
Abstract
Background:
Insulin lispro was subjected to a simulated in-use study in the Medtronic MiniMed Paradigm® pump system (Medtronic, Northridge, CA) under stressed conditions over 14 days.
Methods:
Basal and bolus insulin doses were delivered under conditions of elevated temperature (37°C) and continuous shaking over 14 days. The simulation included a study arm with infusion set changes every 3 days and an arm with no infusion set changes over the entire study period. Analyses were performed on samples pumped through the infusion system and on samples retained in the pump reservoir.
Results:
Results met U.S. Pharmacopeia criteria for insulin lispro potency through the entire testing period. No precipitation was observed on visual inspection, and no occlusion alarms were noted.
Conclusions:
Insulin lispro demonstrated appropriate physicochemical stability for up to 14 days in the MiniMed Paradigm pump system.
Background
However, efficacy and safety may be compromised if the insulin formulation is not stable in the pump. 10,11 The CSII delivery system subjects insulin formulations to stresses that may jeopardize stability, including agitation, exposure to device components, pH changes, and increased temperature. 12 Studies have suggested that aggregation or precipitation of the formulation due to these stresses may increase the risk for occlusion of the infusion set through formation of fibrils or precipitates. 13,14 Therefore, it is imperative that insulin formulations used in CSII demonstrate stability.
Previous in vitro stability studies have shown that a rapid-acting insulin analog, insulin lispro (Humalog®, Eli Lilly and Co., Indianapolis, IN), is stable in the reservoir of insulin pumps at 37°C (98.6°F) for up to 48 h; 15 it remains stable both in the reservoir and in 3-mL cartridges at 37°C (98.6°F) for up to 7 days. 16 In both studies, no changes of practical significance were noted in potency, purity, degradation, or degree of polymerization. Additionally, there were no instances of insulin precipitation or catheter occlusions. 15,16
The present study examined the chemical and physical stability of insulin lispro administered as basal and bolus doses that simulated patient use in the Medtronic MiniMed Paradigm® pump (Medtronic, Northridge, CA) and infusion system over a 14-day period under stressed conditions.
Materials and Methods
Study design
This simulated patient in-use study used basal and bolus doses of insulin lispro under conditions of elevated temperature, at 37°C (98.6°F), and continuous shaking over 14 days. There were two study arms: one with infusion set changes every 3 days (WC) and one with no infusion set changes throughout the study (NC). Reservoirs remained in the pumps and were not changed in either study arm for the study duration. In both arms, analyses were conducted on dosed samples and material remaining in the reservoir. Four 10-mL vials of insulin lispro were placed into 5°C (41°F) storage for use as baseline control samples. The baseline controls served as indicators of a zero-time sample condition.
Bolus dosing (three 6-U doses per day) occurred on four separate days. Bolus doses were separated by a minimum of 2 h and a maximum of 4 h. Samples were collected at the end of each bolus infusion day (Days 1, 5, 10, and 14).
A variable pumping rate was used for basal dosing. A basal rate of 0.8 U/h (19.2 U/day) was used on sample collection days, with a reduced rate on non-collection days (0.05 U/h, with a return to the 0.8 U/h basal rate 19 h prior to collection). This variable dosing-rate scheme balanced the need for insulin lispro exposure to pumping across the 14-day period with the 3-mL reservoir capacity.
Materials and infusion systems
Insulin lispro is a solution formulation (pH 7.4) containing zinc (0.0197 mg/mL), disodium phosphate (1.88 mg/mL), glycerin (16 mg/mL), and m-cresol (3.15 mg/mL). This study used one commercial lot (expired) of insulin lispro (U100) 10-mL vials. The device used for evaluation was the MiniMed Paradigm pump (model MMT 722NAS), along with MiniMed plastic reservoirs and infusion sets.
Testing conditions
The stress test procedure was developed through multiple discussions with the Food and Drug Administration (FDA). The procedure is consistent with recent draft guidance from the FDA. 17
The reservoirs of 20 pumps (10 for each study arm) were filled with insulin lispro. Infusion sets were attached to the reservoirs, and the reservoirs were loaded in the pumps according to the manufacturer's instructions. Each infusion set was then connected to a 3.5-mL collection vial.
Pumps were placed on a reciprocating shaker table (model R2, New Brunswick Scientific, Edison, NJ) capable of agitation at 100 strokes/min with a 1-inch total displacement. This table was placed inside an incubator (LAB-LINE, Imperial III, Forma Scientific, Marietta, OH) set at 37°C (±2°C). Infusion sets from the pumps led to collection vials that were placed outside the incubator.
The pumps and the insulin lispro were exposed to thermal and mechanical stress conditions continuously throughout the study, with interruptions only to collect the bolus doses, inspect the systems, and change the sample collection vials.
Sample collection
At the beginning of each of the four bolus dosing days, 3.5-mL Type 1 glass vials, fitted with halobutyl stoppers and secured by aluminum seals, were weighed and connected to each infusion set. Initial weights were recorded and used later to calculate delivered volume. The basal and bolus doses were then delivered. After 24 (±1) h, each collection vial was weighed to determine the total delivered volume into each vial; an average daily pumped volume was then calculated. The amount collected in each of the 10 vials on each bolus dosing day was pooled into one vial for each study arm. The pooled samples were stored at 5°C until analysis. Analysis results were compared with the acceptance criteria for that test.
