
Abstract
Objectives:
Hyperglycemia is a prominent feature among patients exposed to major stress such as in cardiac surgery. The implementation of a continuous glucose monitoring system (CGMS) for glucose monitoring during cardiac surgery was assessed.
Subjects and Methods:
Fifty-nine consecutive patients who underwent cardiac surgery were monitored by CGMS. Patients' fluid glucose content, drug requirements, and hemodynamic and physiologic parameters were evaluated.
Results:
Of the 59 patients, 32 completed the monitoring with CGMS. Patients were divided into three groups: diabetes patients, patients without diabetes history who developed significant hyperglycemia perioperatively, and patients who did not develop hyperglycemia. Hyperglycemia was most frequently observed postoperatively. Hyperglycemic patients required significantly more insulin (81±40 vs. 34±37 units, P=0.005) and experienced an increased early complication rate, although this difference was not significant. CGMS erroneously detected late-phase operative and immediate postoperative hypoglycemia in approximately one-third of patients as reflected from venous blood sample measurements.
Conclusions:
CGMS enables close monitoring and optimal control of blood glucose among patients undergoing major cardiac surgery, although its reliability is limited during the cardiac surgery phase and in the early postoperative period, because of incorrect hypoglycemic readings.
Introduction
Patients undergoing cardiac surgery are exposed to stress and acute physiological changes from multiple sources, including the surgical procedure itself, drugs and blood products, extracorporeal circulation, and hypothermia. 10 Coronary artery bypass graft (CABG) surgeries are common in T2DM patients. In these patients, elevated hemoglobin A1c levels are associated with increased length of hospital stay, morbidity, and mortality. 11
Hyperglycemia is a prominent feature in patients both with and without diabetes exposed to major stress such as surgery and trauma and is associated with increased morbidity and mortality rates. 12,13 Hyperglycemia during and after surgery is influenced by various factors, including type of anesthesia, glucose load, exogenous insulin administration, and core temperature. 14 –18 Hyperglycemia in a hospitalized patient, for any reason, is an independent risk factor for morbidity and mortality, 12 whereas hyperglycemic patients with no known diabetes may represent a subgroup with a poor prognosis. 19 This underscores the importance of continuous and intensive blood glucose monitoring in patients undergoing major surgery. Continuous glucose monitoring is a promising tool to assist glucose control, but the accuracy and reliability of these devices in critically ill patients are uncertain. 20,21
The aim of this study was to examine and monitor glycemic response in patients undergoing cardiac surgery during the perioperative period, using 24-h monitoring with a continuous glucose monitoring system (CGMS) and evaluating its accuracy and reliability.
Subjects and Methods
Study subjects were a nonselected convenience sample of patients admitted to the cardiac surgery department at our institute during a 4-month period. This means that the participants were not selected from the target population using a probability sample; rather, patients who happened to be undergoing the stated procedures were selected if they agreed to participate. After signing an informed consent form, subjects were connected to the CGMS preoperatively.
The CGMS (CGMS® System Gold™ with Sof-sensor®) is an input, Holter-like device, manufactured by MiniMed (Northridge, CA). A small sensor containing glucose oxidase is inserted subcutaneously via a needle, and the data are collected in a small device attached to the sensor through a cable. Glucose values are collected in 5-min intervals, amounting to 288 values per day. The continuous glucose monitoring was blinded, and the data were not available to the department staff.
Blood glucose levels were measured during and after the operation from plasma blood samples drawn intravenously, in the preoperative phase every hour for 2 h, in the operative phase every hour, and in the postoperative phase every 2 h for 12–24 h, in order to enable calibration and comparison between blood glucose levels and CGMS values. Blood glucose was measured with a Stat Profile® 5 machine (Nova Biochemical, Waltham, MA).
The fluids that were given to the patients during the operation included mostly glucose-free fluids except the cardioplegia solutions, which contained 5 g of glucose/L. Glucose-rich solutions were used liberally only postoperatively.
