
Abstract
Background:
None of the studies concerned with the performance of a continuous glucose monitor (CGM) over time has examined the extent to which extended periods of wear affect the responses of both CGM accuracy and lag time to rapid changes in blood glucose levels. Here we propose a novel approach to address these issues.
Methods:
Eight participants without diabetes were each fitted with two CGMs (Paradigm® 722 Real-Time [Medtronic, Northridge, CA]; abdominal and triceps regions) and completed fasted oral glucose challenges (OGCs) on six occasions over a 9-day period, while the CGMs were worn without removal. Arterialized blood samples were collected for comparison with CGM values.
Results:
There were marked mismatches and lag times between blood glucose and CGM values in response to all OGCs, most notably during the initial rapid increase in glucose levels. Abdominal and triceps CGMs consistently underestimated peak blood glucose by an average of 2.7±0.2 and 2.9±0.2 mM, respectively, and were associated with a peak blood glucose lag of 21.6±1.8 and 18.1±1.6 min, respectively. CGM accuracy did not deteriorate over 9 days of wear in OGCs for either the abdominal or triceps sensor. All participants found the triceps sensor site more comfortable than the abdominal site (P<0.05).
Conclusions:
The current CGM sensor tested here may be used for extended periods, providing added economic benefits for the wearer. However, the marked inaccuracy and lag time of CGM readings when blood glucose levels change rapidly within the physiological range must be considered for optimal CGM use in glycemic management.
Introduction
Prolonged wearing of CGMs raises the issue of whether the performance of their sensors remains stable over their periods of use. Although most but not all 5 studies suggest that sensor performance remains relatively stable over 3, 6 –9 5, 10 –12 6, 13 7, 14 or 1015 days, many of these studies did not support their findings with any statistical analyses, 5,7,8,10,13,14 and several important accuracy issues were not addressed. For instance, it remains to be established whether several days of wear affect sensor accuracy under conditions of rapid changes in blood glucose levels. This is an important issue because rapid changes in blood glucose concentrations are associated with greater mismatches between blood glucose and CGM values compared with periods of stable blood glucose levels. 10,16 –19 Another limitation is that none of these studies adopted a matched paired study design between consecutive days to account for such events as meals, insulin, or activity regimens on consecutive days despite these factors likely causing increased variability between blood glucose and CGM values between testing days. This is even more problematic if exposure to low blood glucose levels 9,20 and to rapid changes in blood glucose concentrations varies between testing days because these factors contribute to greater mismatches between blood glucose and CGM values. 10,16 –19 It has also been overlooked that sensor accuracy over time might have been overestimated because of a decrease in glycemic variability during the observation period. Indeed, glycemic variability has been shown to decrease over time of CGM use, 21 thus raising the possibility that the reported absence of deterioration in the mismatch between CGM values and blood glucose levels with prolonged CGM use might in some cases reflect a decrease in glycemic variability rather than the maintenance of stable sensor accuracy per se. Finally, no study has measured the effects of sensor wear on lag time between CGM readings and actual blood glucose levels. This latter limitation is an important one considering that a prolonged lag can result in marked inaccuracies between CGM readings and actual glucose levels. 10,16 –18
In order to test the effect of duration of wear on the lag time and accuracy of CGM exposed to rapid changes in blood glucose levels without the confounding effect of falling glycemic variability with time of wear, it is important for a CGM to be subjected to reproducible changes in blood glucose levels over several consecutive days. This is a highly challenging task given the marked variability in blood glucose levels in individuals with diabetes. One labor-intensive and expensive approach to achieve this would be to subject these individuals to a glucose clamp, allowing reproducible changes in blood glucose levels to be generated over consecutive days. Alternatively, because the pattern of response to an oral glucose challenge (OGC) is not expected to differ markedly between testing days in individuals without diabetes, this raises the possibility that CGM performance could be tested in individuals without diabetes exposed on consecutive days to an OGC. Although this experimental approach does not allow one to evaluate the performance of CGM over both the hypoglycemic and hyperglycemic ranges, it does allow the assessment of the response of CGM to reproducible physiological changes in blood glucose levels considered to be within the target concentration range for optimal diabetes management. Using such a novel and simple approach, the purpose of this study was to evaluate the effect of wearing a CGM for 9 days on the accuracy and lag time of CGM responses to physiological changes in blood glucose levels. Given that prolonged wear raises the issue of comfort, this study also assessed comfort responses to sensor site of insertion. This study is important because the possible demonstration that prolonged sensor wear does not affect the accuracy of CGM has the potential of reducing the daily cost of CGM use without compromising performance.
