
Abstract
Background:
This study was performed to examine the efficacy of sitagliptin, a dipeptidyl peptidase-4 inhibitor, in Japanese patients with type 2 diabetes using continuous glucose monitoring (CGM) of 24-h glycemic changes.
Subjects and Methods:
The study was a prospective open-label pilot study in patients with type 2 diabetes who were admitted to our hospital and treated with sitagliptin alone or concomitantly with another oral hypoglycemic drug. CGM was performed for 2 days before sitagliptin administration and for another 2 days after administration. The average 24-h blood glucose level, SD of the 24-h blood glucose level, 24-h glycemic fluctuation range, mean amplitude of glycemic excursions (MAGE), and hyperglycemic and hypoglycemic time periods were compared before and after administration.
Results:
Sitagliptin administration alone and with a concomitant drug decreased the average 24-h blood glucose level, SD of the 24-h blood glucose level, 24-h glycemic fluctuation range, MAGE, and hyperglycemic time, compared with these parameters before administration. There were significant correlations between the average 24-h blood glucose level before administration and the decrease in the average 24-h blood glucose level after administration and between MAGE before administration and the decrease in MAGE after administration.
Conclusions:
Sitagliptin decreased the average glycemic level and also improved 24-h glycemic fluctuation, including postprandial hyperglycemia.
Introduction
In CGM, the average glucose level is measured at an interval of 1–5 min. This allows monitoring of postprandial glycemic changes, which have previously been partially monitored by conventional self-monitoring of blood glucose (SMBG). In CGM, the pattern of glycemic changes can be visualized; the 24-h glycemic fluctuation range (the time for which the glucose level is greater than or less than a certain level) can be obtained; and asymptomatic hypoglycemia, which cannot be determined by conventional methods, can be analyzed using software. These advances have improved glucose management by facilitating control of the glucose level with smaller 24-h glycemic fluctuation and less swing at the same HbA1c value.
Sitagliptin is a dipeptidyl peptidase (DPP)-4 inhibitor that enhances the activity of incretins, which then promote insulin secretion in a glucose-dependent manner, and inhibits glucagon secretion. 4 –7 A comparative clinical study with an α-glucosidase inhibitor showed that sitagliptin significantly improved the glucose level at 2 h after meal, the fasting blood glucose level, and HbA1c. 8 However, each of these parameters was measured at a single time point, and the effects of sitagliptin on 24-h glycemic changes in Japanese patients are still unclear. Therefore, in this study, we examined the effects of sitagliptin on 24-h glycemic changes using CGM in single administration or concomitant administration with another oral hypoglycemic drug.
Subjects and Methods
Study design
This study was performed as a prospective open-label pilot study at two facilities. Approval was obtained from the ethical committee of Shin-yamate Hospital. Prior to commencement of the study, all patients gave informed consent after receiving an explanation of the study. The subjects were patients with type 2 diabetes who were admitted to our hospital for glycemic control. The inclusion criteria were age ≥20 years and ≤75 years old and an HbA1c level at admission ≥6.5% and <10.0% (criteria of the Japanese Diabetes Society). Patients who met the following criteria were excluded: type 1 diabetes (positive for antibody to glutamic acid decarboxylase, C-peptide level in urine 10 μg/day); severe infection in the previous 3 months; and oral administration of a steroid for treatment of rheumatism in the previous 3 months.
Study method
After the patient was admitted to the hospital, CGM was performed when the blood glucose level before a meal reached a stable level after dietary therapy alone or in combination with an oral hypoglycemic drug. CGM was performed using the CGMS® System GOLD™ system (Medtronic MiniMed, Northridge, CA). Glycemic changes were monitored by CGM for 4 successive days, and administration of 50 mg of sitagliptin once daily was started before breakfast on Day 3 of the 4-day observation period (Fig. 1). Based on the CGM data on Day 2 of observation and Day 2 of sitagliptin administration (Day 4 of observation), the average and SD of the 24-hour glucose level, mean amplitude of glycemic excursion (MAGE), 24-h glycemic fluctuation (total area between the 24-h mean blood glucose and continuous blood glucose curve), and time periods of hyperglycemia (glucose level >180 mg/dL) and hypoglycemia (glucose level <70 mg/dL) were determined.
