
Abstract
Background:
Real-time (RT) continuous glucose monitoring (CGM) offers the possibility to better manage glucose levels during exercise in active individuals with type 1 diabetes mellitus (T1DM). However, studies have yet to determine the appropriate actions to take when glucose levels are trending toward hypoglycemia. The purpose of this observational field study was to test the effectiveness of RT-GCM and a new carbohydrate intake algorithm designed for maintaining euglycemia during sports.
Methods:
During a 2-week sports camp, 25 adolescents (8–17 years old) with T1DM were fitted with a RT-CGM device and instructed to ingest fast-acting carbohydrates (8–20 g, depending on the concentration of glucose at the time of RT-CGM alert and rates of change in glycemia) when glucose levels were trending toward hypoglycemia. Rates of change in glucose were measured before and after algorithm use, and the incidence of hypoglycemia was documented.
Results:
With RT-CGM and algorithm use, euglycemia was largely maintained with modest amounts of carbohydrate intake, even when glucose levels were initially dropping at an elevated rate (>0.55 mmol/L per 5 min). Mild biochemical hypoglycemia (3.0–3.9 mmol/L) occurred just twice out of 22 uses of the algorithm (9%) when trend arrows alerted the subjects that glucose levels were dropping. When glucose levels were already below target (<5.0 mmol/L), mild hypoglycemia occurred five times out of 13 events (38%), despite 16 g of carbohydrate being ingested. Average glucose levels during sports in the 60 min following algorithm use were 5.8 ± 1.2 mmol/L, 5.3 ± 1.0 mmol/L, and 6.2 ± 0.8 mmol/L in the 20-, 16-, and 8-g carbohydrate intake protocols when glucose levels were initially on target but dropping toward hypoglycemia.
Conclusion:
When coupled with RT-CGM, a new carbohydrate intake algorithm prevents hypoglycemia and maintains euglycemia during exercise, particularly if patients ingest carbohydrate when trend arrows alert them of a drop in glycemia.
Introduction
Even mild hypoglycemia impairs sports performance in youth with T1DM, 8 similar to how it lowers cognitive processing and math performance scores. 9 To avoid these negative outcomes, some young people with T1DM may avoid regular exercise altogether, whereas others may consume excessive amounts of carbohydrates or lower their insulin intake too dramatically, thereby causing hyperglycemia. Unfortunately, hyperglycemia caused by excessive carbohydrate intake, or too low a level of circulating insulin, may attenuate any potential improvement in glycemic control that regular exercise might cause.
Although guidelines for reductions in insulin administration and carbohydrate intake prior to exercise do exist, 1 these recommendations are challenging to implement as both the duration and intensity of activity need to be predetermined. In addition, reductions in basal and/or bolus insulin administration may cause pre-exercise hyperglycemia and may not always prevent hypoglycemia altogether. 3,10 As an alternative, increased consumption of carbohydrates can be used to limit hypoglycemia, 1 although the recommended amount is largely based on estimates of carbohydrate utilization rates rather than the concentration of glucose at the time of exercise and/or the rate at which glucose concentration is dropping. As such, these recommendations can sometimes promote higher blood glucose levels than necessary and negate the beneficial effects of exercise on glycemia. These guidelines are considered as starting points only for patients and their families, and frequent blood glucose monitoring is always advised so that both hyper- and hypoglycemia during sports can be avoided. 1
With the recent advent of real-time (RT) continuous glucose monitoring (CGM) devices that show updated glucose levels every few minutes and that have directional arrows indicating rates of change in glycemia, more patients are moving toward their use during periods of increased physical activity to help prevent exercise-associated hypoglycemia. 11 However, there are no guidelines on the amount of carbohydrate to consume to prevent hypoglycemia when glucose levels are within a targeted range, but still dropping, because glucose production is not matching peripheral glucose disposal.
Thus, we investigated, in a field study design, the use of a novel carbohydrate intake algorithm to be used during exercise with RT-CGM, which considers both the interstitial glucose concentration at the time of exercise and the rate at which glucose is dropping during the activity. We hypothesized that when coupled with this carbohydrate intake algorithm, RT-CGM would prevent exercise-associated hypoglycemia and allow active individuals with T1DM to maintain their engagement in sports, without promoting untoward hyperglycemia.
