
Abstract
Background:
Artificial pancreas systems may offer a potential major impact on the normalization of metabolic control and preventing hypoglycemic events. This study aims to establish near-normal overnight glucose control and reduce the risk of nocturnal hypoglycemia using the MD-Logic Artificial Pancreas (MDLAP), an algorithm that was developed by our research group. This inpatient feasibility study is the first step towards implementing an overnight closed-loop MDLAP system at the patient's home.
Subjects and Methods:
Seven patients with type 1 diabetes (three adolescents and four adults; mean±SD age, 20.6±4.7 years; duration of diabetes, 9.6±2.6 years; body mass index, 24.3±3.9 kg/m2; and glycated hemoglobin, 7.8±0.8%) participated in a total of 14 closed-loop overnight sessions. Each participant underwent two closed-loop inpatient sessions starting at dinner alone and at dinner following exercise. The closed-loop inpatient sessions were compared with data derived from nights spent at home with an open-loop system in a similar scenario to the study protocol.
Results:
The mean percentage of time spent in the near normal glucose range of 63–140 mg/dL was 83±16%, and the median (interquartile range) was 85% (78–92%) for the overnight closed-loop sessions compared with 34±31% and 27% (6–57%) in the homecare open-loop setting, respectively. During the overnight closed-loop sessions at dinner alone 92±9% of the sensor values ranged within target range, compared with 73±19% for the sessions following exercise (P=0.03). No hypoglycemic (<63 mg/dL) events occurred during the closed-loop sessions.
Conclusion:
Closed-loop insulin delivery under MDLAP is a feasible and safe solution to control overnight glycemia.
Introduction
Approximately one-third of each day is spent in sleep with no meals or exercise; hence the overnight period is a significant proportion of the time requiring good glycemic control for patients with T1DM. The implementation of insulin pump and continuous glucose sensing for the treatment of diabetes has been demonstrated to improve overall glycemic control but not nighttime control. A study by Deiss et al. 6 showed that changing from multiple daily injections to pump therapy significantly improved glycemic control, but not the nighttime glucose control. The use of continuous glucose monitors in well-controlled children with diabetes demonstrated a significant improvement in daytime glucose control but, again, not overnight control. 7 The obvious explanation for the limited improvement overnight recorded in both of these studies is the lack of an appropriate intervention for patients who are asleep, even the ones who are most motivated and well controlled. It has also been shown that the glucose sensors alarming for decreasing blood glucose level are not successful in significantly reducing nocturnal hypoglycemic events as 71% of children with diabetes do not respond to the alarms during the night. 8
Therefore, a feedback closed-loop system for controlling glucose levels throughout the night has the potential to decrease hypoglycemic events and maintain good glycemic control and thus liberates the patients with diabetes, their families, and caregivers from the anxiety and stress associated with this period of time. Moreover, an assessment of parental attitudes regarding automated glucose control revealed that 90% of them would feel confident in using an overnight closed-loop system. 9
A major concern in using continuous glucose monitoring (CGM) for closed-loop systems is the sensor accuracy over a wide array of glucose levels, especially the hypoglycemic range. Several studies have demonstrated that CGM was less accurate during the night than during the day, leading to overestimation of the frequency of nocturnal hypoglycemia. 10,11 This might be due to decreased movement or to changes in the subcutaneous circulation or oxygen availability overnight. Furthermore, when glucose is falling, interstitial glucose may fall before plasma glucose and reach nadirs lower than corresponding glucose levels. 12 These accuracy issues may be automatically detected by looking at the sensor raw data. Nevertheless, overestimation of hypoglycemia or earlier detection might be safety advancement to a closed-loop system.