Infusion sets were changed every 3 days for the WC study arm. During collection vial changeover, the tubing was visually inspected for color, precipitation, and occlusions, and the collected material was examined for color and clarity. At the end of the 14-day exposure, for each study arm, the material remaining in all reservoirs was pooled into a single 10-mL vial and submitted for analysis.
Sample analyses
Analyses were conducted on pooled samples collected after pumping through the infusion system and on samples retained in the pump reservoirs. In addition, a 5°C baseline control sample was analyzed. Both stress and baseline control samples were evaluated using high-performance liquid chromatography (HPLC) assays for insulin lispro. Analyses were similar to those in a previous study 16 and included physical appearance, pH, potency (U/mL), purity, high-molecular-weight protein (HMWP) content, and m-cresol content. These analyses were measured with HPLC methods that follow those described in the U.S. Pharmacopeia (USP) monograph for insulin lispro injection. 18
pH
Measurement of pH followed the USP method. 19
Insulin lispro potency
A reversed-phase chromatography method was used to determine insulin lispro potency by using a Waters Spherisorb ODS II (Waters Corp., Milford, MA), 3-μm particle size, 10-cm×4.6-mm i.d. column. The assay used a combination of 80:20 0.2 M sodium sulfate buffer (pH 2.3):acetonitrile and 70:30 0.2 M sodium sulfate buffer (pH 2.3):acetonitrile for mobile phase, which was mixed directly on the HPLC instrument. Flow was 0.8 mL/min with a column temperature of 40°C. Detection was by ultraviolet absorbance at 214 nm. Samples were acidified by adding 3 μL of 9.6 N hydrochloric acid/mL of drug product, and the injection volume was adjusted to 20 μL.
HMWP
Size exclusion chromatography was used to determine HMWP content by using a Waters Insulin HMWP, 30-cm×7.8-mm column with a mobile phase consisting of 65% 1.0 mg/mL
Purity
A reversed-phase chromatography method was used to determine A-21 desamido and other related substances. This method used a Vydac® Protein and Peptide C18, 25-cm×4.6-mm i.d. column (Grace Davison Discovery Sciences, Deerfield, IL), with a temperature of 40°C and a flow rate of 1.0 mL/min. The method used a gradient system with mobile phase A containing 82% 0.2 M sodium sulfate buffer (pH 2.3):18% acetonitrile and mobile phase B containing 50% 0.2 M sodium sulfate buffer (pH 2.3):50% acetonitrile. The gradient program began isocratically at 19% mobile phase B for 60 min, and then mobile phase B was increased linearly from 19% to 49% over a 23-min period. Initial conditions then returned to 19% mobile phase B and finally remained isocratic for at least 10 min to equilibrate the column for the next injection. Detection was by ultraviolet absorbance at 214 nm. Samples were acidified by addition of 3 μL of 9.6 N hydrochloric acid/mL of drug product. A volume of 20 μL was injected.
m-cresol
A reversed-phase chromatography method, which used a Vydac Protein and Peptide C18, 15-cm×4.6-mm i.d. column, was used to determine m-cresol content. The assay used a combination of 80:20 0.2 M sodium sulfate buffer (pH 2.3):acetonitrile and 70:30 0.2 M sodium sulfate buffer (pH 2.3):acetonitrile for mobile phase, which was mixed directly on the HPLC instrument. The column temperature was 40°C, and the flow rate was 1.0 mL/min. Detection was by ultraviolet absorbance at 270 nm. Samples were acidified by adding 3 μL of 9.6 N hydrochloric acid/mL of drug product. Standards and samples were prepared to a target concentration of approximately 0.64 mg/mL m-cresol using 0.01 N HCl as the diluent. A volume of 20 μL was injected.
Data acceptance criteria
Accuracy of delivered volume was determined by comparison with the device specifications (the average daily pumped volume across all pumps must be within±5% of theoretical each day). The specification for m-cresol was not less than 1.15 mg/mL, which is the minimum concentration necessary to meet USP antimicrobial effectiveness requirements for multi-use pharmaceutical products for injection. 20 All other results were expected to meet the acceptance criteria given in the USP monograph for insulin lispro injections, 18 as follows: insulin lispro potency, 95.0–105.0 U/mL; related substances, not more than 4.0%; A-21 desamido, not more than 1.5%; HMWP, not more than 1.5%; and pH 7.0–7.8.
Results
Dosed samples with infusion set changes (WC)
For the WC study arm, collected data included pH, potency, HMWP, purity (other related substances and A-21 desamido), m-cresol content, pump volume accuracy, and physical appearance.
pH
A pH of 7.40 was observed on Day 14. This was slightly higher than the baseline control (pH 7.26).
Insulin lispro potency
Figure 1 shows the potency results for the dosed WC samples. Results at all time points are presented along with the baseline control sample.