Subjects and Methods
Participants
Eight healthy individuals without diabetes (seven women and one man; age, 31.3±7.1 years; body mass index, 24.6±2.6 kg/m2; mean±SD) were recruited to this study. Each participant received a detailed description of all experimental procedures prior to providing written consent. This study was approved by the University of Western Australia's Human Research Ethics committee.
At 17:30 h on the day prior to the first OGC, each participant was fitted with two Paradigm® 722 Real-Time CGMs (Medtronic, Northridge, CA) in accordance with the manufacturer's guidelines. One sensor was inserted in the region of the abdominal wall 5 cm lateral to the navel, and another one on the contralateral rear upper third of the nondominant arm (triceps). For the duration of the study, participants calibrated both abdominal and triceps CGMs simultaneously four times daily using a validated blood glucose meter (Accu-chek® Performa, Roche Diagnostics, Indianapolis, IN). On each day prior to the laboratory trials, participants were asked to abstain from alcohol and caffeine and were asked to replicate the evening meals prior to the laboratory trials. No food was allowed from 22:00 h until after the testing session the following day.
Data collection
The morning after the CGMs were fitted and after an overnight fast, participants were required to calibrate both their CGMs at 07:00 h before arriving in the laboratory at 08:00 h for an OGC (day 1 of testing). After a blood sample was taken to measure fasting blood glucose levels, participants consumed a 20% (wt/vol) glucose solution providing 1 g of glucose/kg of body weight (Glucodin™, Boots Healthcare, North Ryde, Australia). Blood samples were taken every 15 min for the next 2 h to compare blood glucose levels with both abdominal and triceps CGM values. Each blood sample was collected from arterialized venous blood into a 35-μL capillary tube obtained from the fingertip of the hand prewarmed in a 43°C water bath, and glucose was then analyzed (ABL700 series, Radiometer, Copenhagen, Denmark). This OGC trial was repeated in the same manner on days 2, 3, 5, 7, and 9 for a total of six testing sessions. The sensors were removed after the final trial, and CGM data were uploaded using Carelink™ software version 3.0A (Medtronic) for analysis.
Statistical analyses
Analyses were carried out using Prism® (GraphPad, San Diego) version 5 software. Level of statistical significance was set at P<0.05. One- and two-way repeated-measures analyses of variance with Bonferroni's post hoc tests were adopted to compare variations between blood glucose levels and CGM values over the trial days. The variables analyzed to examine sensor accuracy and lag time are described in Figure 1 and included mismatch between area under the curve (AUC) values, mismatch at peak blood glucose level, mismatch between blood glucose peak and CGM peak, difference between time to peak glucose levels, and difference between the rate of glucose increase (0–15 min). Paired t tests compared differences between CGM sensor sites (abdominal versus triceps) during individual trial days. A χ2 analysis compared the observed and expected frequencies of site preference.