The MD-Logic artificial pancreas (MDLAP), an algorithm that was developed by our research group, applies fuzzy logic theory to imitate lines of reasoning of diabetes caregivers in order to establish good glucose control, as demonstrated in previous studies. 13 This system provides a personalized treatment approach with real-time learning ability. 14 It uses a combination of control-to-range and control-to-target strategies to automatically regulate individual blood glucose levels, in addition to safety algorithms for prevention of hypoglycemia, prolonged hyperglycemia, etc. 13
The study was carried out within the framework of the Diabetes Wireless Artificial Pancreas Consortium (DREAM) project that was established in order to carry out studies that will evaluate the efficacy and safety of the MDLAP system in controlling the blood glucose levels of patients with T1DM during the night at home. It is a multicenter, multinational consortium with centers in Slovenia, Germany, and Israel. We conducted a validation study, testing MDLAP overnight at inpatient settings under two main challenges: dinner alone and dinner following exercise.
Research Design and Methods
The current study was designed as a prospective feasibility trial to assess overnight closed-loop glucose control under MDLAP. From October 2010 to February 2011, seven patients with T1DM attending the National Center for Childhood Diabetes at Schneider Children's Medical Center of Israel were recruited. Inclusion criteria were >14 years old, disease duration of at least 1 year, and treatment with an insulin pump for at least 3 months. Patients with a concomitant disease affecting metabolic control or another medical condition that could affect their safety during the trial were excluded, as were patients with a known or suspected allergy to the trial products or who had participated in another study involving drugs that could affect glucose measurements or glucose management.
The study was approved by the institutional ethics committee and carried out in accordance with the Declaration of Helsinki. All subjects/surrogates signed an informed consent form.
Seven patients (three adolescents and four adults; four females and three males), 20.6±4.7 years old, with duration of diabetes mellitus of 9.6±2.6 years, duration on insulin pump of 6.1±2.5 years, body mass index of 24.3±3.9 kg/m2, total daily insulin dose of 0.96±0.48 units/kg/day, and glycated hemoglobin (HbA1c) of 7.8±0.8% (61.4±9.6 mmol/mol), participated in 14 closed-loop sessions. The Body Mass Index-SD Score for the three adolescents was 1.31, 0.25, and 0.05.
Each patient attended two automated overnight closed-loop sessions on two separate occasions. One session consisted of the subject's having dinner only (“Visit 1”), and the second session consisted of the subject's having dinner after having taken part in exercise (“Visit 2”). Each session was supervised by a diabetologist. In both visits, patients ate dinner comprising approximately 45–50 g of carbohydrates at around 19:00 p.m. followed by a postmeal fast until the following morning.
Study protocol: procedures
Preparation visit
Prior to each closed-loop session, the patients wore a continuous glucose monitor (Sof-sensor®; Medtronic, Northridge, CA) for a period of 6 days and used an insulin pump that was compatible with the MDLAP system (MiniMed Paradigm® Veo™ insulin pump+CGM; Medtronic). They were instructed to use the bolus calculator in their insulin pumps in order to record their carbohydrate consumption during this period and to use only their own glucometer throughout the study (FreeStyle®; Abbott Diabetes Care, Alameda, CA) (coefficient of variance between 2.2% and 2.4%). A short-acting insulin analog (NovoRapid®; Novo Nordisk, Bagsvaerd, Denmark) was used. The learning algorithm utilized the data downloaded from the sensors, pumps, and glucometers to create the patients' profile for application in the MDLAP system. 14 All patients were healthy during the 6 days at home.
Visit 1: overnight closed-loop session starting at dinner alone
Patients arrived at the study center at approximately 16:00 h. Intravenous access was obtained, and a venous blood sample was taken to check their blood glucose levels according to the YSI® 2300 STAT PLUS™ (Yellow Springs Instrument Co. Inc., Yellow Springs, OH), and at the same time the patients used their own glucometers. The patients' blood glucose levels were brought as close as possible within the range of 90–120 mg/dL prior to eating dinner: in order to achieve this, they were given correction boluses or carbohydrates as necessary.