Fluid types and quantities were similar in patients both with and without diabetes (Table 1).
Characteristics of patients with hyperglycemia did not differ from those of patients with normoglycemia.
T2DM, type 2 diabetes mellitus.
Once the patient was connected to the CGMS, a comprehensive data collection took place, including hemodynamic and biochemical parameters during and after the operation, drug requirements, body temperature, and continuous electrocardiogram monitoring. A day after the operation the CGMS was disconnected, and the data were transferred to a PC.
Data analysis
Analysis of data was carried out using SPSS version 9.0 statistical analysis software (SPSS Inc., Chicago, IL). Continuous variables, such as age, glucose, heart rate, and body temperature, were reported as mean±SD values. Categorical variables, such as the presence or absence of specific postoperative complications or comorbidities, were described using frequency distributions. Repeated-measures general linear modeling was used to detect differences in the means of blood glucose by method as within-subject factors, and diabetes (yes/no) was used as the between-subjects factor. Post hoc analysis of blood glucose was assessed using the t test for paired samples. At each time point, each method of blood glucose measurement was compared by diabetes using the t test. The χ 2 test was used to detect differences in categorical variables by time. All tests are two-tailed and considered significant at P<0.05.
Results
Fifty-nine cardiac surgery patients were enrolled in the study. In 27 patients, an early failure of CGMS failure precluded data collection, leaving 32 subjects (84% men; 34 operations) connected to the CGMS, for analysis (Table 1). In the majority of the cases the failure occurred because of technical dislocation of the sensor during the phase of transporting the patients to or from the operation room.
Nine patients (28%) of the 32 subjects were known to have T2DM; seven patients (22%) who developed significant hyperglycemia during and after the operation were not known to have diabetes. Significant hyperglycemia was defined as blood glucose of ≥250 mg%. The rest were normoglycemic during the follow-up. Seven of the diabetes patients were treated with oral hypoglycemic medication, and two were treated with diet only.
The majority of patients (50%) had triple-vessel disease, and an additional 29% had double-vessel disease. Mean left ventricular ejection fraction was 52% (Table 1). Background medical illnesses, smoking status, and drug usage did not differ significantly between patients with and without diabetes.
Twenty-nine patients were operated for CABG, and three more underwent operations to excise a myxoma of the left atrium, repair an atrial septal defect, and for aortic valve replacement. Two patients needed CABG combined with mitral valve replacement, aortic valve replacement, and excising of a left ventricle aneurysm. Another two patients needed immediate re-operation due to postoperative bleeding and ischemia. Both re-operations were successful. All patients were operated on using extracorporeal circulation and patient-induced hypothermia. Mean trough temperature during the operation was 32±3.5°C.
Extracorporeal circulation time averaged 1 h 43 min. All patients were anesthetized using a moderate dose of opioid anesthesia (fentanyl dose, 30–50 μg/kg). All patients were discharged without any early mortality.
The glucose load was similar in patients with and without diabetes during both the operation. In the first postoperative day, diabetes patients required more insulin compared with hyperglycemic patients without diabetes (Table 1).
Mean perioperative venous blood glucose levels were elevated in diabetes patients compared with those without diabetes; these differences were statistically significant at the first stage of the operation and postoperatively despite exogenous insulin given according to blood glucose levels during follow-up. CGMS readings detected significantly different blood glucose levels between patients with and without diabetes postoperatively only (Table 2).
Pre-bypass represents the time during the operation between induction of anesthesia and bypass, bypass represents the time during operation that cardiopulmonary bypass was carried out, post-bypass represents the time during operation between cessation of bypass and the end of operation, and postoperative represents the postoperative period (duration of 24 h). Blood represents blood samples drawn intravenously and monitored with the Stat Profile 5 machine, and sensor represents glucose values as monitored with a continuous glucose monitoring system.