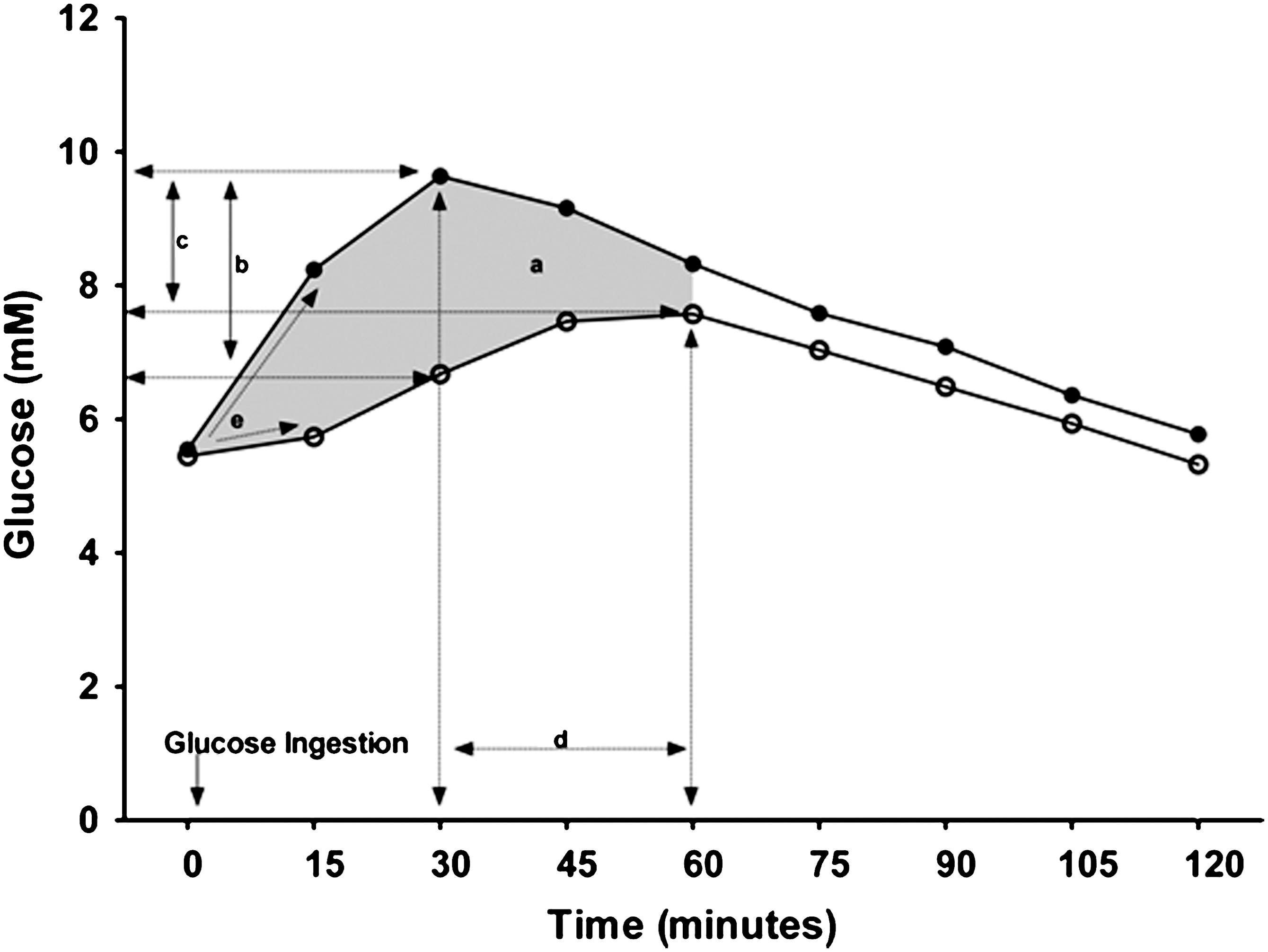
Graphical description of the analyses used in accuracy and lag assessment: shaded area a, mismatch between area under the curve calculated between blood glucose and continuous glucose monitor values (0–60 min); line segment b, mismatch between maximum blood glucose and continuous glucose monitor value at the same time point; line segment c, mismatch between peak blood glucose and peak continuous glucose monitor values; line segment d, difference between time to peak blood glucose and peak continuous glucose monitor values; and line segment e, difference in rate increase between blood glucose and continuous glucose monitor values.
Results
Effect of repeated OGC tests on the patterns of change in blood glucose levels
Baseline blood glucose levels and the patterns of change in blood glucose level in response to OGC did not differ between testing days, with blood glucose levels during the OGC not being different irrespective of the days compared (P=0.47). Each day, there was also no difference between baseline blood glucose levels and pre-OGC CGM values (P=0.98). In response to the OGC, blood glucose levels of all participants and across all treatments returned to baseline within 120 min, with no difference from pre-OGC values (P=0.99; Fig. 2). Across all OGCs, there were statistically significant mismatches between blood glucose and CGM values, most notably during the first 30 min when blood glucose levels increased rapidly (all P<0.05, Fig. 2). There was no difference between abdominal and triceps CGM sensor values during the trials on days 1, 2, 3, 5, and 7. However, on day 9, CGM readings obtained from the triceps sensor were lower than those obtained from the abdominal sensor throughout the glucose challenge (P=0.01).