All patients received their dinner around 19:00 h. Patients could choose one of two standard meals containing 45–50 g of carbohydrates (one vegetarian and one with meat). Patients/parents were asked to estimate the carbohydrate content of the meal and to give an insulin bolus 10 min beforehand based on their estimation and the current capillary blood glucose level. From this time onward automated control of all insulin delivery was carried out via the closed-loop MDLAP system. To assure the safety of the patients, blood glucose levels were checked via the patient's home glucometers at the following points: before dinner, 2 h postmeal, prior to bed at around 23:00 h (when they were encouraged to go to sleep), and every 2 h throughout the night until 07:00 h when the patients were awakened and disconnected from the closed-loop system. The CGM system was calibrated before dinner and at bedtime using the glucometer values that were measured at that time.
Visit 2: overnight closed-loop session starting at dinner following exercise
The exercise session took place between 17:00 and 18:00 h and included walking on a treadmill with increasing resistance until a target heart rate of 140 bpm was reached. This was divided into three 10-min segments with 5 min of less intensive activity between them. Prior to exercising, the patients adjusted their insulin treatment and/or consumed carbohydrates as they normally do in preparation for a 40-min exercise session. Blood glucose levels were checked via their glucometers at the start and at the end of exercising, and the sensor levels were monitored throughout. After the exercise was completed, dinner was served at 19:00 h as for the first session followed by the activation of the MDLAP closed-loop system.
Automated MDLAP system
We developed the artificial pancreas link (AP-Link) software that enables our MDLAP system to communicate wirelessly with the Paradigm Veo insulin pump and glucose sensor (Medtronic, Northridge, CA). The AP-Link has a human interface that logs and presents data, incorporates safety rules, facilitates physician overview, and provides alerts to the user in case technical or clinical safety issues arise. The AP-Link software is designed to be simple and easy to operate with a double click start-up procedure. Once the patient's profile has been established and the personal pump identification has been entered, the system is activated and automatically regulates its own safety checks. It operates the closed-loop only when all indicators confirm that it is safe to do so. The MDLAP's algorithm uses fuzzy logic technology, which has been previously described in detail. 13 The sensor readings are fed automatically into the MDLAP system every 5 min, and the system provides an insulin dose recommendation after each reading, which is then automatically transmitted to the pump.
Data analysis and statistics
The overnight period was defined as the time between bedtime (23:00 h) and wakeup (07:00 h). The primary glycemic control outcome measured was percentage of time glucose levels spent within the target range of 63–140 mg/dL. Secondary outcomes included mean glucose concentration, the percentage of time glucose levels spent below and above the glucose target range, the number of hypoglycemic events (glucose level below 63 mg/dL), glucose levels at bedtime and upon awakening, High and Low Blood Glucose Indexes (variability indexes), 15,16 and insulin infusion rates. The post-dinner results (the period of time between meal [19:00 h] until bedtime [23:00 h]) included peak postprandial glucose level, 2-h postprandial glucose levels, number of hypoglycemic events, and insulin infusion rates.
We compared the glycemic control between the closed-loop session with dinner alone (Visit 1) and the closed-loop session following exercise (Visit 2) to evaluate the effect of physical activity on glycemic control. Glycemic control outcomes were analyzed during the overnight and post-dinner periods using the two-tailed homoscedastic t test.
Because this was a feasibility study we did not include a control group for comparison. Instead, in order to appreciate the results achieved, we conducted a qualitative comparison of the glycemic control during the overnight inpatient closed-loop sessions with CGM data collected from the home setting for the same group of patients. Patients' home data were matched to the study protocol scenario for the following parameters: premeal blood glucose level, dinner eaten around 19:00 h comprising approximately 45–50 g of carbohydrate, followed by a postmeal fast until the following morning. We were able to find 15 suitable nights.
Results
There were two instances of sensor accuracy problems. In one occasion the sensor was not correlated with capillary measurements for a period of 6 h despite routine calibration. Therefore, this session was stopped per protocol. In the other occasions the sensors began to drift upwards and created a discrepancy of more than 80 mg/dL from the glucometer readings. Only after calibration did glucose sensor readings start to drop. As a result, the system overdosed with insulin, and the study physician's supplemented the patients with carbohydrates. These two instances were excluded from the overall data analysis, and will be presented separately (leaving 12 sessions: six sessions of Visit 1 and six sessions of Visit 2).