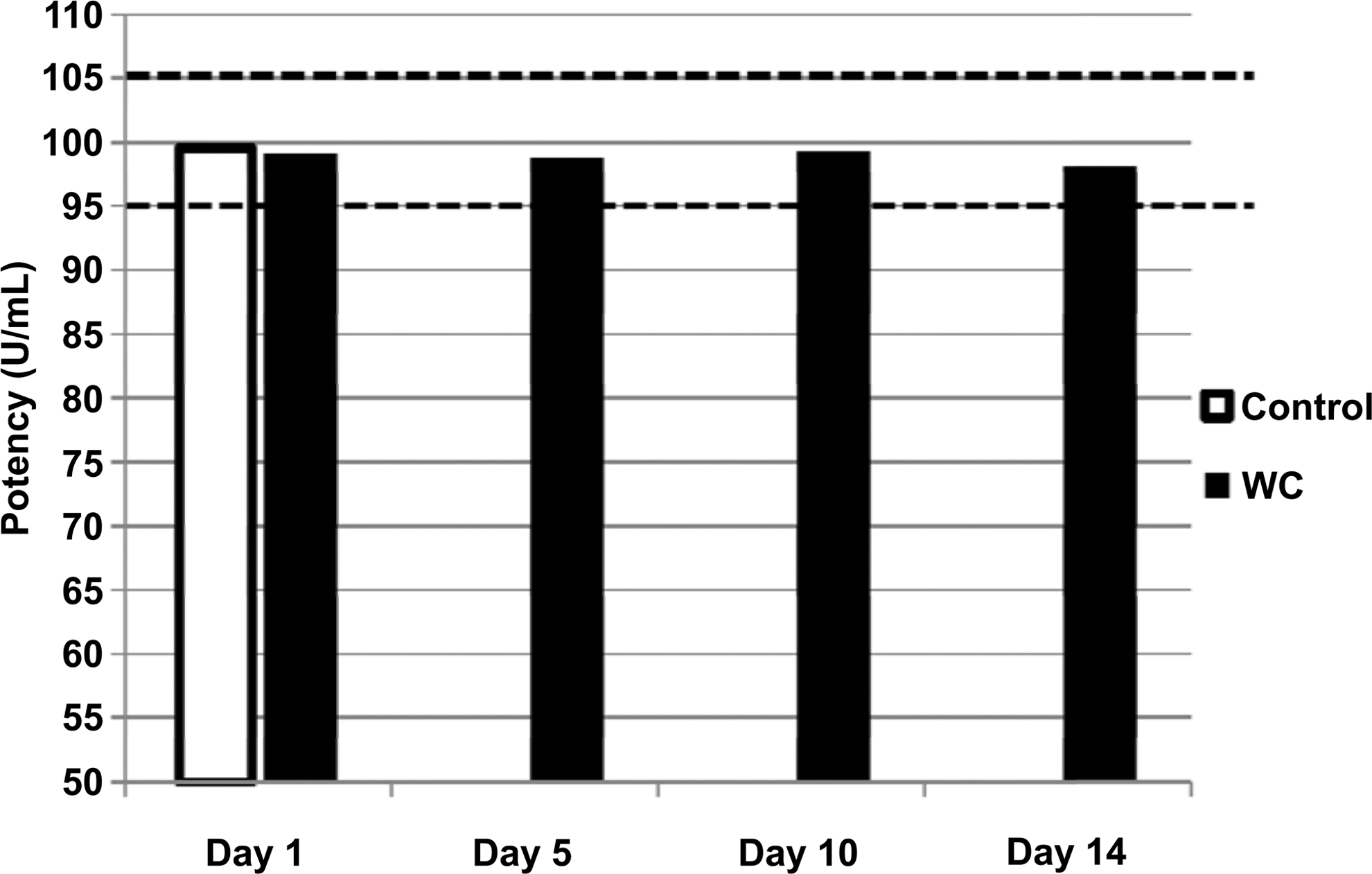
Insulin lispro potency data from dosed samples at four collection time points and a baseline control sample stored at 5°C without agitation. Infusion sets were changed every 3 days in the WC study arm. Dosed WC samples were delivered under conditions of elevated temperature (37°C) and continuous agitation. The dashed lines show the upper and lower specification limits (95.0 U/mL and 105.0 U/mL, respectively).
HMWP (polymer)
Figure 2 shows HMWP data for the dosed WC samples. Results at all time points are presented along with the baseline control sample.