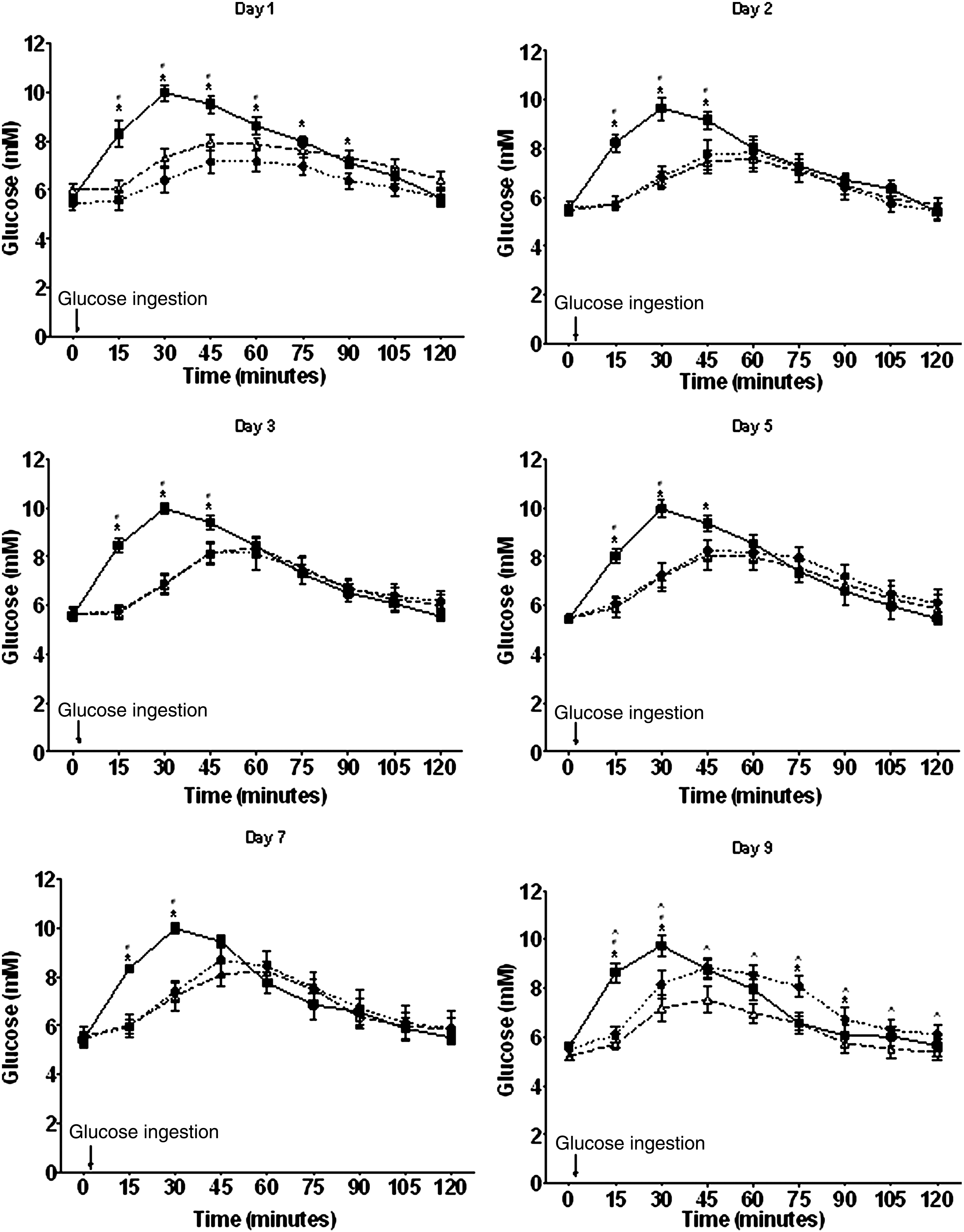
Patterns of change in reference blood glucose levels (squares), continuous glucose monitor abdominal glucose values (circles), and continuous glucose monitor triceps glucose values (triangles) after glucose ingestion. Statistically significant differences (P<0.05) are indicated between *blood glucose levels and abdominal continuous glucose monitor values, #blood glucose levels and triceps continuous glucose monitor values, and ^abdominal continuous glucose monitor values and triceps continuous glucose monitor values.