Overnight MDLAP closed-loop control
Figure 1A and B details a 12-h period from commencement of the closed-loop system at the start of the meal (19:00 h) until the time the patient woke up the following morning (07:00 h) for Visit 1 and Visit 2, respectively.
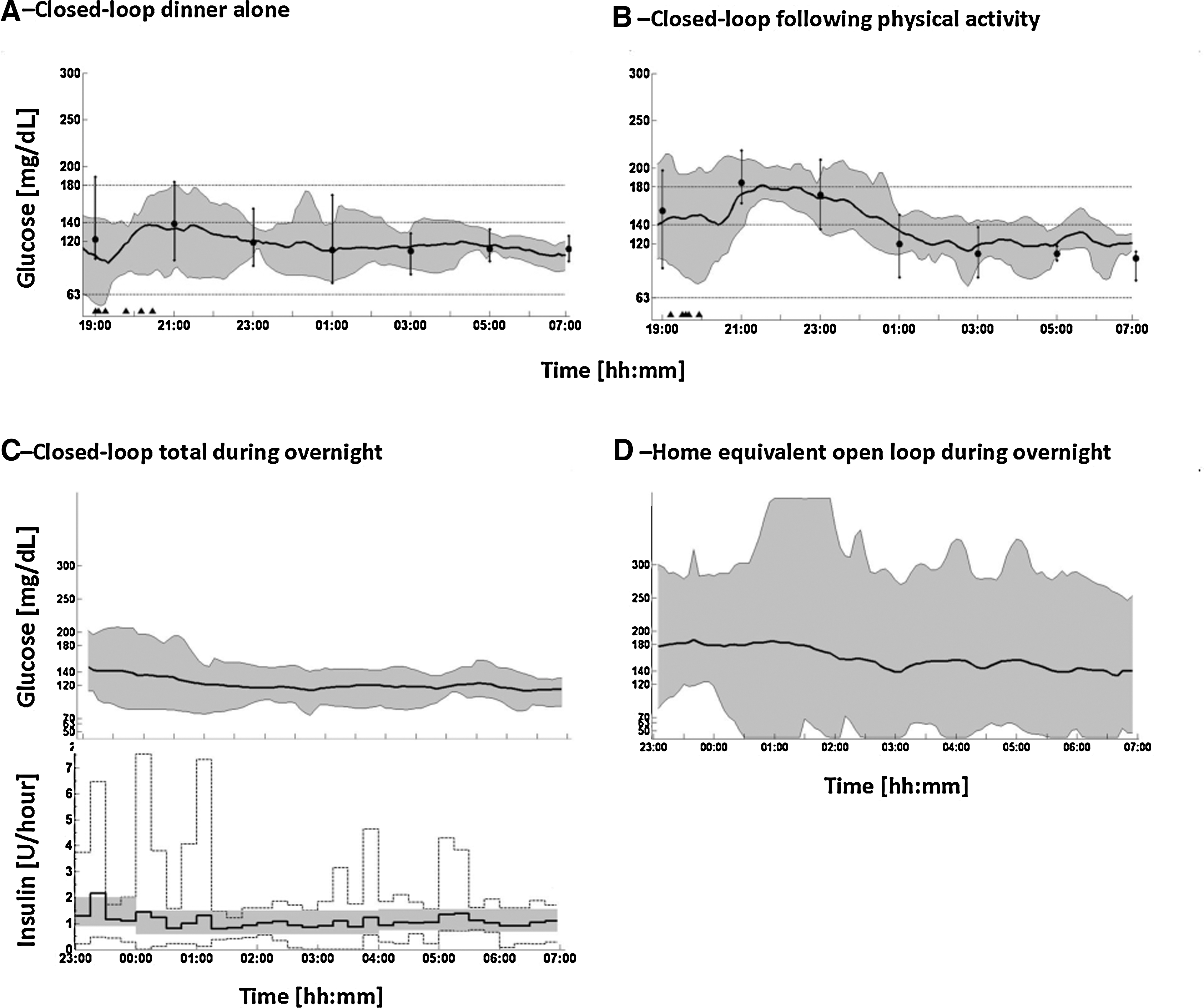
Overview of glycemic control under the MD-Logic Artificial Pancreas system. (
Closed-loop control starting at dinner alone versus dinner following exercise
Comparison of closed-loop control with (n=6) and without (n=6) exercise is presented in Table 1.
