
Abstract
Background:
Universal screening for gestational diabetes mellitus (GDM) is advocated in Indian women as they have the highest frequency of GDM among the South Asian population. For this the diagnostic procedure has to be simple, economical, and evidence based. Hence, this study was undertaken to compare point-of-care measured capillary whole blood glucose (CBG) with a glucometer and laboratory-estimated venous plasma glucose (VPG) and to suggest which is feasible as a diagnostic tool.
Methods:
Consecutive pregnant women in the third trimester were included in this study with the approval of the institutional ethical committee. They were given 75 g of oral glucose in the fasting state. After 2 h, CBG was measured by finger prick using an Accu-Chek® glucometer (Roche Diagnostics India Pvt. Ltd., Mumbai, India), and venous blood was drawn to estimate VPG in the laboratory by the glucose oxidase–peroxidase method. The diagnosis of GDM was based on a 2-h plasma glucose level of ≥7.8 mmol/L (World Health Organization criteria).
Results:
Among 819 pregnant women, 86 (10.5%) were diagnosed as having GDM. The CBG value at a 2-h plasma glucose level of ≥7.8 mmol/L had a sensitivity of 80.2% and specificity of 98.5% with false-positive and false-negative rates of 1.5% and 19.8%, respectively. The area under the receiver operator characteristic curve of CBG was 0.991.
Conclusion:
The CBG value at a 2-h plasma glucose level of ≥7.8 mmol/L may be recommended for the diagnosis of GDM in healthcare centers where laboratory technology is not available.
Introduction
To perform universal screening, we need a near-patient technology that offers the same precision as laboratory analysis. In community health centers, pregnant women are not too willing to permit venous blood to be drawn for estimating plasma glucose (PG). In Europe, most blood sugar determinations are performed with capillary whole blood using portable blood glucose meters, 5 which is a patient-friendly approach. Hence, we also wanted to ascertain the use of glucometer to diagnose GDM in our population. With the above aim, this study was undertaken to determine the sensitivity and specificity of capillary whole blood glucose (CBG) in comparison with venous PG (VPG) in diagnosing GDM. The expected outcome of this study is to suggest a method that would be convenient, ethical, and economical to diagnose GDM in the community.
Patients and Methods
Consecutive pregnant women, between 24 and 28 gestational weeks, attending the prenatal clinics in the community health center of Chennai city, Tamil Nadu, India were included in the study. Approval of the institutional ethical committee was obtained before carrying out the study. Informed consent was taken from all pregnant women to perform CBG testing and to draw venous blood samples for estimating PG. They were given a 75-g glucose load orally in the fasting state, and venous blood samples were collected at 2 h. A simultaneous finger-prick was performed using Accu-Chek® Active glucometer (Roche Diagnostics India Pvt. Ltd., Mumbai, India) standardized for estimation of PG by qualified technicians. The glucometer was calibrated and validated following the manufacturer's guidelines. VPG was measured by the glucose oxidase–peroxidase method in a Hitachi (Tokyo, Japan) autoanalyzer. The diagnosis of GDM was based on having a 2-h 75-g post glucose value of ≥7.8 mmol/L (World Health Organization criteria).
Statistical methods
To determine the linear relationship between the intravenous method and the capillary method in estimating the 2-h glucose value, the correlation coefficient was computed. Linear regression analysis was done to find the predictive equation, in order to predict 2-h PG value of the venous blood sample corresponding to the observed CBG. Sensitivity (measures the proportion of actual positives that are correctly identified as such), specificity (measures the proportion of negatives that are correctly identified), false-positive (proportion of absent events that yield positive test outcomes [i.e., the conditional probability of a positive test result given an absent event]), and false-negative (proportion of events that are being tested for which yield negative test outcomes with the test [i.e., the conditional probability of a negative test result given that the event being looked for has taken place]) were computed to validate the capillary method in detecting GDM. The receiver operating characteristic curve was drawn to analyze the predictive power of the constructed equation. The coefficient of variation was calculated to study the variability of VPG and CBG.
