to evaluate the efficacy of noninvasive ozone–oxygen therapy in the treatment of foot wounds in diabetes.
Subjects and Methods
This randomized, placebo-controlled, multicenter clinical trial was approved by each institution's Helsinki Committee as well as by the Israel Ministry of Health. All patients gave signed informed consent prior to participating in the study.
Study participants
Patients were recruited from two large diabetes clinics in Israel: E. Wolfson Medical Center, Holon; and Soroka University Medical Center, Beer-Sheva. Included in the study were adult (18 years of age and older) men and women with type 1 and type 2 diabetes and a Wagner classification stage 2 or 3 or post-debridement stage 4 foot ulcer. The wound size was ≤40 cm2, and the wound was at least 8 weeks old at study initiation.
Patients were excluded from the study if they had one or more of the following conditions: (1) gangrenous foot ulcers, (2) active osteomyelitis, (3) a history of collagen diseases, (4) hyperthyroidism, (5) pregnancy or nursing, (6) hemoglobin A1c (HbA1c) levels >10.5%, (7) ankle brachial index (ABI) <0.65, (8) hemoglobin less than 8 g/dL, (9) liver function tests (alanine transaminase, aspartate transaminase, or γ-glutamyl transpeptidase) elevated to more than three times the upper normal limit, (10) serum creatinine >2.5 mg/dL or dialysis, and (11) a known allergy to ozone.
Design
The study was a randomized, double- blind, placebo-controlled clinical trial. Included patients were randomized to one of two treatment groups. The ozone (active treatment) group received ozone treatments using the Ozoter 101® device (OZ Recovery Technologies, Ramat Gan, Israel) in addition to usual diabetic foot ulcer care. The control group received sham treatments using the Ozoter 101 device set to the inactive mode in addition to usual diabetic foot ulcer care.
Study visits were performed at baseline and at weeks 1, 2, 3, 4, 6, 8, 10, and 12. At week 24, 12 weeks after the completion of the active study treatment, a termination visit was performed, and patients were examined for wound status. Complications of treatment were monitored at each visit.
Treatment plan
Usual care included debridement and daily wound dressings appropriate for the degree of secretion and moisture maintenance of the wound. Active ozone treatment was divided into two phases: at first, patients received treatment sessions four times each week for the maximum period of 4 weeks, or until granulation appeared in 50% of the wound area, whichever came first. Intervals between treatments did not exceed 1 day in 5 days a week, and gas concentrations were 96% oxygen and 4% (80 μg/mL) ozone. During the second treatment period, session frequency was reduced to twice a week to complete the 12 weeks of treatment, and gas concentration was changed to 98% oxygen and 2% (40 μg/mL) ozone. Patients in the control group received sham treatments, and the ozone device circulated room air only. Each treatment session lasted 26 min.
A study technician was trained to operate the Ozoter 101 device and performed the actual treatments. The technician determined the mode of action for each patient according to the randomization, so that 32 patients were treated in the active model (ozone–oxygen treatment), and 29 in the inactive mode (room air only). The patients and the investigator were blinded to the mode of treatment.
Ozoter 101 device
A complete description of the device is reported elsewhere (

The Ozoter 101 device. Color images available online at
Once an air-tight seal is established, the second step begins, in which the ozone/oxygen mixture is introduced into the system. For the first 6 min, ozone levels are increased by the system from 0% to 4% (from 0 to 80 μg/mL) and to 96% oxygen according to the phase of the study treatment. During the next 14 min, ozone levels are maintained at the determined concentration in the −40 mbar subatmospheric condition. The duration of each session is 26 min, including a 20-min ozone treatment session, after which pure 100% oxygen is passed through the system for an additional 6 min, to assure complete removal of ozone from the system. Throughout the session, the ozone is returned through the tubing to an ozone destruction device. The gases are streamed from the ozone generator to the chamber and then to the ozone killer that turns the ozone to oxygen.