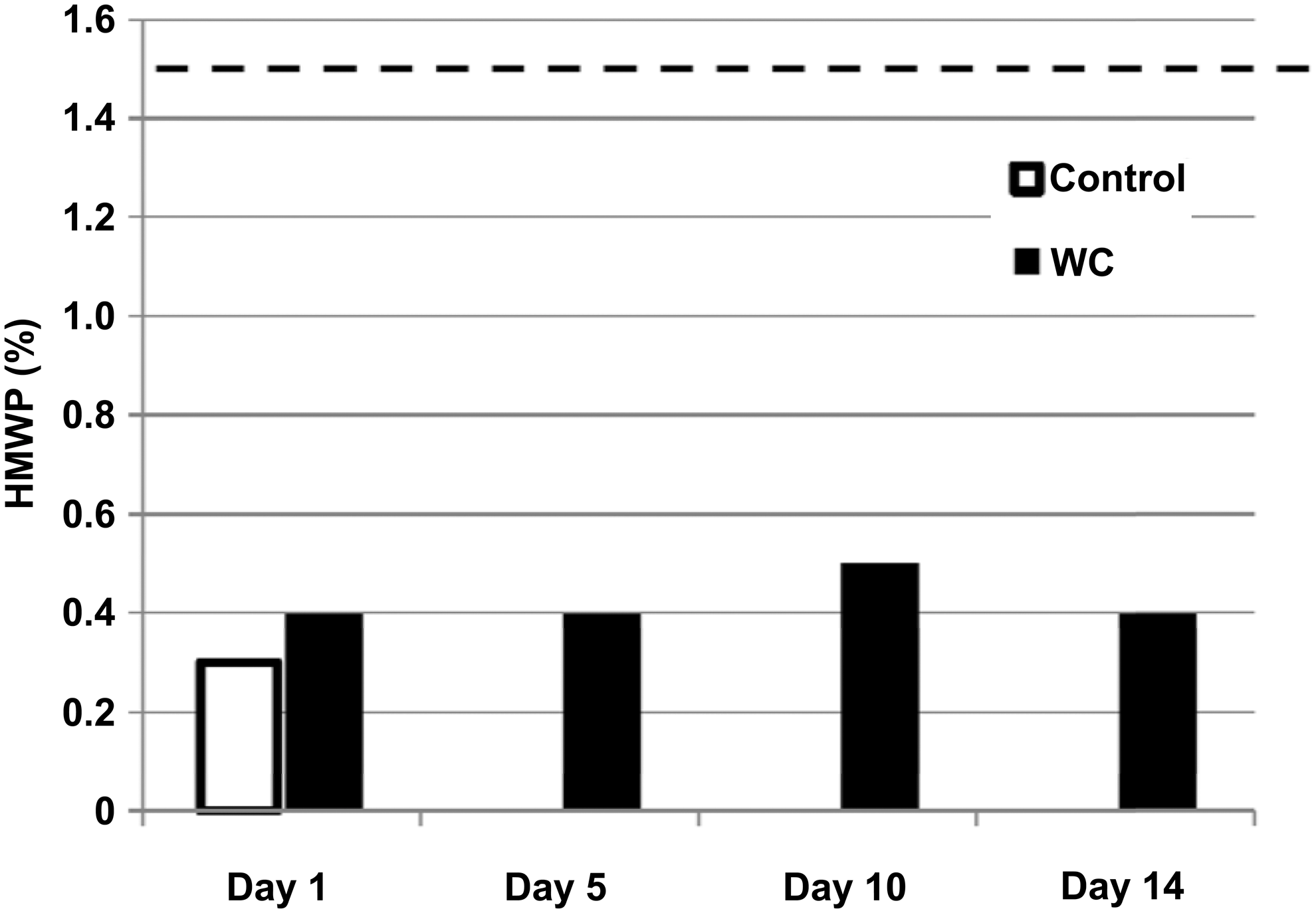
High-molecular-weight protein (HMWP) data for insulin lispro from dosed samples at four collection time points and a baseline control sample stored at 5°C without agitation. Infusion sets were changed every 3 days in the WC study arm. Dosed WC samples were delivered under conditions of elevated temperature (37°C) and continuous agitation. The dashed line shows the upper specification limit (1.5%).
Purity
Figure 3 shows both the A-21 desamido results and other related substances results for the dosed WC samples.