HG, significant hyperglycemia with no known diabetes; NG, normoglycemic results and no history of diabetes; T2DM, type 2 diabetes mellitus.
During the operation, all patients experienced a mild increase in glucose levels. Before cardiopulmonary bypass activation, glucose level changes were minimal. During the bypass, there was a mild increase in glucose levels with essentially no difference between patients with and without diabetes. Only at the last stage of the operation and postoperatively, while the patients were re-warmed, a marked increase in glucose levels was measured. When comparing between blood and CGMS readings, among patients both with and without diabetes, differences were nonsignificant during the operation and gained significance postoperatively (Table 2).
Overall, there was a good correlation between blood samples and CGMS readings with a moderate increase in glucose levels during and after the operation (Fig. 1) except at the final stages of the operation due to the split phenomenon. This phenomenon did not differ by diabetes status (22% in those with diabetes, 31% in those without diabetes, P=0.6), body temperature (31.6±1.5°C in subjects with split vs. 32±4.1°C in those without split, P=0.8), intraoperative drugs (26.9% in those with vs. 25% in those without fentanyl, P=0.9), or lactate levels (3.1±0.9 mmol/L in those with vs. 2.7±1.1 mmol/L in those without, P=0.6). In the perioperative phase the mean absolute relative difference (MARD) was 19.2% versus 13.3% in the postoperative phase.