Results
In total, 819 pregnant women were included in this study. The clinical characteristics of the pregnant women are given in Table 1. The 2-h PG value by the intravenous method glucose oxidase method (Hitachi) and 2-h PG value by CBG were obtained simultaneously in all women. Among the 819 pregnant women, 86 (10.5%) were diagnosed as having GDM by World Health Organization criteria. In order to examine the relationship between glucose measured in CBG and VPG, the correlation coefficient was computed. It was 0.961.
BMI, body mass index.
The linear regression equation with the PG value obtained by the intravenous method as the dependent variable and the capillary method value as the independent variable was constructed in order to predict the intravenous value for a given capillary value. The linear regression equation was VPG=0+0.974×CBG. The 95% confidence interval for the regression coefficient was 0.970–0.978. This interval was very narrow, indicating the precision of the regression coefficient. The predicted capillary 2-h PG value and the observed intravenous value in diagnosing the GDM are given in Table 2.
In this analysis it is observed that the mean glucose value of the VPG method is lower than the capillary method (i.e., 6.16±1.38 vs. 6.31±1.42 mmol/L). The capillary method has a sensitivity of 80.2% and specificity of 98.5% at 7.8 mmol/L. The false-negative rate is 19.8%, and the false-positive rate is 1.5%. This result indicates that the capillary method predicts almost all positive cases.
Receiver operator characteristic analysis was done for the predicted values using the fitted equation (Fig. 1). The analysis indicates that the area under the curve is 0.991. This implies that the prediction power of the constructed equation is very high (Fig. 1). The coefficient of variation in VPG is 22.41%, and that in CBG is 22.50%. The variability of the values is almost identical.
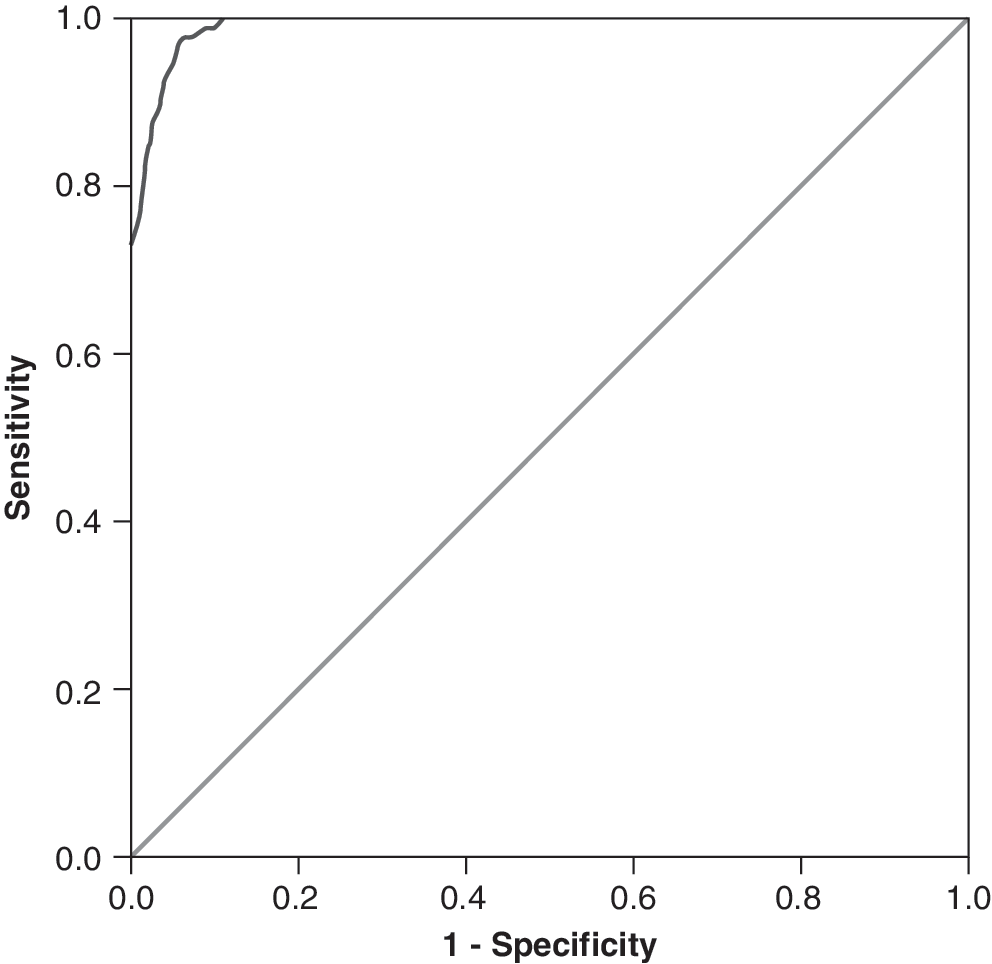
Receiver operator characteristic curve of (1 – specificity) versus sensitivity. Diagonal segments are produced by ties.