Research Design and Methods
This observational field study was conducted at the York University Diabetes Youth Sports Camp in Toronto, ON, Canada, and was approved by the University's Human Participants Review Committee. This sports camp offers instructional coaching and competitive activities for T1DM youth, 8–18 years old, who participate in soccer, basketball, tennis, swimming, and track and field (facultyofhealth.blog.yorku.ca/diabetes-sports-camp/). Typically, campers arrive at 0830 h each day and have baseline capillary glucose monitored before initiating their selected activities (basketball, tennis, soccer, and track and field) and again at a hydration break (1000 h) and before lunch. Lunch is provided daily at 1200 h, and participants resume their sporting activities from 1300 h until approximately 1600 h. All participants were given information sheets in advance of the camp about published recommendations for reductions in basal insulin and mealtime bolus insulin, according to the International Society of Pediatric and Adolescent Diabetes. 1 The typical exercise intensity at the camp ranges between moderate (i.e., 5 METS) to vigorous (10 METS) activities and includes skills coaching, competitive games, and “free time.” Following a final capillary glucose measurement at approximately 1600 h, the youth depart the camp for the day. Following informed consent, 25 volunteers (12 girls and 13 boys) with T1DM (age [mean ± SD] = 13.0 ± 2.8 years; body mass index = 22 ± 3.5 kg/m2; body fat = 21 ± 7.0 %) were recruited from the summer 2010 session to wear RT-CGM devices and test the carbohydrate intake algorithm. Average duration of diabetes was 6.0 ± 2.6 years, and participants were in fair to good glycemic control at the time of the study (hemoglobin A1c = 8.1 ± 1.0%).
Volunteers were fitted with RT-CGM by a camp nurse (Guardian® Real-Time units or MiniLink® transmitters for connection with those participants on a sensor-augmented pump [Medtronic of Canada Ltd., Brampton, ON, Canada]), and the device was worn continuously for 2–6 days with onsite training. To mimic a real life experience, participants were instructed to view their interstitial glucose readings during lulls in activity and at hydration breaks. In addition, they were asked to follow a specific carbohydrate intake regimen, with some assistance from research volunteers, to prevent hypoglycemia (Fig. 1). The goal of this algorithm was to recommend a dose of fast-acting oral carbohydrate (Dex4®, Can-Am Care, Montreal, QC, Quebec) based on the level of glycemia and the trend arrows provided by the RT-CGM device when glucose levels were in target range (<7.0 mmol/L) but declining toward biochemical hypoglycemia (defined here as glucose <3.9 mmol/L). Once treated with carbohydrate, subjects were allowed to continue competing with their peers unless glucose levels dropped below 3.9 mmol/L. In all cases, if interstitial levels dropped below 5 mmol/L, participants were instructed to stop exercising, confirm capillary glucose, and treat with 16 g of glucose. This process was facilitated by diabetes-trained camp volunteers (medical students and young adult athletes with T1DM) who would confirm and record the RT-CGM glucose measurement at the time of algorithm use and provide and record the carbohydrate intake. For safety reasons, subjects were also instructed to stop their sporting activity and check their capillary blood glucose level with their own blood glucose monitor if they felt symptoms of hypoglycemia. In all occasions, participants resumed play following carbohydrate ingestion if their capillary glucose was above biochemical hypoglycemia.