AUC
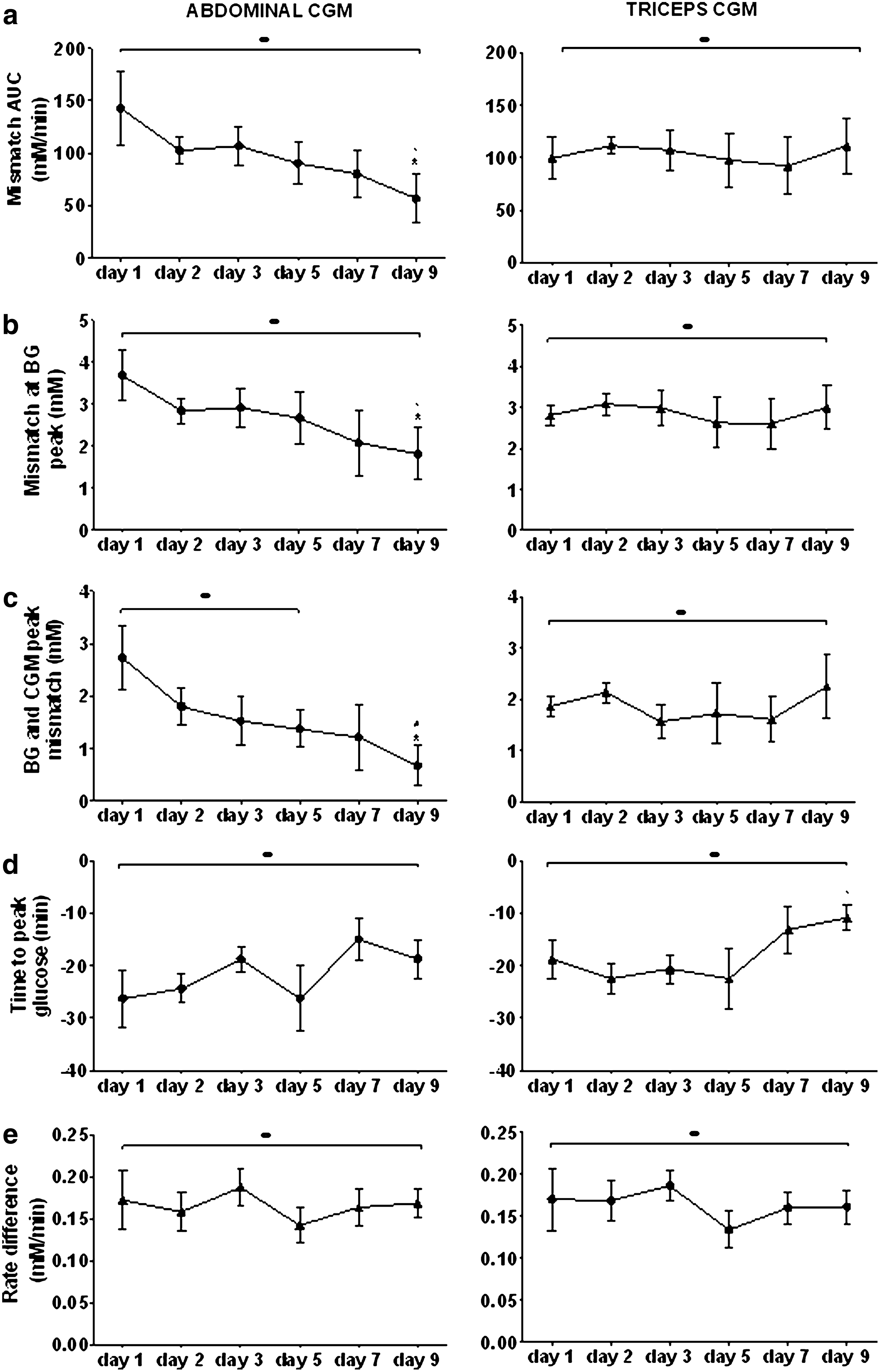
The glucose×time AUC was calculated from the glucose response to the OGC between 0 and 60 min post-glucose ingestion (Fig. 3a), with the AUCs for both abdominal and triceps CGMs being lower than blood glucose AUC on each testing day (P<0.01). The mismatch between both abdominal (P=0.5) and triceps (P=0.3) AUC compared with reference blood glucose did not differ between days 1 and 2. The triceps AUC did not differ between consecutive OGC trials (P=0.83). However, over time, the abdominal AUC trended to more closely match the reference AUC (reference – abdominal: day 1=142.8±35.3 mM −1/60 min vs. day 9=56.9±23.3 mM −1/60 min; P=0.065) and on day 9 was less than the triceps AUC difference to reference blood glucose AUC (56.9±23.3 mM −1/60 min vs. 111.4±26.5 mM −1/60 min; P<0.01).