By two-tailed homoscedastic t test.
The mean glucose level at dinnertime and the amount of premeal bolus had no statistically significant differences in the two visits. However, the 2-h postprandial glucose level was significantly higher on Visit 2 compared with Visit 1 (P=0.03), causing the MDLAP system to deliver a significant additional amount of correction boluses on Visit 2 compared with Visit 1 (P=0.003). Overall visits, the peak postprandial glucose level ranged between 91 and 208 mg/dL, and the average 2-h postprandial glucose level was 161±37 mg/dL. The meal insulin for Visit 1 and Visit 2 was on average 4.8±2.6 and 4.1±1.8 units, respectively, with no statistical significance between them.
During the overnight period, the average percentage of time that glucose levels spent within target range was significantly higher on the meal-only scenario compared with the meal post-exercise scenario (92% vs. 73%, respectively; P=0.03). Mean blood glucose level was 114±11 mg/dL versus 130±8 mg/dL (P=0.02), respectively. No time was spent below 63 mg/dL in any instance. In addition, the mean insulin infusion rate was similar in the two visits.
Closed-loop versus home equivalent open-loop control
The sensor glucose profiles for the overnight period (23:00–07:00 h) during closed-loop control versus home open
Capillary measurement using a glucometer.
Excluded datasets
Figure 2 shows the two datasets that were excluded from analysis. We had one hypoglycemia event that was related to insulin overdose of the system due to sensor inaccurate readings. Nadir capillary glucose value was 53 mg/dL, whereas CGM nadir reading was 79 mg/dL. The patient was treated with 30 g of fast-acting carbohydrate, and the closed-loop trial was continued. Mean glucose levels according to CGM and capillary values were 123±32 mg/dL and 95±38 mg/dL, respectively.