Comparison between mean blood glucose readings measured by the continuous glucose monitoring system (CGMS) and blood samples.
A “split curve” describes a mismatch between the CGMS glucose readings compared with venous blood values. This phenomenon was evident at the final stages of the operation and shortly after, as the CGMS documented a glucose drop to hypoglycemic levels whereas much higher, actual blood glucose values were obtained from venous samples at the same time (Fig. 2). This phenomenon was noted among 10 patients (31%), six of whom had diabetes or developed hyperglycemia, and four were normoglycemic patients. This gap between the readings developed in the post-bypass stage of the operation and was maintained for a few hours postoperatively before the curves reconverged (Fig. 3).
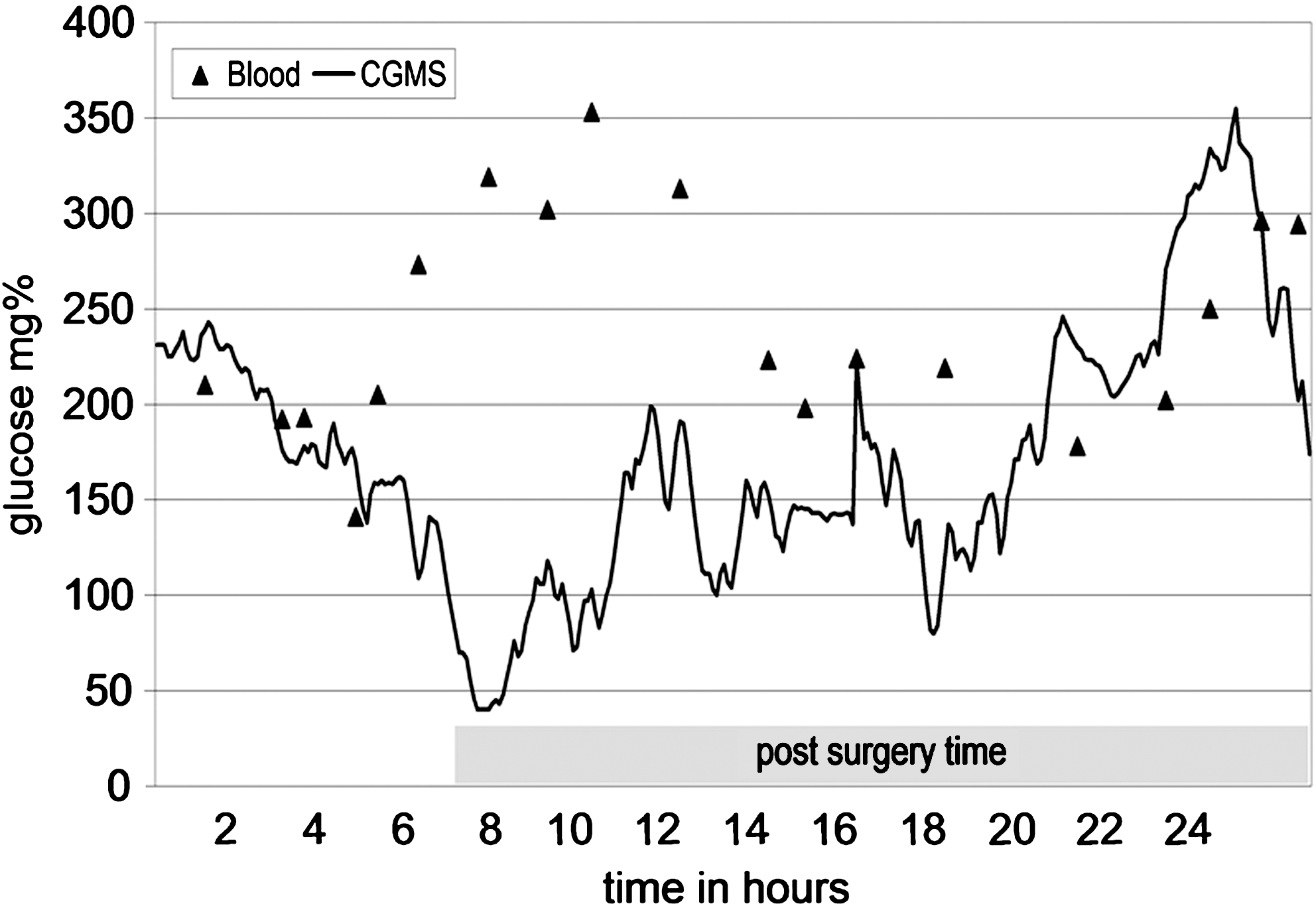
The “split” phenomenon between continuous glucose monitoring system (CGMS) and blood glucose levels.
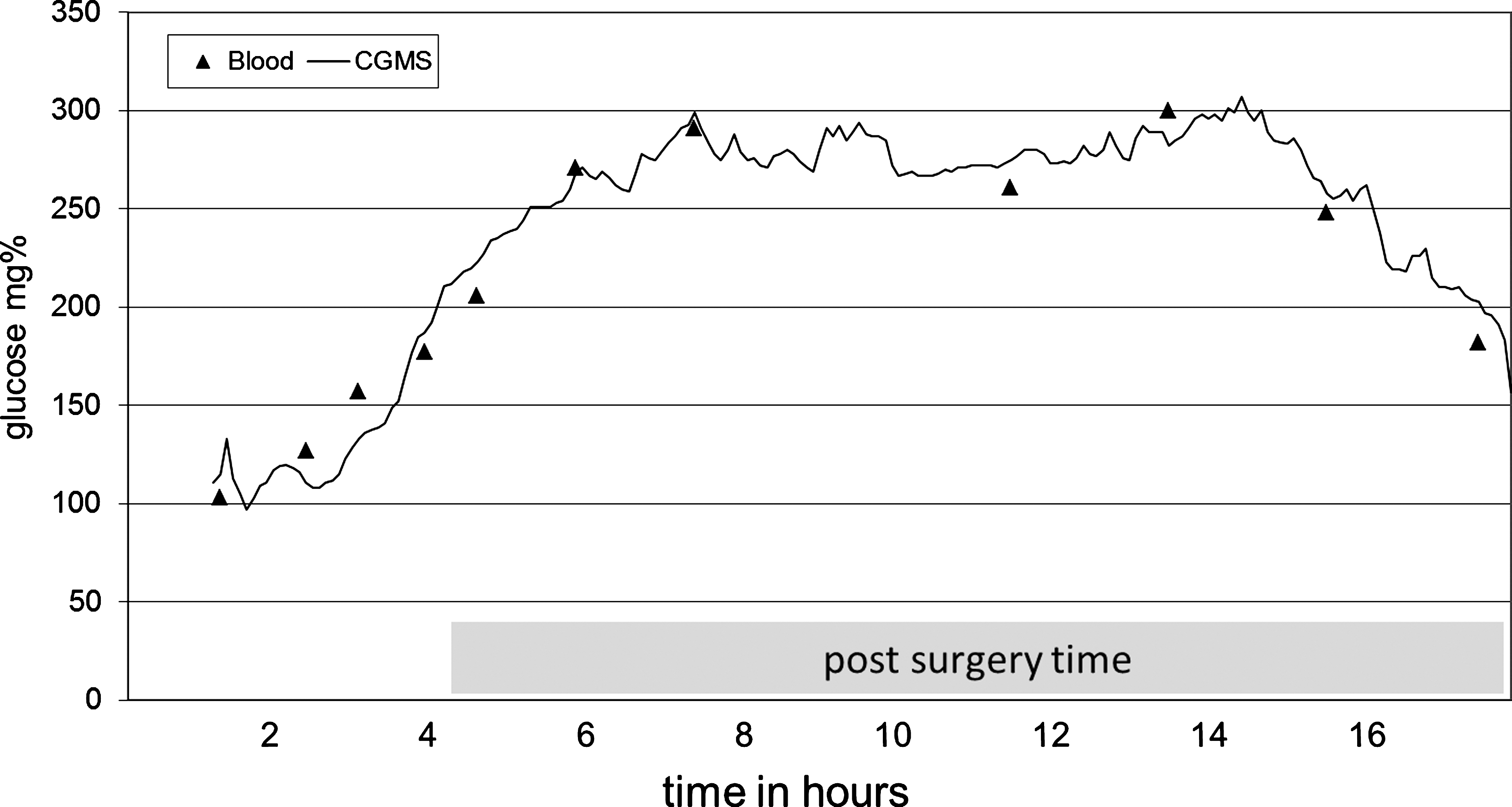
Correlation between continuous glucose monitoring system (CGMS) and blood glucose values.
Complications developed in 11 patients (34%), two requiring immediate re-operation due to bleeding and ischemia. The complication rate among the diabetes patients was 44%, in the hyperglycemic patients was 42%, and in the normoglycemic patients was 29%, although these differences were not significant. Overall, the most prevalent complication was cardiac arrhythmia (ventricular tachycardia or paroxysmal atrial tachycardia), which developed among two-thirds of the patients postoperatively, but with no clinical significance or need for intervention. Ventricular fibrillation developed in one patient postoperatively because of cardiac ischemia, and emergency re-operation was successful. Pulmonary complications developed in three patients, which included acute respiratory failure and accumulation of pleural fluid. Other complications included acute renal failure, which developed in three patients, mediastinitis in two, and quadriplegia in one patient (related to a prior, severe orthopedic problem).
Discussion
In the present study, patient candidates for CABG were divided into three groups according to their glycemic status: known diabetes patients, patients who developed pronounced hyperglycemia with no history of diabetes, and normoglycemic patients. It is not clear whether the second group represented stress hyperglycemia or undiagnosed diabetes.
Intraoperative hyperglycemia developed less frequently in our study population than reported in the literature. 16,17,22 This may be due to the intraoperative glucose dose used at our institute (4 g), which is lower than the dose used by others (10–100 g). Glucose dose may play a crucial role in glycemic control during a major operation. Indeed, even the diabetes patients did not develop hyperglycemia during the operation when given glucose-free solutions. A moderate rise in glucose levels did occur, but marked hyperglycemia developed only postoperatively. This rise was observed in patients both with and without diabetes, whereas half of the patients remained normoglycemic.