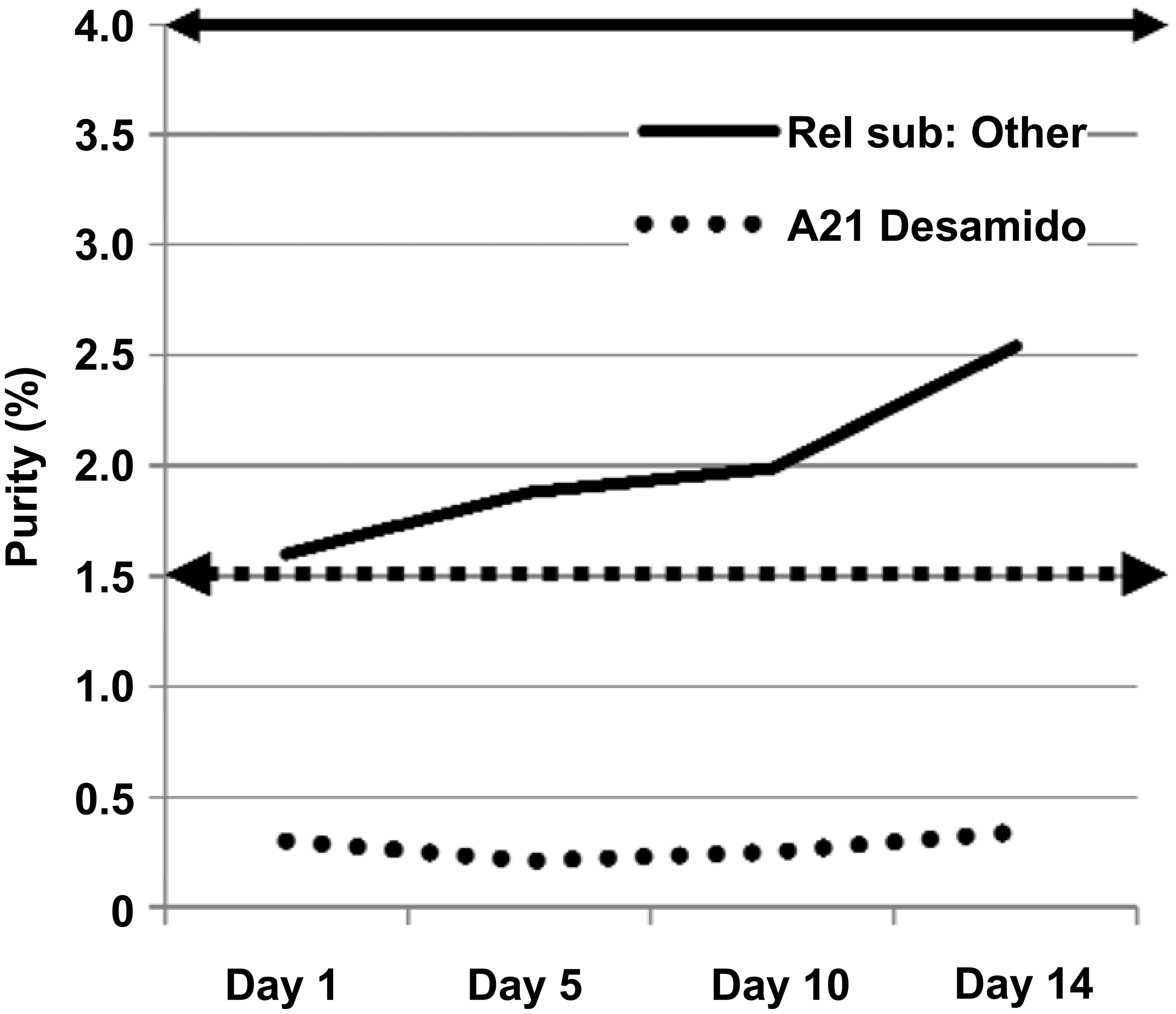
Purity (other related substances [solid line] and A-21 desamido [dotted line]) data for insulin lispro from dosed samples at four collection time points. Infusion sets were changed every 3 days in the WC study arm. Dosed WC samples were delivered under conditions of elevated temperature (37°C) and continuous agitation. The solid line with arrows shows the upper specification limit for other related substances (4.0%), and the lower dashed line with arrows shows the upper specification limit for A-21 desamido (1.5%).
Preservative content
Figure 4 shows m-cresol concentrations for the dosed WC samples at each collection time point, along with the baseline control (only taken at Day 1).
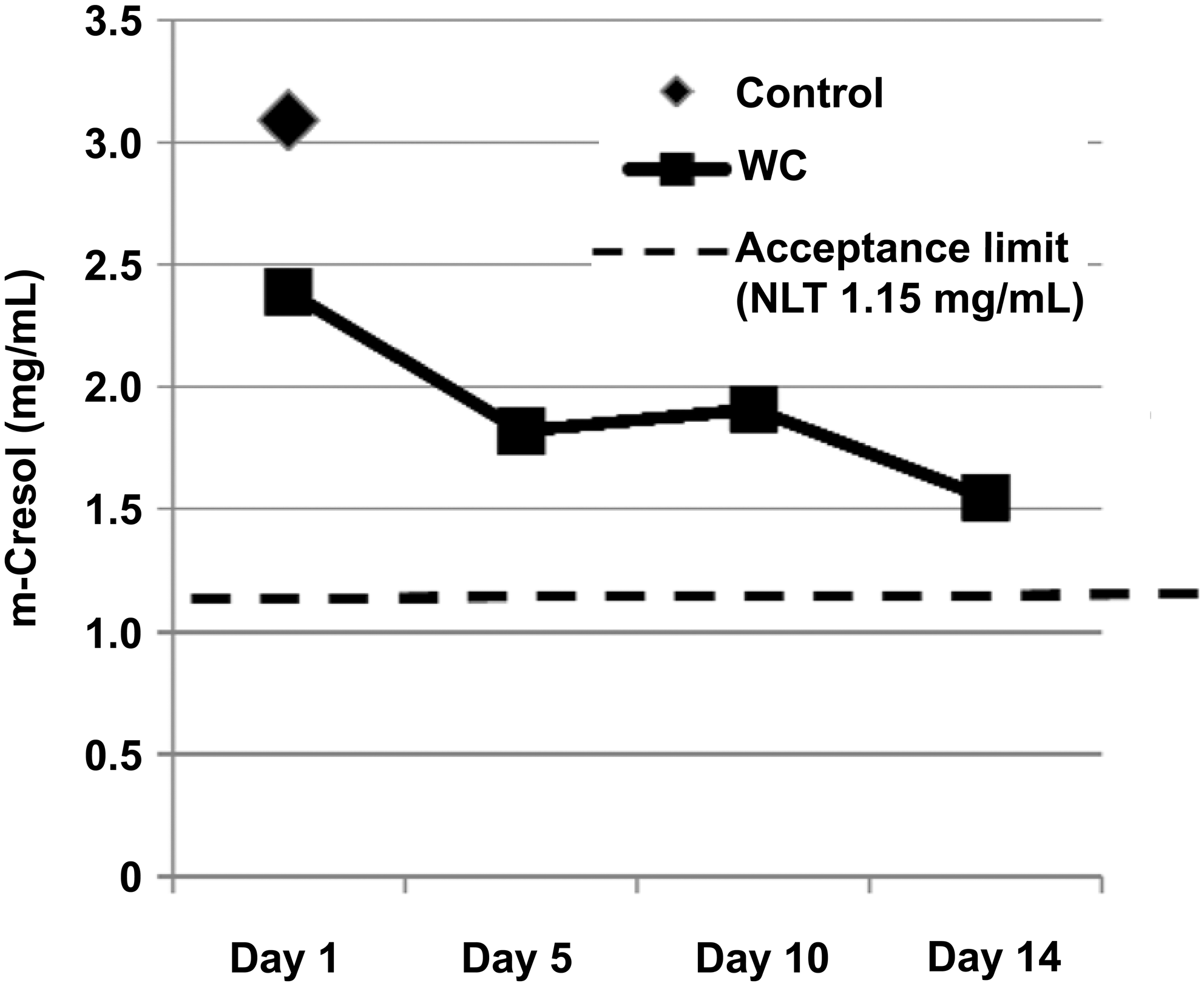
Concentration of m-cresol in insulin lispro from dosed samples at four collection time points and a baseline control sample stored at 5°C without agitation. Infusion sets were changed every 3 days in the WC study arm. Dosed WC samples were delivered under conditions of elevated temperature (37°C) and continuous agitation. The dashed line shows the minimum m-cresol concentration shown to meet the U.S. Pharmacopeia requirement for antimicrobial effectiveness (i.e., not less than [NLT] 1.15 mg/mL).
Accuracy of delivered volume
Pumping accuracy was determined by comparing the average daily delivered pumping volume from all pumps with the theoretically expected volume (percentage). Pump accuracy data from the WC study arm are presented in Figure 5.
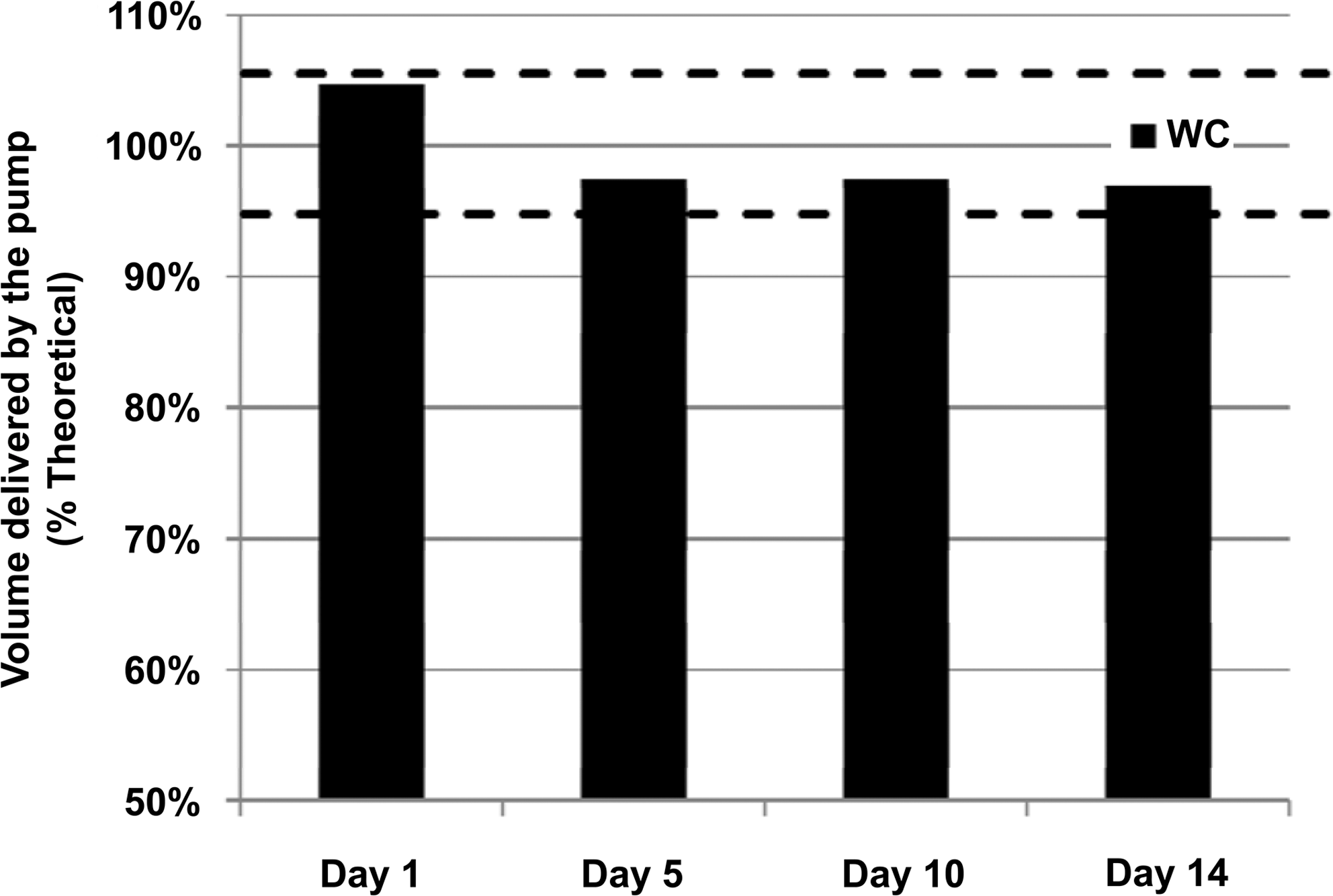
Percentage theoretical volume delivered for insulin lispro from dosed WC samples at four collection time points. Delivered volume at each collection time point was determined by gravimetric analysis and converted to a percentage theoretical value. Infusion sets were changed every 3 days in the WC study arm. Dosed WC samples were delivered under conditions of elevated temperature (37°C) and continuous agitation. The dashed lines show the upper and lower study limit, based on the manufacturer's claim of±5% for delivered volume accuracy.
Dosed samples without infusion set changes (NC)