Effect of time of wear on mismatches between blood glucose (BG) levels and continuous glucose monitor (CGM) abdominal values (
Mismatch at peak blood glucose
When blood glucose reached peak levels in response to OGC, both abdominal (P<0.01) and triceps (P<0.01) CGM readings underestimated peak blood glucose by an average of 2.7±0.2 and 2.9±0.2 mM, respectively (average of all days; Fig. 3b). There was no difference in the mismatch between days 1 and 2 for both the abdominal (3.7±0.6 mM vs. 2.9±0.3 mM, respectively; P=0.23) and the triceps (2.8±0.2 mM vs. 3.1±0.3 mM, respectively; P=0.41) CGMs. There was a trend for the magnitude of the abdominal CGM mismatch to decrease with time (abdominal day 1=3.7±0.6 mM vs. day 9=1.8±0.6 mM; P=0.098) but not for the triceps CGM mismatch (triceps day 1=2.8±0.2 mM vs. day 9=3.0±0.5 mM; P=0.76). CGM values did not differ between sites with the exception of day 9 when the mismatch of peak abdominal CGM readings was less than that of the triceps CGM mismatch (1.8±0.6 mM vs. 3.0±0.5 mM; P<0.01).
Mismatch between blood glucose peak and CGM peak
In response to the OGC, abdominal and triceps CGM peak glucose readings were lower than peak blood glucose levels on all days except for day 9 when peak abdominal CGM readings more closely matched reference peak glucose (P=0.12) and were higher than triceps CGM peak glucose (P<0.01; Fig. 3c; reference=10.0±0.3 mM vs. abdominal=9.4±0.3 mM vs. triceps=7.8±0.5 mM). There was no difference between the mismatch between reference and abdominal CGM peak glucose readings between day 1 and 2 (2.7±0.6 mM vs. 1.8±0.3 mM; P=0.13); however, the abdominal CGM mismatch to reference glucose readings decreased over time (day 1=2.7±0.6 mM vs. day 9=0.7±0.4 mM; P=0.04). There was no difference between the reference glucose readings and triceps CGM peak glucose mismatch between days 1 and 2 (1.9±0.2 mM vs. 2.1±0.2 mM; P=0.14) or over time (day 1=1.9±0.2 mM vs. day 9=2.3±0.6 mM; P=0.56).
Time to peak glucose levels
The time to achieve peak CGM glucose readings was slower for both the abdominal and triceps sensors in comparison with the time to reach peak reference blood glucose level on all trial days (Fig. 3d). There was no difference in the time between reference and abdominal CGM peak glucose readings (P=0.8) and between reference and triceps CGM peak glucose readings (P=0.2) between days 1 and 2 as well as over all trial days (P=0.3 [abdominal], P=0.2 [triceps]). However, the lag time to triceps peak CGM glucose readings trended to decrease over the trial period (day 1=18.8±3.8 min vs. day 9=10.9±2.4 min; P=0.085), whereas there was no difference in the average lag time for the abdominal CGM (day 1=26.3±5.5 min vs. day 9=18.8±3.8 min; P=0.35).
Rate of glucose increase
The initial rate of increase in glucose levels measured by the CGM for the first 15 min of the OGC (Fig. 3e) was slower for both the abdominal (0.02±0.00 mM/min−1; P<0.01) and triceps (0.02±0.01 mM/min−1; P<0.01) sites compared with actual blood glucose (0.19±0.01 mM/min−1) on each trial day (average values for all trial days), and neither improved (or more closely matched the rate of increase of blood glucose) over the 9 days.