Study visits
During the baseline visit, demographic and medical information including age, sex, medical history, laboratory values, and wound assessments were gathered from patient interview and from the patient's medical record. Physical examination was performed at baseline, and ABI was assessed using a sphygmomanometer. Laboratory measures included a complete blood count, sedimentation rate, complete blood chemistry including liver function tests, HbA1c, and urinalysis.
Wound assessment included wound size measurements and assessment for wound infection. The wound surface area was measured by applying a transparent grid onto the wound, according to the method described by Bohannon and Pfaller 16 and Majeske. 17 In all cases the total recorded surface area, as calculated by the addition of the number of full and half squares, was greater than the actual wound size.
Wound infections were assessed clinically, and the symptoms and signs were recorded. Data recorded included the presence of purulent drainage, erythema, color, exudation, odor, pain, fever, and leukocytosis. A post-debridement swab culture specimen was also used to determine the presence of infection and to guide appropriate antimicrobial therapy. Bacterial cultures were taken on the first day of treatment and then every fourth treatment and at week 24 of the study.
Study definitions and end points
Intention to treat cohort
The flow diagram of study participants is presented in Figure 2. The intention to treat (ITT) cohort comprised all patients randomized to this study who were examined at the baseline visit and had full baseline data including wound size at study entry. Patients who did not complete follow-up had end point data imputed using last observation carried forward.
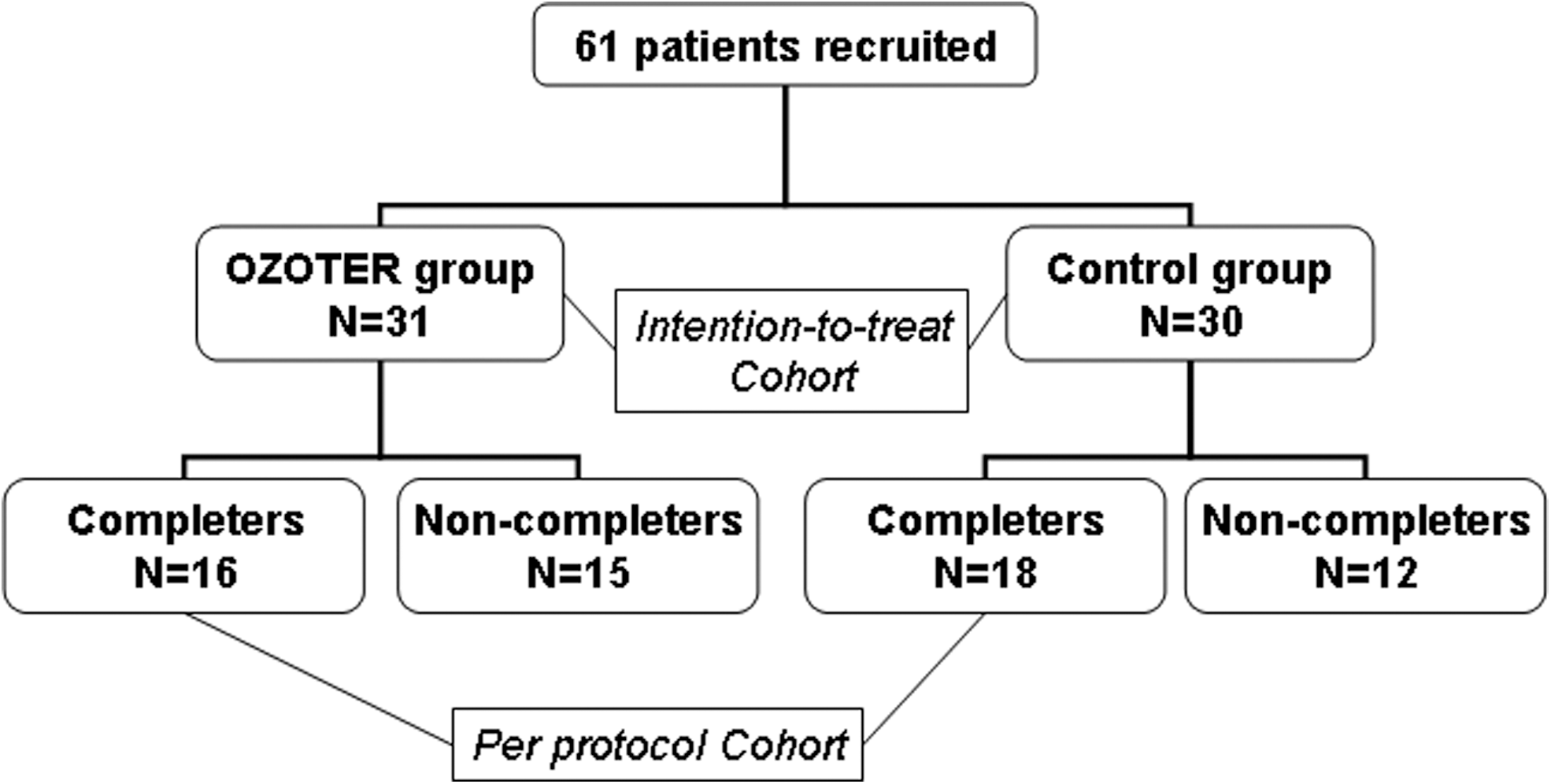
Consort diagram of study flow.
Per protocol cohort
The per protocol (PP) cohort comprised ITT cohort patients who attended the final visit, had a reported measurement of the wound size at study termination, and had at least one additional wound measurement during the 12 weeks of the study.
Non-compliance
Non-compliance was defined as missing more than one treatment session for any reason. Per definition, patients who missed two or more treatment sessions were considered non-compliant and discontinued from study participation. Discontinuation from study participation could also be necessitated on the basis of patient welfare. Subjects who prematurely terminated study participation were evaluated as part of the ITT analysis. For these patients, the last available wound size measurement was used (last observation carried forward).