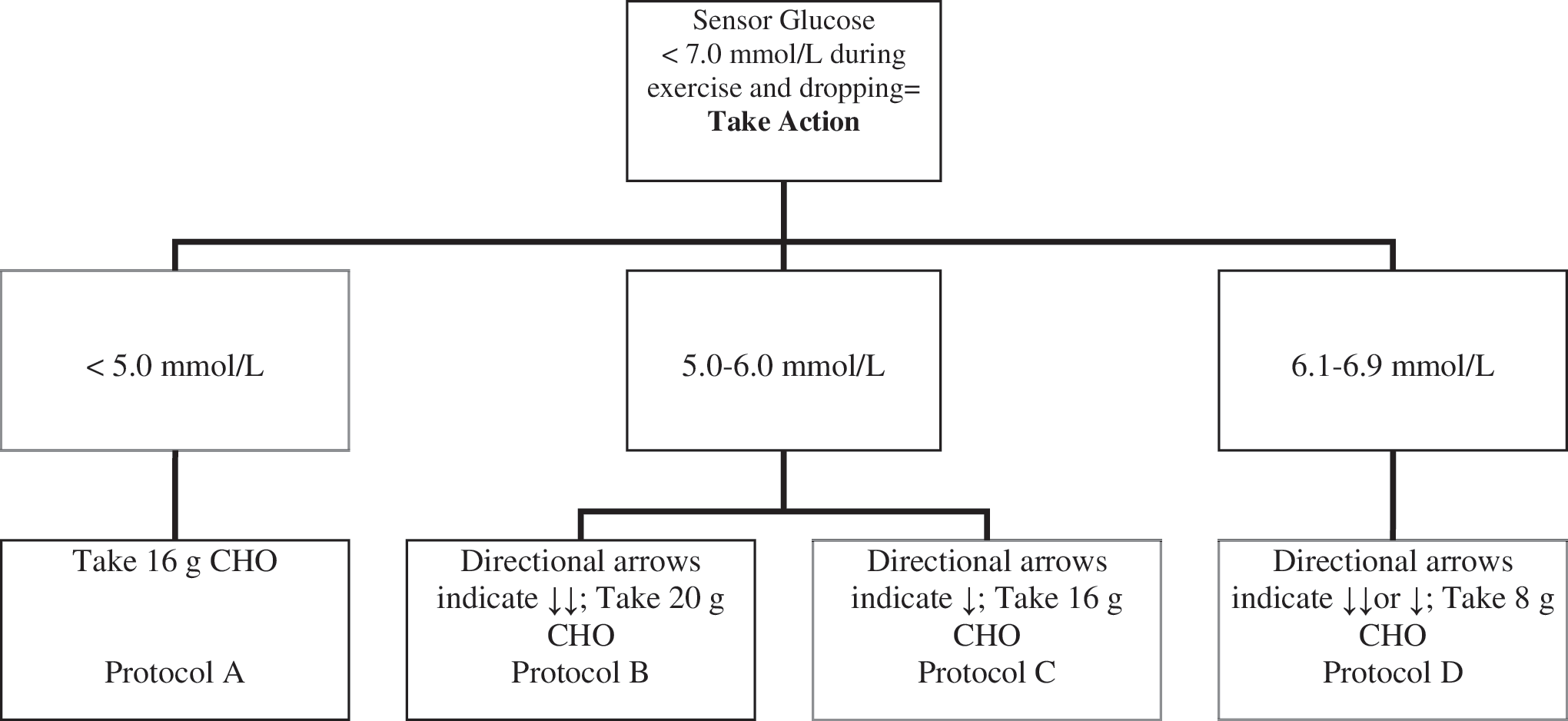
The real-time continuous glucose monitoring/carbohydrate (CHO) intake algorithm. When subjects noted that glucose levels were below 7 mmol/L, they would consume fast-acting CHO in the form of dextrose tablets (Dex4), with the amount ingested based on their glucose level and rate of change in glucose, as shown. Subjects would resume exercise once their glucose was ≥3.9 mmol/L. Note that two downward arrows on the real-time continuous glucose monitoring device (i.e., ↓↓) indicates that the glucose level is dropping at a rate >0.55 mmol/L per 5 min, whereas one downward arrow (i.e., ↓) indicates that the glucose level is dropping at a rate of 0.30–0.55 mmol/L per 5 min.
The general purpose of the algorithm is to achieve stable glycemic control during sports (defined here as RT-CGM values between 3.9 and 6.5 mmol/L) for as long as possible, once glucose levels dropped into range, without the need to interrupt the various sporting activities because of hypoglycemia. It was developed with the following considerations in mind: (1) carbohydrate intake would need to be high (i.e., 20 g) if current interstitial glucose level was in the euglycemic range but dropping at a high rate, as indicated by two downward trending arrows on the RT display window (>0.55 mmol/L per 5 min); (2) carbohydrate intake would need to be less (i.e., 8 g) if interstitial glucose was already slightly elevated (6.1–6.9 mmol/L) but levels were still declining at a moderate rate (0.30–0.55 mmol/L per 5 min, as indicated by a single downward trending arrow) or at a high rate (two downward trending arrows); (3) carbohydrate intake would need to be moderate (i.e., 16 g) if euglycemia had been achieved (i.e., 5.0–6.0 mmol/L) but glucose levels were declining modestly, as indicated by one downward trending arrow; and finally (4) carbohydrate intake would also need to be moderate (i.e., 16 g) if glucose values were already below target range (<5.0 mmol/L). It is important to note that this algorithm is reasonably easy to follow because individuals would simply note if their glucose levels were in target range and if levels were decreasing. For practical purposes, carbohydrate intake was provided in only three dosages and divisible by 4 (8, 16, and 20 g) because Dex4 tablets are equivalent to 4 g of carbohydrate each. Data from all algorithm events were grouped and analyzed according to the categories as shown in Figure 1. If meals and or snacks occurred, either 30 min before or in the 60-min follow-up analysis, these events were discarded because of the confounding variables associated with feeding (insulin, additional carbohydrates consumed).