CGM site preference
Based on a written questionnaire, all participants (eight out of eight) preferred wearing the CGM on the triceps region in comparison with the abdominal region (P=0.005). Discomfort at the abdominal region was primarily due to the transmitter rubbing against the waistline of the clothing, especially while seated. No infection, pain, or bleeding was reported.
Discussion
The capacity of CGMs to improve glycemic control, reduce the duration of hypoglycemia, and encourage patients' adherence to treatment depends on the accuracy of their readings and their cost of use. This is the first study to show that despite statistically significant mismatches between blood glucose levels and CGM readings, CGM accuracy and lag time associated with rapid physiological changes in blood glucose levels do not deteriorate over 9 days of continuous use. We also show a clear preference for sensor wear on the triceps rather than the conventional abdominal site. Although our findings have implications for the user in terms of the cost-effectiveness of single-use sensors, the marked inaccuracy and lag time of the CGM during rapid changes in blood glucose levels must be considered for optimal CGM use in glycemic management.
Although most studies have reported that sensor performance does not deteriorate markedly as a function of time, 5 –15 their findings were not conclusive. As mentioned earlier, this is because none of these studies matched testing conditions between consecutive days, examined lag time, and addressed CGM performance in response to rapid changes in blood glucose levels, 5 –15 and all of these studies overlooked the potential confounding effect of the decrease in blood glucose variability with CGM time of wear. 21 In contrast, these limitations were overcome in this study by exposing the unit on consecutive days to a reproducible pattern of change in blood glucose levels. As a result, this study conclusively shows that both the mismatches and lag time between CGM readings and blood glucose levels in response to a rapid physiological rise in blood glucose levels do not deteriorate over a 9-day period.
To some extent, our findings are surprising as it was reasonable to expect an eventual loss of sensor function over time. This is because the responses at the insertion site to a foreign body include inflammation, fibrosis, and vessel regression around the tissue surrounding the implanted object. 22 These factors can influence sensor function because of the degradation of sensor materials from reactive oxygen intermediates, 23 decreased exposure of interstitial glucose to the sensor due to inflammatory cells, 24 and collagen deposits surrounding the sensor during healing. 25 In addition, the presence of inflammatory cells can influence the concentration of glucose in the exudate surrounding the sensor. 24 As these complications can be triggered immediately after the sensor is implanted, 26 manufacturers often encourage cautious interpretation of CGM readings obtained within the first 12–24 h after initiation. 27 This early “break-in” period refers to the period of time the sensor requires to become intrinsically stable after insertion. 28 Although others have reported a higher disagreement between reference and CGM values on day 1 compared with the following days of wear, 8,13 this observation is not corroborated by our own findings and those of others 10 as indicated by the lack of differences across all performance measures between the first 2 days of sensor use. However, because our study did not examine the first 12 h of CGM use after insertion, our results do not exclude the possibility that sensor performance may have been poorer during this period compared with other times. Moreover, the possibility that foreign body reactions to the sensor can cause an increase in sensor signal errors over time is also not supported by our findings, which suggest that 9 days of wear may not be long enough for these factors to impair or degrade the function of the sensor.
Given that this study was not intended to determine the intrinsic or physiological mechanisms for changes in sensor accuracy over time, we can only speculate as to why no deterioration in sensor accuracy was reported in this study, with CGM readings at the abdominal site showing that sensor function may even marginally improve over time. As previously suggested by others, maintaining sufficient vascularization surrounding the implant is important for sensor functioning. 28,29 Although the injury caused by the insertion may damage the surrounding blood supply and limit the delivery of glucose and oxygen surrounding the sensor, 30 maybe the sensors' performance did not deteriorate because of the production of new capillaries at the insertion site. 30,31 That this could be the case is suggested by the observation that the use of angiogenic materials on sensor surface 28 can improve the performance of sensors by counteracting tissue fibrosis, 32 improving glucose diffusion, 31 preventing enzyme degradation, and encouraging vascularity. 28 Moreover, angiogenic-treated sensors are associated with a higher average blood vessel density, stabilize faster in vivo, and remain functional for longer than those that do not have any specific coating. 28 Whether the absence of deterioration and even marginal improvements of the CGM investigated in the current study were caused by such factors was not examined here because of limiting proprietary rights on sensor design.