The study of dosed samples without infusion set changes incorporated a study arm using conditions identical to those in the WC study arm, with the exception that infusion sets were not changed during the study, representing a worst-case scenario. Samples were collected at the same time points and subjected to the same analyses as the WC arm. At all time points, the levels of all attributes were maintained within the acceptance criteria and were very similar to those seen in the WC study arm (data not shown). In addition, there was no evidence of precipitation or occlusion alarms.
Reservoir samples
Reservoir samples were taken at Day 14 for both study arms (WC and NC). The levels of all stability attributes for reservoir samples from both study arms were maintained within the study acceptance criteria (data not shown). Samples were colorless and free of any precipitated material.
Discussion
This study examined the chemical and physical stability of insulin lispro in the Medtronic MiniMed Paradigm pump system under stressed conditions that mimic typical patient use over a period of 14 days. Analyses included assays to determine the impact of the stress conditions on the physicochemical properties of insulin lispro, including the potential for occlusion of the infusion set.
Changes in pH of insulin formulations may cause chemical degradation and/or precipitation, especially if the change is outside the pH specification limits. This could form an occlusion in the infusion set. In this study, the pH of insulin lispro increased only slightly and remained well within the acceptance criterion for pH of 7.0–7.8 for both study arms (WC and NC). Under these conditions, degradation due to changes in pH would not occur and would, therefore, not be expected to cause occlusion.
Insulin formulations may adsorb onto the surfaces of plastic reservoirs and infusion sets, resulting in reduced concentration and potency. 21 In addition, potential conformational changes resulting from this contact may produce aggregation that could initiate precipitation and occlusion. 16 Potency results at all time points from both study arms were comparable to the analytical control sample and well within the acceptance criterion of 95.0–105.0 U/mL.