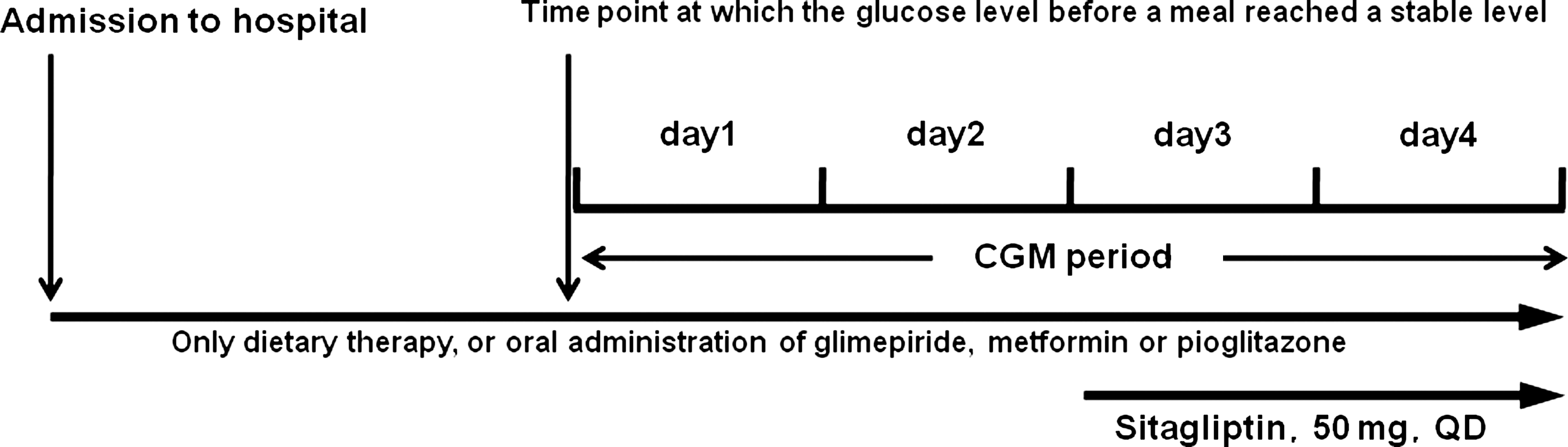
Outline of the study. Continuous glucose monitoring (CGM) was performed when the glucose level before meals reached a stable level after dietary therapy alone or combined dietary therapy and oral administration of a hypoglycemic drug. Glycemic changes were monitored using the Medtronic CGMS System GOLD for 4 successive days. Administration of sitagliptin (50 mg) once daily before breakfast was started on Day 3 of this period.
Statistical analysis
Statistical analysis was performed using SAS version 9.1 software (SAS Institute, Cary, NC). Data obtained on Day 2 and Day 4 of CGM (before and after sitagliptin administration, respectively) were compared by paired t test. Correlations between the average 24-h glucose level before sitagliptin administration and changes in the average 24-h glucose level after administration and those between MAGE before and after administration were evaluated using Pearson correlation analysis.
Results
The patients' background is shown in Table 1. Sitagliptin was administered to 30 subjects (20 men, 10 women) with mean age, body mass index, and HbA1c at hospital admission of 69.9 ± 5.7 years old, 25.3 ± 3.6 kg/m2, and 7.6 ± 1.3% (criteria of the Japanese Diabetes Society), respectively. Fourteen subjects received sitagliptin only, and 16 received concomitant therapy with another oral hypoglycemic drug. A sulfonylurea was the most common concomitant drug.
Criteria of the Japanese Diabetes Society.