Values are reported as means ± 1 SD in all tables, graphics, and text. A repeated-measures one-way analysis of variance was used to analyze glucose levels from 30 min before carbohydrate supplementation (denoted as zero-time) to 60 min following carbohydrate intake. Tukey's HSD post hoc tests were performed, against the zero-time glucose value, if a significant F ratio was achieved.
Results
Of the 25 participants, six subjects were excluded from analysis because of sensor loss or insufficient data for analyses (i.e., sensor data loss, sensor fell out, or less than 24 h of data was collected). One additional algorithm event was discarded from one boy as it was discovered that he infused insulin at the time of carbohydrate intake using his pump “wizard,” thereby resulting in subsequent hypoglycemia. Anthropometric and clinical data for the 18 subjects who used the carbohydrate intake algorithm is shown in Table 1. Of the 18 volunteers included in the analyses, average sensor wear time was 2.9 days, with a total of 35 captured algorithm events during daily sports. Figure 2 shows interstitial glucose levels for all events subdivided to the various treatment arms of the algorithm. When glucose levels were already below target (<5.0 mmol/L) and when carbohydrates were consumed, five out of 13 possible cases of mild hypoglycemia occurred (Fig. 2A). The lowest CGM value recorded in that arm of the algorithm was 3.00 mmol/L, occurring at 20 min following the 16 g of carbohydrate intake. When subjects were alerted via trend arrows that their glucose concentrations were dropping (for a total of 22 events), mild hypoglycemia (3.0–3.9 mmol/L) occurred only twice, both in the 16-g protocol (Fig. 2B–D). We observed no hyperglycemia (glucose >10 mmol/L or 180 mg/dL) during the time frame of investigation in any of the 35 events (30 min prior to and 60 min following carbohydrate intake).

Combination of real-time continuous glucose monitoring and the new carbohydrate intake algorithm prevents exercise-induced hypoglycemia during exercise. (
BMI, body mass index; HbA1c, hemoglobin A1c; MDI, multiple daily injections.
Average glucose levels in the 60 min following carbohydrate intake were 5.8 ± 1.2 mmol/L, 5.3 ± 1.0 mmol/L, and 6.2 ± 0.8 mmol/L in the 20-, 16-, and 8-g intake protocols, when their glucose levels were initially dropping toward hypoglycemia (not significantly different from each other). Average glucose level in the 60 min of exercise following carbohydrate intake when mildly low glucose levels had already occurred and subjects then consumed 16 g of carbohydrate was 4.6 ± 1.1 mmol/L.
Discussion
In this observational study, we show that the use of a RT-CGM device, coupled with a new carbohydrate intake algorithm, helps to prevent hypoglycemia and maintains good glycemic control during prolonged exercise in physically active youth with T1DM. Moreover, we show that if a mildly low interstitial glucose concentration is detected (i.e., glucose levels 4.0–5.0 mmol/L) during sports, then severe hypoglycemia (glucose <3.0 mmol/L) is largely preventable with 16 g of carbohydrate intake, even if physical activity is continued after a brief interruption in play. These findings are important as hypoglycemia is a major barrier to physical activity participation in youth with T1DM, and excessive carbohydrate intake or insufficient insulin administration may negate the beneficial effects that exercise has on glycemia in this patient population.