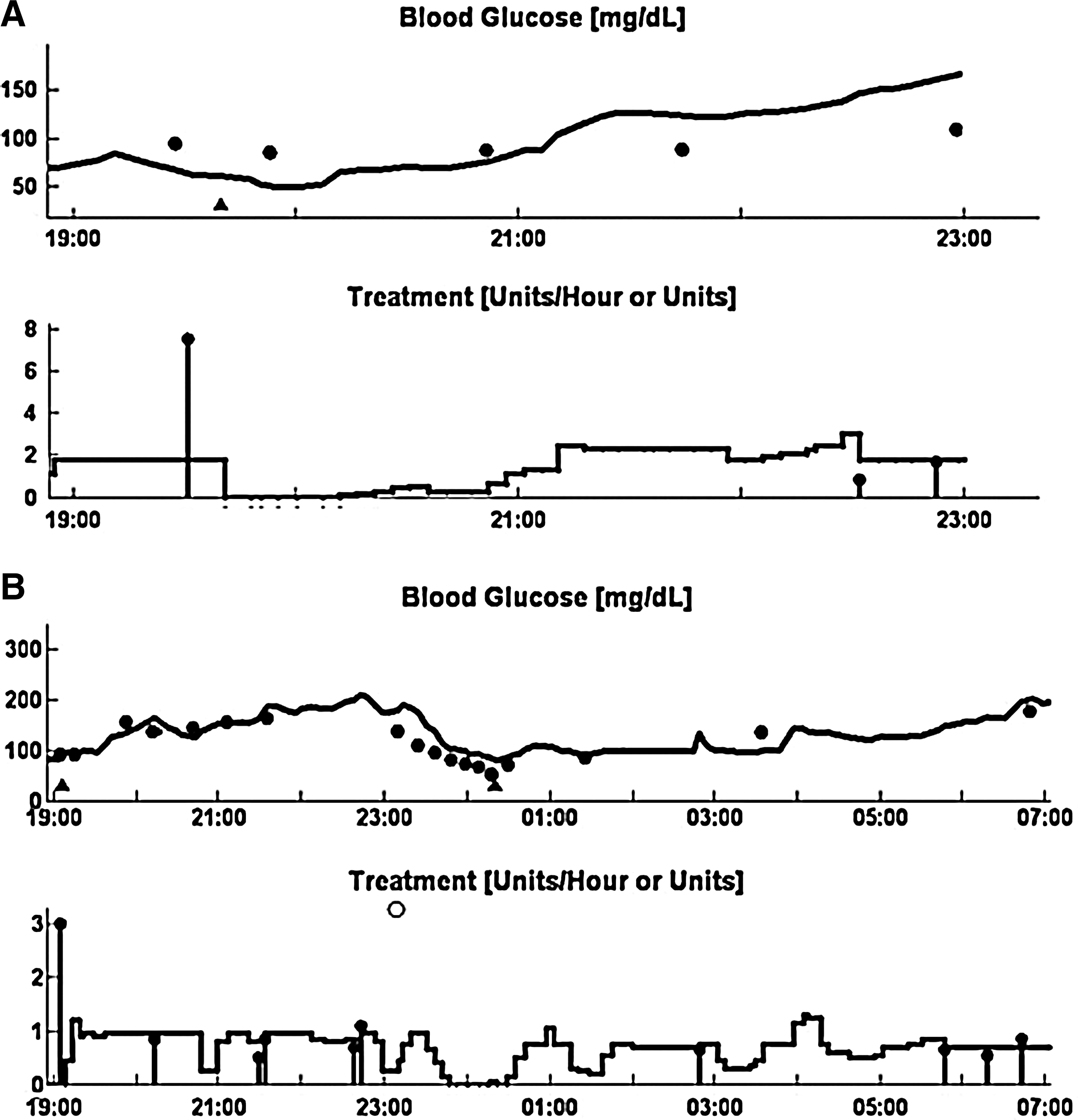
Excluded dataset results. (
Conclusions
The results of this current study demonstrate the ability of the MDLAP system to control overnight glucose levels within the near-normal range with no nocturnal hypoglycemia in young patients with T1DM. Our closed-loop system also enhanced the patients' management of blood glucose levels around dinnertime, resulting in improved blood glucose levels at bedtime with fewer overnight variables.
The present study was designed to serve as a feasibility study and therefore did not include a control group. However, we compared nights at home that had similar conditions (i.e., same meal size at a similar time of day and followed by a postprandial fast until the following morning) with closed-loop nights in a clinical research center. The overnight glucose levels at patients' homes remained within the target range for only 34% of the time and within the hypoglycemic range up to 7% of the time. The overnight results at patients' homes are similar to previous inpatient studies we had undertaken with open-loop control using similar conditions (i.e., the overnight blood glucose levels were within target range for 40% of the time). Therefore, although comparing home open-loop nights with hospital closed-loop nights is not ideal, it is reasonably representative. During the night period (23:00–07:00 h), the extent of variability of glucose levels was far less in the closed-loop nights compared with the homecare open-loop nights, possibly as a result of the better pre-bedtime glycemic levels that had been achieved during the evening in the period immediately after dinner. Despite the adjustments made to insulin delivery during the closed-loop session, the actual amount of insulin units was similar in both the closed-loop and homecare nights.