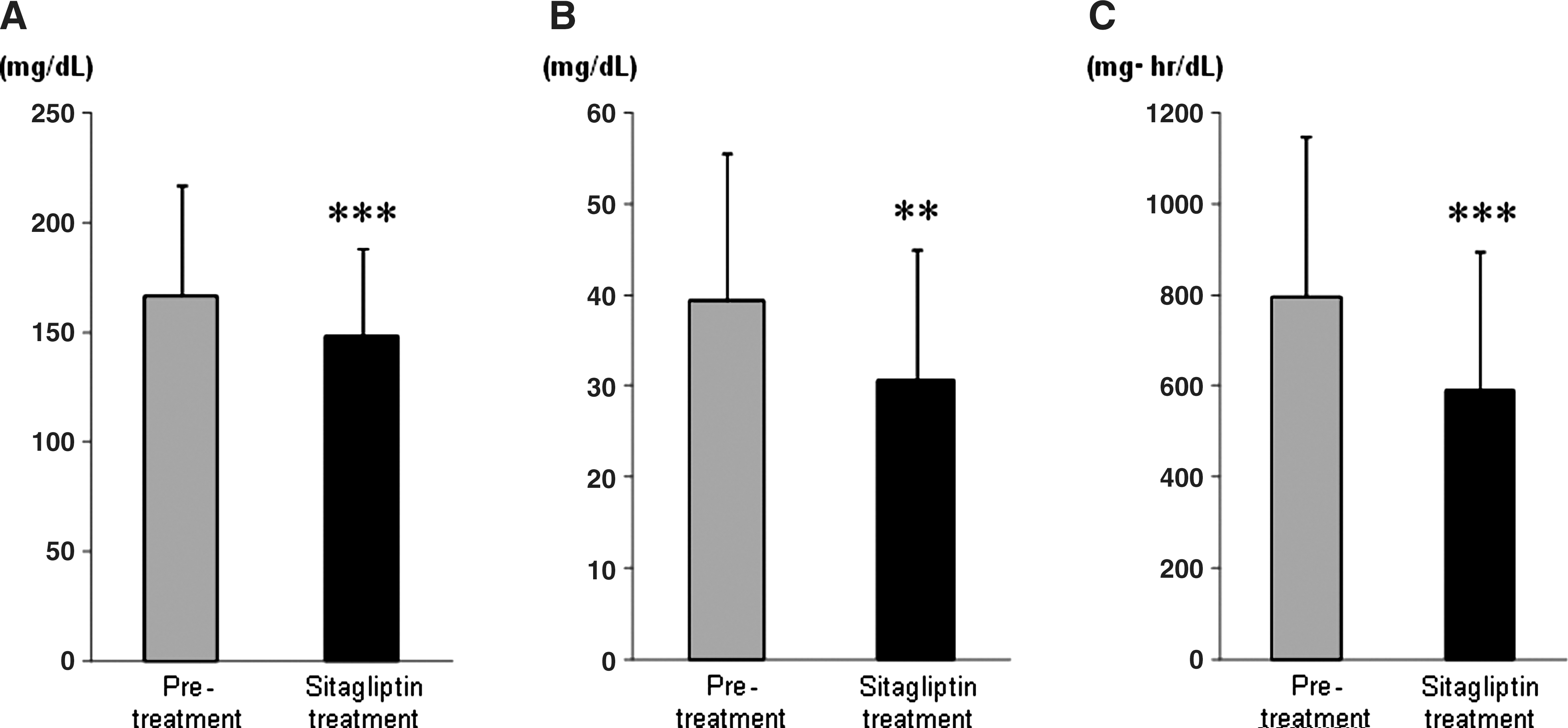
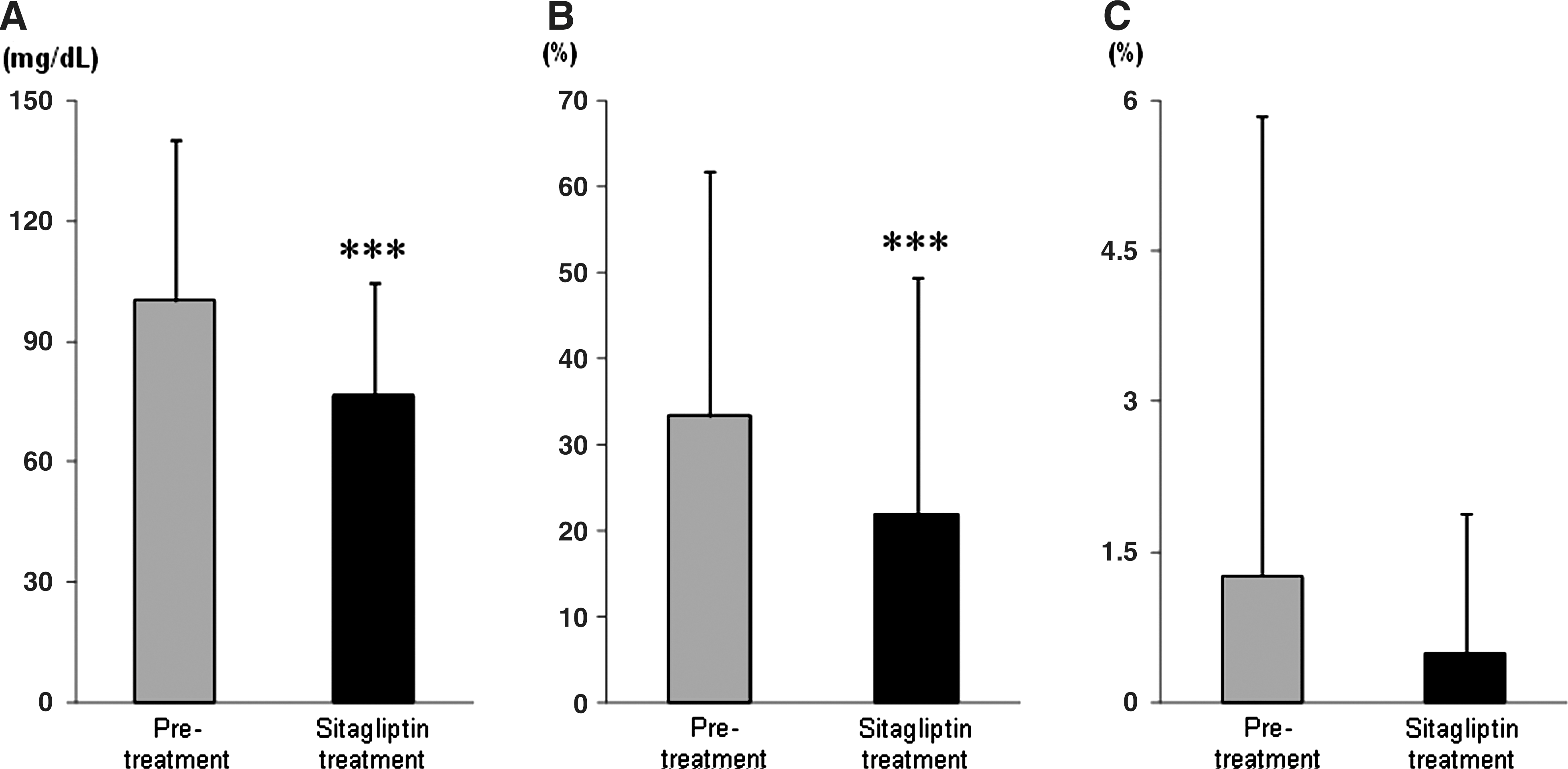
Glycemic changes obtained by CGM before and after administration of sitagliptin are shown in Figure 2. These data are averaged over all subjects. Hyperglycemia observed after meals before administration was improved by sitagliptin. The nighttime fasting glucose level was also decreased compared with the level before administration. The average 24-h glucose level, SD of the 24-h glucose level, and 24-h glycemic fluctuation were all significantly decreased after administration, compared with these data before administration (Fig. 3). MAGE and the time period of hyperglycemia (blood glucose level >180 mg/dL) were also significantly decreased after administration of sitagliptin (Fig. 4). All of these parameters showed similar improvement in patients treated with sitagliptin alone and those that received a concomitant sulfonylurea drug.