Hypoglycemia is the major barrier to achieving “tight” glycemic control in patients with T1DM 12 and is the major side effect of physical activity participation for youth with the disease. 1 Hypoglycemia is also a major deterrent for participation in sports and exercise 13 and it can impair performance and cognitive processing in active youth. 8 Moreover, antecedent hypoglycemia appears to increase susceptibility for exercise-induced hypoglycemia 14 which in its most severe cases can cause loss of consciousness, seizures, and severe organ (muscle, liver) injury. 7 Therefore, glucose levels during sports should be ideally between 5.0 and 9.0 mmol/L to maximize performance and safety in youth with T1DM, 1 although it is very challenging for individuals to maintain this level of glycemia once the exercise begins because of the rapid increase in glucose disposal that occurs at the onset of the activity. According to a recent Diabetes Research in Children Network study, approximately 80% of adolescents will have a drop in blood glucose level during exercise by more than 25% when pre-exercise blood glucose levels are >7 mmol/L. 4 If blood glucose levels are below 7 mmol/L (126 mg/dL) at the start of 45 min of exercise, then 86% of youth with T1DM either develop hypoglycemia (blood glucose <3.5 mmol/L) or require carbohydrate intake to prevent hypoglycemia during the activity. 4
Carbohydrate feeding, both prior to and during exercise, has long been known to help limit hypoglycemia during sports; however, the amount, type, and timing of carbohydrate intake are often debated. In one study, when the exercise occurred when insulin levels were peaking, up to 1.5 g of fast-acting carbohydrate/kg of body weight/h (approximately 80 g for a 55-kg adolescent) was required to prevent glucose levels from declining in youth with T1DM. 15 This high amount of carbohydrate intake contrasts with that recommended by some authors 16 and professional organizations 17 in which 15–30 g of carbohydrate is to be consumed for 30–60 min of activity. In this study, we found that modest amounts of fast-acting carbohydrate (8–20 g) were sufficient in preventing hypoglycemia for at least 60 min of activity in adolescents weighing from approximately 40 to 70 kg when prior reductions in bolus and/or basal insulin had been implemented. This amount of carbohydrate was chosen in part because of estimated circulating glucose requirements and because of the convenience of the tablets used (4 g per tablet). Perhaps a better approach, which would be expected to reduce the variability in our results, would have been to provide the carbohydrate based on the individual's body mass rather than based on convenience. Surprisingly, however, we found fairly consistent glycemic responses to the different doses of carbohydrate even though our subjects differed markedly in age and size (Table 1).
When hypoglycemia occurs during sports, current guidelines recommend stopping exercise, treating with 15 g of fast-acting carbohydrate, waiting 15 min, and then retesting again and treating further if glycemia is not restored. 2 This approach is clearly undesirable and frustrating for many individuals. Although 15 g of glucose has been proposed to increase glucose levels by 3–4 mmol/L (55–70 mg/dL) in a resting hypoglycemic child who weighs approximately 50 kg, 18 this recommendation has not been tested in the context of exercise. In this study, we found that 16 g of carbohydrate when taken when glucose levels were mildly hypoglycemic prevents severe but not mild hypoglycemia and increases glycemia by approximately 1.5 mmol/L (Fig. 2A). However, because glucose levels still dropped below 3.9 mmol/L in five of 13 of the participants (∼40%), we recommend that either a higher threshold in glycemia may be needed for carbohydrate intake during exercise (i.e., 5.5 mmol/L) or that greater amounts of carbohydrates are required when glucose levels drop below 5.0 mmol/L. Because CGM tends to overestimate glucose concentrations when blood glucose values are dropping during exercise, 19 carbohydrate intake at a higher glucose threshold will likely be of greater benefit in preventing hypoglycemia.
In this study, we show that the consumption of just 8 g of carbohydrate is needed when glucose levels are somewhat elevated (between 6.0 and 7.0 mmol/L) but still declining during sports (Fig. 2D). Based on the limited data collected in this arm of the algorithm (only six events tested), this approach appears reasonably effective in preventing hypoglycemia and maintaining glucose in a targeted range. In this study, we also show that higher amounts of carbohydrate intake (20 g) tend to have a more variable glucose response than lower amounts (i.e., 8 g), likely because of the large intersubject variability in glucose disposal rate among the subjects tested. Again, however, the limited data collected in this arm of the algorithm (only five events) severely limit its generalizability to a larger population of active individuals with T1DM.