Primary end point
The primary end point was an ITT by-treatment group comparison of the proportion of subjects with complete closure of the wound.
Secondary end points
Secondary end points included (1) wound size and (2) the proportion of patients who had a reduction in wound size. In addition, primary and secondary end points were secondarily analyzed in the subgroup of patients who completed the treatment PP (PP cohort).
Adverse events
Deterioration of the target ulcer (manifested as new-onset erythema, pain, purulent discharge, infection, tissue necrosis, requirement for repeated debridement, or other surgical intervention such as amputation) was considered a serious adverse event, and the patient was considered a “non-responder” even if the ulcer was completely closed prior to the final visit.
Total area closed
The “total area closed” was calculated for each patient by subtracting the last available wound size measurement from the first one. The timing of the last available measurement for the ITT cohort varied from week 2 to week 24. For the PP group, the last available measurement was the one obtained at week 24 or was set to 0 in the case of an early wound closure. The first wound size was, in most cases, the baseline size measurement, except for four patients (one in the control group, three in the ozone group) for whom the Week 1 measurement was used because of lack of data for the baseline visit.
Statistical analysis
Data were analyzed using SAS software version 8 (SAS Institute, Cary, NC). The t test for independent samples or the Mann–Whitney U test were used as appropriate for a given variable's distribution to compare continuous data by treatment group. The χ2 or Fisher's exact test was used to examine by treatment differences in categorical variables. Missing data were imputed using last observation carried forward. All tests were two-sided and considered significant at P<0.05.
Results
Patient dispensation
As indicated in Figure 2, 61 patients with diabetes were randomized to treatment: 32 to the active ozone treatment and 29 to the sham treatment. All patients randomized to treatment are included in the ITT cohort. A total of 34 patients completed the study PP: 16 in the ozone group and 18 in the sham treatment group. Patients are compared by completion status in Table 1. As can be seen, patients who completed and those who dropped out were similar in terms of age, sex, duration of diabetes, HbA1c at baseline and end point, and baseline wound size. There were somewhat more patients with ABI >1 among completers than among those who discontinued the study.