Analyses of other related substance data for both study arms showed an increase in degradation over time. This increase was expected because of exposure to temperature and mechanical stresses; however, results remained well below the acceptance criterion of not more than 4% at all time points.
Insulin and rapid-acting insulin analogs are known to undergo deamidation of the asparagine residue at position 21 of the insulin A-chain (A-21 desamido). 16 Acidic conditions accelerate this deamidation process, but the deamidation is difficult to detect above pH 6. 16,22 No time-dependent trending was observed in either study arm, and the results were well below the acceptance criterion of 1.50%. These results are consistent with expectations because the A-21 desamido degradation product would not be expected to form in the pH ranges observed in this study.
Rapid-acting insulin analogs are subject to chemical degradation from factors such as increased temperature, mechanical stress, and extreme pH, which results in reduced activity and formation of high-molecular-weight polymerization products. 16 As expected, results from both study arms showed that there is an increase in percentage of HMWP at all study time points compared with the baseline control sample. However, HMWP remained below the 1.50% acceptance criterion.
The antimicrobial agent m-cresol is present in insulin lispro vials and cartridges at a level of 3.15 mg/mL. Concentrations of m-cresol for samples from both study arms decreased over time but were well above the qualification limit of 1.15 mg/mL at all time points, which provides protection against microbial contamination. Some m-cresol loss is presumably due to exposure to the plastic reservoir and infusion tubing, leading to adsorption and desorption. This has been reported in other studies that have shown absorptive loss of m-cresol when in contact with plastic such as CSII infusion sets 23 or syringes. 24 Accordingly, adsorptive and possibly desorptive loss observed in the infusion tubing would likely be related to residence time, which in turn is dependent on pumping rate.