Changes in 24-h blood glucose before and after administration of sitagliptin. The data are averages from 30 subjects.
(
(
The correlation between decreases in average glucose levels after sitagliptin administration and average glucose levels before administration is shown in Figure 5. These data showed a significant negative correlation, suggesting that the decrease was greater when the average glucose level before administration was higher. A similar significant negative correlation was found between MAGE before sitagliptin administration and changes in MAGE after administration (Fig. 6). Again, this suggests that improvement of glycemic control by sitagliptin is likely to be greater in patients with high MAGE before administration.
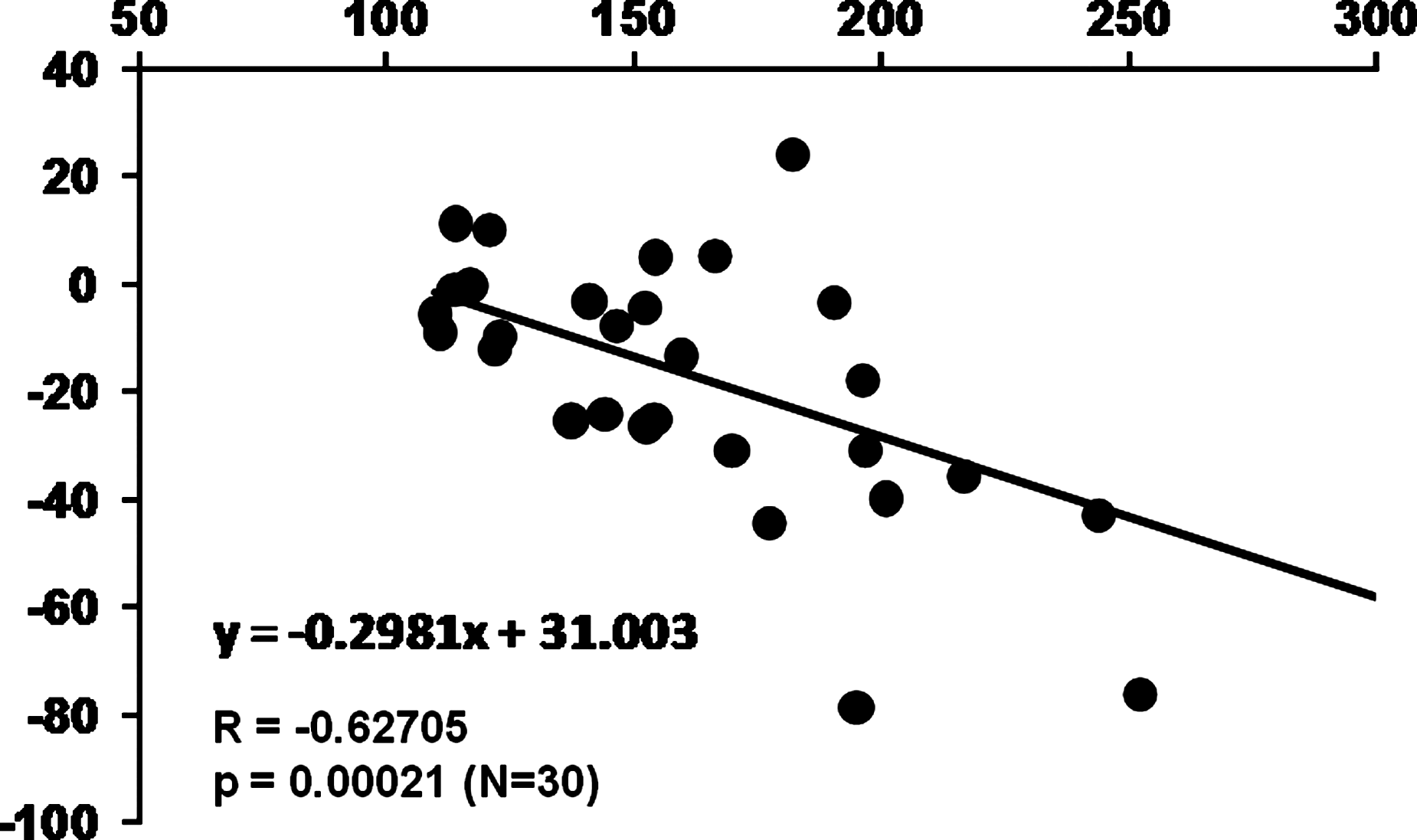
Correlation between average 24-h blood glucose levels before administration of sitagliptin and decreases in average 24-h blood glucose levels after administration.