Our limited observations support the notion that the use of RT-CGM and a new carbohydrate intake algorithm may help facilitate improved short-term glycemic control during exercise in youth with T1DM. It is important to note, however, that this carbohydrate intake algorithm is not designed to replace the reduction in insulin dosage or the pre-exercise carbohydrate snack recommended by several authorities, 1,2,17 but rather to help “fine tune” glucose levels once they have reached a targeted range. All participants in this camp setting were advised about insulin adjustments for increased physical activity, 1,2,17 and most subjects in this study had reduced insulin administration (either basal or bolus) by anywhere from 20% to 50%. Indeed, in all cases in which the algorithm was used, subjects were maintained in a near euglycemic state for 90 min of sports (i.e., 30 min before carbohydrate intake and 60 min following intake). This accomplishment is seldom achieved in situations outside of a clinical laboratory setting in which glucose levels are “clamped” euglycemic using constant rate insulin administration and variable-rate glucose intravenous infusions. 20 –22 Further investigation is needed to determine, however, if this new RT-CGM/carbohydrate intake algorithm approach works on a larger population of active adolescents with T1DM, in a more controlled experimental environment, and if this approach to fine tune exercise glycemia can help improve overall metabolic control in these individuals.
Other limitations of this current field setting study are that it lacks a proper control group (i.e., the subject's interstitial glucose levels measured during exercise without the use of RT-CGM and the use of the carbohydrate intake algorithm) and that the intensity and duration of physical activity were not standardized. Moreover, the amount of “on board” bolus insulin likely varied markedly among the participants, as did their body weight (ranging from 38.5 kg to 68.4 kg), thereby making generalizable recommendations difficult. However, it is already well established that prolonged exercise causes a linear drop in glycemia in adolescents with T1DM, which is largely reproducible for a given individual. 23 This drop in glycemia occurs even if there is little to no “on board” bolus insulin because the exercise takes place several hours after their last bolus injection. 24 One advantage of RT-CGM is that the rapid decrease in glucose levels, typically caused by excessive insulin concentrations in the circulation, can be displayed, and the user can be alerted to consume carbohydrate, as was performed in this study. Using blinded CGM in an identical camp setting, we have observed high rates of both hyper- and hypoglycemia both during and after exercise. 8,24 In our most recent study of nearly identical adolescents with T1DM in a sports camp setting, we documented that four of 11 (36%) subjects wearing blinded CGM had hypoglycemia (<3.6 mmol/L) at some point during the camp hours (9 a.m.–4 p.m.) on day 2 of the camp, whereas seven of 10 (70%) subjects had hypoglycemia at some point during day 4 of the camp. Moreover, the duration of hypoglycemia ranged anywhere from 15 min to 2.5 h in that study. 8 These findings contrast markedly to what we observed here with unblinded CGM, in which only seven episodes of mild hypoglycemia occurred out of 35 captured events (∼20%), with all events lasting less than 20 min. These comparisons should be interpreted with caution, however, because the average sensor analysis period between these two studies differed (3 days in the current study vs. 2 days in the other study) and the campers in this study were supported by counselors who were assisting the subjects in the use of RT-CGM and who were ready to provide carbohydrate to them when the downward directional arrows were observed.
In summary, we show that the use of RT-CGM, coupled with a newly designed carbohydrate intake algorithm that takes into account the level of glycemia during sport and directional rate of change arrows, appears to reduce the risk of hypoglycemia and helps to promote euglycemia during exercise in active youth with T1DM. These preliminary observations may have important clinical applications for active CGM users who are engaged in sports and who are at high risk for exercise-associated hypoglycemia.
Footnotes
Acknowledgments
The authors would like to acknowledge the research participants and volunteers of the 2010 York University Diabetes Sports Camp for their enthusiasm and support in this project. The RT-CGM devices and Dex4 glucose tablets were generously donated to the Sports Camp by Medtronic Canada and Can-Am Care Co., respectively. The authors would like to thank Katherine Iscoe for her editorial suggestions on this article. The carbohydrate intake algorithm was developed by M.C.R. and J.M. with input from Mr. Dylan Kelly. Study design and data collection were performed by M.C.R. and J.M. The data analysis and manuscript were written by M.C.R.
Author Disclosure Statement
M.C.R. has received speaker's honoraria from Medtronic.