Inaccurate delivered volume may be caused by pump failure, air bubbles, changes in viscosity of the insulin formulation, kinked or pinched infusion tubing, or other obstructions in liquid flow, such as insulin precipitation. The current volume accuracy results for both study arms met the acceptance criterion of±5% of the theoretical value at each study time point, indicating the lack of insulin lispro-related flow obstructions, even under stressed conditions with continual use of one infusion set.
The present study includes comprehensive stability-indicating data over an extended 14-day study period under conditions simulating patient use. Results indicate that insulin lispro has very good stability under these stressed conditions, with no indication of precipitation or line occlusions. To date, there are no other published reports showing other insulins having sufficient stability under these conditions for a period of 14 days.
Two cases of an apparent insulin lispro precipitation have been reported from patient use; however, only high pressure alarms were noted along with tubing discoloration, 25 and there were no chemical or physical testing data to confirm the presence of insulin precipitation. In addition, there were no significant differences in occlusions seen between groups in controlled clinical trials that compared insulin lispro with regular insulin 1,26 –29 and insulin lispro, insulin aspart, and regular insulin. 30 In addition, there were no significant differences seen between groups in an in vitro study 31 that compared insulin lispro with regular insulin, insulin aspart, or insulin glulisine. Taken together with this current 14-day in-use study outcome, there is now an abundance of data confirming the stability of insulin lispro under pump in-use conditions.
It is important to clarify the definition of an occlusion and to differentiate the cause of an alarm. Catheter/tubing occlusions in CSII therapy may be related to either the insulin or the device and can be caused by insulin precipitates, tubing kinks, or clots from blood or tissue. Alarms have commonly been referred to as occlusion alarms (or high pressure alarms), regardless of the nature of the blockage. An alarm caused by the insulin would be expected as a result of physical changes that cause a blockage. An alarm related to a device abnormality could be caused by inappropriate loading of the reservoir, a kink in the infusion tubing, an incorrectly inserted needle, or incorrect assembly of the device components. However, for clarity, we define an occlusion strictly as a clog caused by a physical obstruction within a line or other component of the pump device. It is significant that no alarms occurred during this 14-day study, even under the worst-case condition of no infusion set changes.
Limitations in the design of this study warrant discussion. These limitations include the use of a baseline control rather than a true (non-stressed) control, accuracy of delivery volumes in individual pumps, and the pooling of samples into a common daily sample for analysis.
Control samples
As described above, chemical testing results were compared with a baseline control sample that was obtained from the same batch of vials containing insulin lispro that was used to fill the reservoirs. The baseline control represents the condition of the material prior to exposure to the reservoir and stressed conditions mimicking in-use conditions. This baseline control sample accounts for all change incurred from patient use (e.g., the patient obtains a refrigerated vial and transfers material to a pump for use under stressed conditions). For clarity, a true control sample intended to specifically assess change resulting from the elevated temperature and shaking only would have evaluated the insulin from the pump in non-stressed conditions at all time points throughout the 14-day period. However, to understand the full range of change from a patient's perspective, we chose to use a baseline control rather than a true control.
Accuracy of delivered volume from individual pumps
Pumping accuracy criteria was partially based on the pump manufacturer's claim of±5% of the theoretical. The manufacturer conducts testing under conditions that are much more controlled than can be afforded under patient use (e.g., tightly controlled temperatures, no shaking, long pre-equilibrations, etc.). As a result, when conducting accuracy assessments for multiple pumps under patient use conditions, it is unlikely that the manufacturer's claim will be met for all individual pumps across all time points. Accordingly, Eli Lilly and Co. and the FDA jointly adopted an approach to apply the manufacturer's accuracy criteria to the daily average volume pumped across all pumps as opposed to each individual pump. Although daily averaged pump data met the intended pump accuracy criteria for both study arms, as expected, some of the individual pump data were not within 5% of theoretical (Table 1).
Pooled sample for analytical testing
As described in previously reported studies, individual daily samples were pooled into a common daily sample in order to provide sufficient volume for analytical testing. 14 –16 Testing results indicate that pooled samples readily passed all study criteria. However, because individual samples could not be tested owing to analytical limitations, the individual sample variability could not be determined.
These results demonstrate that insulin lispro formulation is both chemically and physically stable in vitro for 14 days in an external insulin pump system. The conditions used in this study would be unlikely in actual patient use, as insulin lispro is approved for 7-day use in the pump reservoir and patients are instructed to change their infusion set at least every 3 days and rotate their infusion site frequently.
Footnotes
Acknowledgments
This study was funded by Eli Lilly and Company, Indianapolis, IN. Thanks to Beth Baker for assisting in the setup and execution of the laboratory work, to Carlos Vargas for providing analytical support and consulting, and to Karen Boleyn for drafting the manuscript; all are employees of Eli Lilly and Company.
Author Disclosure Statement
All authors are full-time employees and shareholders of Eli Lilly and Company.