ABI, ankle brachial index; HbA1c, hemoglobin A1c.
Table 2 lists the reasons for discontinuing the study among patients in the ITT cohort. There were two adverse events or complications in the control group versus five events in the ozone group. Adverse events/complications in the control group included amputation and infection, and in the ozone group they included osteomyelitis, fever, wound infection, and pulmonary congestion. None of the adverse events was assessed to be causally associated with the study intervention.
Characteristics of the 61-subject ITT cohort are described in Table 3.
ABI, ankle brachial index.
Primary end point
A significant between-group difference in the proportion of patients with full wound closure was not detected (41% vs. 33%, P=0.34).
Secondary end points
Secondary end points included (1) wound size and (2) the proportion of patients who had a reduction in wound size. As shown in Table 4, total area closed did not differ between treatment groups in either the ITT or PP cohorts.
ITT, intention to treat cohort (n=61, 32 in the ozone group and 29 in the control group); PP, per protocol cohort (16 in the ozone group and 18 in the control group).
Of 34 (56%) patients who were included in the PP cohort, the 16-patient ozone study group had a significantly greater proportion of complete wound closure than controls (81% vs. 44%, P=0.03). When this comparison was repeated in the subgroup of patients with baseline wound size ≤5 cm2, 100% of ozone-treated patients versus 50% of control patients exhibited complete wound closure (P=0.006).
Discussion
In the present study, the between-group difference in the proportion of patients with full wound closure was not significant in the ITT analysis. In the PP analysis, the ozone treatment group had a significant, relative increase in the proportion of patients with full wound closure (81% vs. 44%, P=0.03). When the analysis was performed in the subgroup of patients with small initial ulcer size (≤5 cm2), ozone treatment doubled the proportion of patients with full wound closure. In the PP cohort, ozone therapy conferred a significant treatment benefit over conventional treatment alone.
Historically, the medical use of ozone can be traced to the 19th century, with the first ozone generators developed by Werner von Siemens in Germany in 1857. The first therapeutic ozone applications were initiated around 1870. During World War 1, ozone was used to treat wounds, trench foot, and gangrene decubitus ulcers (
In the present study, none of the wounds larger than 5 cm2 at baseline had closed by the end of follow-up. It appears that 12 weeks of treatment is not sufficient to close larger wounds. Between-group differences in total area closed were not observed; nevertheless, total area closed was consistently greater in the ozone group, suggesting that the sample size was inadequate to detect true differences in this secondary end point.
Generalization of our study results is greatly limited by the large attrition rate, which suggests selection bias. Although significant differences in characteristics between patients who discontinued study participation and those who completed it were not detected, it is nevertheless possible that study completers are different in some meaningful, if unmeasured, way from those who dropped out. The study protocol necessitated frequent visits to the treatment centers, an effort likely difficult for relatively elderly, immobile individuals. Moreover, travel to and from the hospital was not compensated, and this too may have influenced attrition rates. Therefore, the significant findings in the PP cohort must be interpreted in the framework of possible selection bias because all PP analyses inherently violate randomization. Nevertheless, measures of healing were consistently higher and clinically meaningful in the ozone group, in all analyses. Armed with better understanding of the behavior of diabetic foot ulcers exposed to ozone gained from the present study, another clinical trial, adequately powered to detect these end points, could be performed.
Despite the aforementioned study limitations, it is reasonable to conclude that ozone–oxygen treatments confer clinically meaningful benefit in the treatment of diabetic foot ulcers when added to conventional treatment, especially when adminstered PP and for foot ulcers with a surface area <5 cm2.
Footnotes
Acknowledgments
The Ozoter 101 device was provided by OZ Recovery Technologies, Ramat Gan, Israel.
Author Disclosure Statement
No competing financial interests exist.