Correlation between mean amplitude of glucose excursion before administration of sitagliptin and decreases in mean amplitude of glucose excursion after administration.
Discussion
DPP-4 inhibitors increase the activity of glucagon-like peptide-1 and glucose-dependent insulinotropic polypeptide, which are endogenous incretin hormones that regulate glucose-dependent insulin and glucagon secretion, and this effect improves hyperglycemia. 9 Thus, whereas sulfonylureas and glinide drugs decrease the glucose level through a direct action on insulin secretion with closing of KATP channels of pancreatic β cells, 10 the effect of a DPP-4 inhibitor such as sitagliptin depends on the blood glucose level itself. 11 In this study, the average 24-h blood glucose level was decreased by sitagliptin, and this effect was mainly due to improvement of postprandial hyperglycemia.
The glycemic changes after administration of sulfonylurea drugs to patients with type 2 diabetes suggest that these drugs decrease the average 24-h glucose level, based on the HbA1c value, but do not decrease the range of glycemic fluctuation, as well as decrease postprandial hyperglycemia and the fasting glucose level to a similar extent. 12 Administration of sitagliptin alone and concomitant administration with a sulfonylurea drug decreased the average glucose level and improved glycemic fluctuation. Thus, sitagliptin appears to be a more appropriate drug for improvement of postprandial hyperglycemia and is also likely to improve glucose spikes, which cannot be monitored using HbA1c only, and prevent macrovascular complications.
In this study, we found a significant decrease in the time period of hyperglycemia (blood glucose level >180 mg/dL), but the period of hypoglycemia did not increase and actually showed a tendency to decrease. Vildagliptin, another DPP-4 inhibitor, has been found to significantly increase the level of glucagon in blood in a hypoglycemia clamp study. 13 Incretin hormones have various bioactivities other than a direct increase in insulin secretion via receptors on the pancreatic β cell membrane. 14 –16 Expression of a glucagon-like peptide-1 receptor has been shown in the central nervous system, 16 and a preclinical study showed that glucagon-like peptide-1 signals in the central nervous system control glucose uptake and production in the peripheral tissues. 17 Therefore, sitagliptin may also maintain homeostasis of blood glucose via the central nervous system through increased activity of incretin, in addition to having a direct action in pancreatic β cells.
The extent of the decrease in the average blood glucose level induced by sitagliptin was correlated with the average glucose level before administration. This indicates that patients with a higher glucose level before administration of sitagliptin are likely to have a greater decrease in the glucose level. These data confirm the results of Japanese and overseas clinical studies with sitagliptin, which have shown that the decrease in the glucose level is greater in patients with a higher HbA1c level before administration. 18 –20 The findings also support the evaluation of drug efficacy with CGM because they show that changes in the average 24-h glucose level are related to changes in HbA1c. The MAGE level before sitagliptin administration was also correlated with the decrease in MAGE after administration, which suggests that larger glycemic fluctuation may result in a greater effect of sitagliptin in maintaining the homeostasis of blood glucose.
Conclusions
The results of this study suggested that sitagliptin, a DPP-4 inhibitor, not only decreases the average blood glucose level, but also greatly improves postprandial hyperglycemia. Thus, sitagliptin can improve 24-h glucose swings, that is, maintain the homeostasis of blood glucose.
Footnotes
Author Disclosure Statement
No competing financial interests exist.