The type of anesthesia that was used (moderate opioid anesthesia) also contributed to the suppression of the glycemic reaction. 14,23 –28 Other parameters, such as the degree of hypothermia, intraoperative drugs, etc., that might influence glycemia did not differ between the groups.
Another important observation was the hypoglycemia recorded by the CGMS compared with the higher readings measured from venous plasma blood sampling. This phenomenon developed during the last part of the operation, when the patient was on bypass and was hypothermic to some degree. It has been reported that the combination of cardiopulmonary bypass and hypothermia is devastating to hormonal homeostasis (catecholamine, insulin, etc.) and to the hemodynamic status of the patient. 22 This phenomenon, known as “split curves,” was found to be independent of the diabetes status, degree of hypothermia of the patient, intraoperative drugs, and lactate levels. It is possible that this phenomenon is related to the decrease in glucose levels in the interstitial compartment due to extreme vasoconstriction. Technical failure of CGMS is a less likely explanation because CGMS readings were again correlated to venous blood values a few hours later, suggesting cardiovascular recovery over time.
Another surprising observation was the stronger correlation between CGMS and venous blood sample values among patients with diabetes compared with those without diabetes. This finding may reflect vascular autoregulation impairment among the diabetes patients attenuating the previously mentioned extreme vasoconstriction.
Postoperatively, marked hyperglycemia developed among half of the patients, only half of whom had known diabetes. Those patients were treated with intravenous insulin and strict blood glucose surveillance according to the department protocol (hourly blood sampling); nevertheless, optimal glycemic control was not achieved. The hyperglycemic group (whether known diabetes patients or not) demonstrated a higher complication rate, including two local wound infections. Although the difference did not reach statistical significance in this study, other publications support the view that acute stress hyperglycemia is an independent risk factor for morbidity and mortality, 13,29 –31 and more aggressive glucose control in the postoperative period seems to be a crucial step in lowering morbidity. 13,29 –32
Several authors have reported that diabetes and postoperative hyperglycemia are associated with the development of surgical site infections. 29 –31 Glucose control is also associated with reduced short- and long-term mortality rates. 13 The central question of whether tight control of glucose levels is a major determinant of outcome was also addressed 13 in a prospective study among 1,548 patients admitted to the intensive care unit (the majority after cardiac surgery). Mortality was significantly lower among patients treated to maintain lower glucose levels, during the intensive care unit stay (40%) and in the long term.
Anesthesia type is another factor influencing blood glucose levels. Deep opioid anesthesia given to critically ill neonates undergoing cardiac surgery attenuated the stress response, improved insulin response, and lowered mortality and morbidity. 14 Hyperglycemia was prevented by epidural anesthesia and attenuated by fentanyl/midazolam anesthesia but was not affected by inhaled anesthetics. 23 Earlier articles relating to the effect of type of anesthesia on the glycemic response support these findings. 24 –28
Compared with patients who did not receive glucose-containing solutions, patients without diabetes given cardioplegia solutions were shown to develop marked hyperglycemia during hypothermia, returning to normal only after rewarming. 16,33 Patients given insulin-containing solutions have been shown to exhibit better recovery, 17,34 but this has been not consistently reported, 35,36 and hypoglycemia can be a problem. 37
In conclusion, glucose management in intensive care units is a crucial issue, and CGMS has the potential to improve efficient management. Previous reports have shown that CGMS accuracy was not sufficiently in critical ill patients, 38 –40 although other reports demonstrate a good enough reliability. 41
In addition to these reports, our study documents glycemic alterations during cardiac surgery and supports the importance of continuous glucose monitoring during and after a major operation. CGMS with a 5-min reading interval can be an effective means of surveillance for surgical patients, but it is not reliable during the end of the operation and in the early postoperative period. In order to examine definitively the reliability and accuracy of CGMS a large-scale study is needed to further clarify these issues.
Footnotes
Author Disclosure Statement
No competing financial interests exist.