In order to achieve safe overnight control, a system should be able to cope with situations that may have prolonged influence on overnight blood glucose levels, especially those likely to cause hypoglycemia. Therefore, we included in our study overnight sessions following pre-dinner exercise. The patients who exercised prior to their meal had a higher—although not significant—premeal glucose level compared with patients who did not exercise. The 2-h postprandial value was significantly higher in the dinner post-exercise scenario (P=0.03). This finding was somewhat surprising because we expected lower glucose levels in patients who had exercised. This could partly be attributed to the patients' behavior surrounding the exercise. We instructed the patients to follow their usual routine with regards to planned exercise. Some reduced their basal rate during the exercise, and some ate carbohydrates before the exercise. None suspended his or her pump. Patients apparently overestimate the influence of exercise on glycemic control, and this may be the reason for higher post-exercise blood glucose levels. Individual patient's responses to exercise may also have contributed to this blood glucose rise. Whatever the reason could be, the time spent within target range was significantly greater (P=0.03) in the group that did not exercise before dinner, contrary to what we had expected. Indeed, Hovorka et al. 17 showed that closed-loop control provided the greatest amount of time within target range after early evening exercise. Their study included nine patients who undertook early evening exercise in a similar fashion to our protocol. In their study, the preparation for exercise included a snack of 45 g of carbohydrates with a matched insulin bolus, whereas our patients consumed 45 g of carbohydrates with no corresponding pre-exercise bolus. It is of importance to note that even though our patients' pre-exercise actions resulted in higher blood glucose levels before bedtime, the closed-loop control still succeeded in bringing their overnight blood glucose levels within range 73% of the time.
Overnight closed-loop control has been evaluated in several studies, 17 –23 all of which showed increased time spent within-target range, with fewer hypoglycemic events and of shorter duration. It is difficult to compare the results obtained from our overnight MDLAP with similar closed-loop studies because of numerous differences in methodology (e.g., duration of the overnight period, time of commencement of closed-loop control, carbohydrate content of meals, meal/exercise timings, postprandial fasting, age group, and number of participants within each study). Furthermore, the data were analyzed and presented in different ways: for instance, the time within a range was displayed as a median in some studies and as an average in others; some calculated data from sensor glucose levels and some from reference blood glucose results. We believe that these differences highlight the necessity to establish a uniform way to conduct studies on closed-loop systems and determine the appropriate way to evaluate the data for clinical application.
There were two sensor drift events in two sessions, and both involved a discrepancy of approximately 75 mg/dL between the sensor reading and the glucometer. The episodes occurred during a descent of blood glucose following an insulin bolus. The sensor glucose reading lagged behind the actual glucose level, thus preventing the artificial pancreas system from responding adequately. This demonstrates one of the safety risks faced by the closed-loop system, the reliance on sensors, which needs to be addressed.
The present study shows that the MDLAP system has important built-in layers of restraints and safety mechanisms, especially for hypoglycemia, as well as a fully integrated automatic ability to communicate wirelessly between the components of the closed-loop system. We encountered no major problems with technical communication throughout the study. Our experience in the current study shows that this mode of operation is feasible and easy to use.
In conclusion, closed-loop insulin delivery by the MDLAP system was found to be feasible and safe. Moreover, the use of the MDLAP can improve the control of glucose levels during the night and reduce the risk of nocturnal hypoglycemia in patients with T1DM.
Footnotes
Author Disclosure Statement
R.N., E.A., M.A., S.M., and T.O. declare that no competing financial interests exist. M.P. has served on Advisory Panels for AstraZeneca LP and Sanofi, as a Board Member for C.G.M.3 Ltd., as a consultant for Bristol-Myers Squibb Company, D-medical, AstraZeneca LP, Sanofi, Ferring, and Andromeda, and on Speaker's Bureaus for Animas Corporation, Sanofi, Medtronic, Bayer Health Care, has received research support from Medtronic, Novo Nordisk, Inc., Abbott Diabetes Care, Eli Lilly and Company, Roche, Dexcom, Inc., Sanofi, Insulet Corporation, Animas Corporation, Andromeda, and Macrogenetics, is a stock/shareholder in C.G.M.3 Ltd. and De-medical, and has other relationships with Bayer Health Care, Medtronic, Animas Corporation, Novo Nordisk, Inc., Pfizer, Inc., and Sanofi.