Discussion
In this study, we estimated CBG, and at the same time venous blood was drawn to measure VPG in the laboratory. This methodology was adopted as pregnant women were always eager to know their glycemic status at the time of testing itself. On the following day, they were informed of the laboratory values.
In populations at high risk for GDM, the recommendation of screening every pregnant woman with the oral glucose tolerance test is very demanding. 6 The most commonly used method to diagnose glucose intolerance of varying degrees is based on the measurement of VPG. This procedure requires both sophisticated equipment and technical staff that may not be available in all places, particularly in developing countries, which precludes universal screening. Alternatively, a simple procedure of measuring CBG seems to be more convenient than measuring VPG in general practice. 7 In support, a study revealed that CBG values best approximated VPG values in healthy populations. 8 That the recommendations for diagnosis of diabetes by the World Health Organization using CBG and VPG concentrations as the value 2 h after a 75-g glucose load are equivalent 9 is also in agreement with the above observation, although other studies found that VPG 2 h after the glucose load differed from the CBG value by 0.28–0.5 mmol/L (i.e.,∼5–9 mg/dL). 10,11 In our study, the false-positive rate is as low as 1.5%, and the false-negative rate is almost 20%. Because the mothers are under constant follow-up until delivery, these 20% of the missed cases can easily be identified in the subsequent visits.
It is interesting that, in the diagnosis of GDM, the glucose measurement by CBG and VPG did not differ in the 1-h level (9.9 vs. 9.6 mmol/L) or the 2-h level (7.9 vs. 7.7 mmol/L). 12 Irjala et al., 13 in their study, collected venous and capillary blood specimens simultaneously for blood glucose determination. They examined the interrelations of CBG and VPG with respect to gestation, glucose tolerance, and analytical method. No significant capillary–venous difference was seen when VPG was estimated by the glucose dehydrogenase method. 13 Also, the predictive power of the constructed equation in our study evaluated by the area of the receiver operator characteristic curve was 0.991%.
The easiest and most cost-effective solution would be a 75-g oral glucose load and glucose measurement in capillary blood. 14 CBG determinations are the only qualified way to determine blood sugar in general practice at the moment, as up to now no venous blood devices with complete antiglycolytic derivatives are commercially available. 5 It is safe to diagnose diabetes using CBG provided one uses the equipment with high precision and given that continuous quality assurance procedures are used. 7 CBG values best approximated VPG values from the laboratory. 8 Dacus et al. 15 found by a simpler linear regression that the cutoff value for 2-h PG of ≥7.8 mmol/L had a strong correlation between capillary Accu-Chek and the laboratory values, and one value may be substituted for the other.
The strength of our study was inclusion of large numbers in our cohort for detecting GDM by both CBG and VPG. We were able to establish that Accu-Chek glucometer values were sufficiently accurate to substantiate the laboratory values. Self-monitoring of blood glucose is widely practiced with glucometers, both during pregnancy and outside pregnancy to manage a patient's glycemic status. Hence, a glucometer can be safely recommended for identifying GDM in the community. CBG is a feasible alternative, especially in developing countries where obtaining venous samples may be difficult. 16 If the CBG value is not substantiating the clinical suspicion that a pregnant woman might be having GDM, a laboratory test may be performed for confirmation.
Conclusions
In countries with fewer resources, CBG may be recommended for the diagnosis of GDM, as this procedure is least demanding in both technically trained manpower and equipment.
Footnotes
Acknowledgments
The Diabetes In Pregnancy Awareness and Prevention project was supported by grants from the World Diabetes Foundation. We would like to thank the Government of Tamil Nadu, India for granting permission to carry out this study.
Author Disclosure Statement
No competing financial interests exist.