Despite the evidence that the performance of the CGM unit tested here remains stable for at least 9 days, accuracy, especially during periods of rapid changes in blood glucose levels, was relatively poor as indicated by the marked mismatches and lag time between CGM glucose readings and actual blood glucose levels (Fig. 2). These findings provide further support to the recommendation not to use CGM readings alone for alterations in insulin dose and carbohydrate intake in type 1 diabetes. Our results are also consistent with those of others, with both physiological 19,33 –36 and intrinsic 18 factors contributing to CGM inaccuracy. Physiological factors include the delay for the concentration of glucose in the interstitial fluid to reach that in the blood. 36 Intrinsic factors for sensor inaccuracy have been shown when tested in vitro 18 and may involve the sensor construction and its effects on glucose diffusion rate through the sensor's membrane, 37 as well as the algorithm used by the CGM. 38 However, proprietary rights prevent the relative contributions of the sensors and algorithm to the inaccuracy of CGM from being accurately assessed.
Our results indicate that CGM accuracy is in general not affected by sensor insertion site, although accuracy at the abdominal site marginally improved after 9 days of wear. Other studies have also examined this issue and reported no differences in accuracy between sensor insertion sites. 10,11,39 Unfortunately, the lag time and CGM responses to rapid changes in blood glucose levels between sensor insertion sites were not assessed in these studies. 10,11,39 By exposing the CGM to reproducible pattern of changes in glucose levels on consecutive days, we found no differences in accuracy and lag time between abdominal and triceps CGM values, except on day 9. On that day, sensor accuracy, as defined by AUC and mismatches in peak glucose levels, was slightly superior at the abdominal site than the triceps site, with peak abdominal CGM values more closely matching blood glucose values. This marginally improved accuracy in the abdominal sensor may be due to better integration of the sensor into the surrounding tissue compared with the triceps sensor because of greater movement in the arm compared with the abdominal area, leading to some minor sensor extrusion. 29 This in turn may result in an increased variability in sensor signaling. It is noteworthy that, despite the better performance of the CGM at the abdominal site, all participants found the triceps site more comfortable than the abdominal site, with no complications (e.g., inflammation, bleeding, pain) reported at either site. For this reason, the small difference in accuracy between sites at day 9 may be offset by the better comfort at the triceps site.
One limitation with this study is that our assessment of CGM accuracy was confined within the physiological range of blood glucose levels. It remains to be established whether similar results would have arisen had the CGM performance been evaluated in the hypo- and hyperglycemic ranges in persons with diabetes. However, evaluating CGM accuracy within physiological range as achieved here is important as it corresponds to the blood glucose levels targeted by individuals with diabetes aiming to achieve good glycemic control. Furthermore, accuracy within physiological range is important for the effective use of rate change alarm and low blood glucose alarm by current CGMs.
In conclusion, for the first time we show that CGM sensor accuracy and lag time associated with rapid physiological changes in blood glucose levels do not deteriorate with continuous use over a 9-day period regardless of subcutaneous placement, suggesting that longer periods of wear might also be possible, at least with the CGM model used here. Whether these results extend to other CGM models remain to be established. To address this issue, we propose the adoption of the novel experimental approach described in this study for the assessment of CGM performance over time. The finding that the performance of the CGM tested here did not deteriorate even after 9 days of wear indicates that such an extended use of the sensor could markedly decrease the cost of sensor wear, 40 allowing not only CGM availability to be extended to more patients because of greater affordability, but also greater access to benefits such as improved glycemic control and less time spent in the hypoglycemic range. However, it is clear from our findings that accuracy issues and marked lag times must be taken into consideration for optimal CGM use in glycemia management.
Footnotes
Acknowledgments
The authors acknowledge the lending of CGMs from Medtronic Australasia for the completion of this study.
Author Disclosure Statement
K.E.I. has received speaker's fees from Medtronic and Medtronic Australasia, most recently in 2011. The authors have no other conflict of interests to disclose. There were no external (non-academic) sources of funding. No competing financial interests exist.