
Abstract

FA has been considered as an alternate short-term marker of glycemic control. Like HbA1c, it reflects mean glucose, but does so over a shorter time span, about 2 weeks. FA represents the sum of all glycated proteins (ketamines) in the blood, primarily albumin. 3 However, it is affected by conditions such as nephropathy and cirrhosis that alter albumin levels as well as by other low-molecular-weight substances in the blood, such as bilirubin and uric acid. 4 FA has been used to guide therapy short-term as an adjunct to HbA1c, but randomized controlled trials have had mixed results, 5 –7 with benefit only if there are specific instructions to patients and providers for tailoring therapy. 6 FA is a predictor of fetal macrosomia 7 and therefore may also have a role in pregnancy.
The GA assay was more recently developed to counter the problems with FA, as it is not affected by low-molecular-weight substances. Because the method is reported as a ratio of GA to serum albumin, conditions that alter albumin would have minimal impact. In a study of patients with advanced chronic kidney disease due to nephropathy (stages 4–5), HbA1c was significantly underestimated compared with continuous glucose monitoring (CGM) data, and GA was more closely associated with CGM measures of mean glucose. 8 More recently, it has become recognized that GA has important pathologic oxidative effects. 3,9 GA has been associated with the extent of cardiovascular disease in patients with diabetes. 10 It is also a better predictor of arterial stiffness than HbA1c in end-stage renal disease patients with diabetes. 11 Although studies have used GA to implement changes in regimens, 12 there are no randomized studies testing whether its use achieves better outcomes.
1,5-AG is a polyol that is maintained at steady-state levels in the blood because of metabolic inertness and a large internal pool with relatively small net intake or excretion under normal physiologic conditions. 13 During hyperglycemia, the renal threshold for glucose excretion (approximately 180 mg/dL) is surpassed, and glucose begins to compete with 1,5-AG reabsorption, resulting in preferential excretion of 1,5-AG and decreased serum 1,5-AG levels. Thus, 1,5-AG is an inverse marker of glycemic control. 1,5-AG has been shown to be reliable in mild to moderate chronic kidney disease but not in more advanced renal failure. 14 The use of 1,5-AG in pregnancy requires further study because variable physiologic changes in the threshold for glucosuria may affect the utility of 1,5-AG. 15 It is unclear whether serum levels are affected by sodium glucose co-transport protein inhibitors, which are currently under development.
There are currently few data supporting the role of 1,5-AG as a predictor of outcomes. Recently, 1,5-AG was shown in a cross-sectional study of over 500 subjects to be a predictor of retinopathy but not nephropathy. 16 1,5-AG has not been studied in prospective randomized trials for guiding treatment decisions, although it may be of some use in targeting therapy toward postprandial or fasting hyperglycemia. 17
In this issue of Diabetes Technology & Therapeutics, Liu et al. 18 investigate whether short-term glycemic markers are suitable predictors of remission among subjects with newly diagnosed type 2 diabetes receiving intensive insulin therapy. Remission was defined as fasting glucose <7 mmol/L and postprandial glucose <10 mmol/L for at least 3 months. 19 In their multivariable logistic regression model, 1,5-AG at 1 month following cessation of therapy was found to be the strongest predictor of remission (odds ratio 1.56, 95% confidence interval 1.15–2.12, P=0.004), whereas age and homeostasis model assessment of insulin resistance were also significant. The area under the curve for 1,5-AG in the receiver operating characteristic curve analysis was 0.85, with an optimal cut point of 8.9 mg/L, resulting in a specificity of 83.3% and a sensitivity of 78.6%. Although the acute insulin response was a strong predictor of remission following therapy in unadjusted analyses, it was no longer a significant predictor after the addition of 1,5-AG to the model. Neither FA nor HbA1c at 1 month was a significant predictor in the model. It is interesting that no baseline variables, including HbA1c, age, body mass index, homeostasis model assessment, and measures of glucose control, were significant predictors of remission.
The reasons 1,5-AG predicted remission better than other markers of glycemic control likely relate to the characteristics of the test itself. First, this was a short-term intervention, lending itself to a short-term marker. 1,5-AG rapidly reflects improvement in glucose levels over several days (up to 0.3 μg/dL/day). 19 In the study by Liu et al., 18 one may argue that testing performed at 1 month, before HbA1c has reached steady state, unfairly biases the results against HbA1c. However, this would not explain why 1,5-AG was a better predictor than FA, as discussed below. Moreover, a short-term marker would be necessary because there is no evidence that continuation of intensive therapy for 3 months (to allow for complete recovery of HbA1c) offers additional benefit.
Second, 1,5-AG exhibits a large dynamic range, increasing 57% over 2 weeks and 2.5-fold at 8 weeks of achieving normoglycemia. 20 In comparison, FA and HbA1c yield smaller changes (1.2- and 1.3-fold at 8 weeks) with the achievement of normoglycemia. 21 However, a key limiting feature of 1,5-AG is that it is most discriminating among patients with better overall control, 21,22 as in the current study. 18 In patients who are poorly controlled, GA may be superior.
Third, because postprandial hyperglycemia is an early feature of type 2 diabetes, a marker that preferentially reflects glycemic excursions may be desirable. Although 1,5-AG reflects both fasting and postprandial hyperglycemia in patients with poor overall control, it is more specific than other markers for detecting postmeal excursions in patients with good to moderate control. 23,24 As a composite marker of glycemia, 1,5-AG was superior to isolated fasting or postprandial glucose measures for predicting remission, although a formal oral glucose tolerance test was not performed. 25
The more intriguing finding is that 1,5-AG outperforms the acute insulin response (during an intravenous glucose tolerance test) for predicting remission. This is remarkable given that the acute insulin response is a known long-term predictor of glucose tolerance. 26 The precise physiologic role of 1,5-AG in humans, if any, is unknown. In insulinoma cell lines, 1,5-AG appeared to have an insulin secretory effect at physiologic concentrations, raising the question of whether it could play a role in regulating glucose-mediated insulin secretion. 27
What does this mean for informing clinical practice decisions in newly diagnosed patients? Hu et al. 28 found that patients with newly diagnosed diabetes achieving remission with intensive insulin therapy still have important pathophysiologic differences (with respect to β-cell function) that distinguish them from patients with prediabetes. Thus, with prolonged follow-up, the patients in the study by Liu et al. 18 will likely eventually succumb to disease recurrence, particularly since the definition of remission was less rigorous than that established by recent American Diabetes Association guidelines. 29 Currently, the American Diabetes Association/European Association for the Study of Diabetes guidelines do not specify criteria for discontinuation of therapy in newly diagnosed intensively managed patients, nor is insulin therapy the recommended first-line treatment for most patients. 30 Therefore, much remains to be answered regarding the appropriate treatment course for patients with newly diagnosed diabetes and whether short-term markers may be useful in this regard.
In clinical practice, frequent self-monitored blood glucose and/or CGM data may potentially obviate the need for alternate glycemic markers. However, when such data are unavailable or discrepant with the HbA1c value, alternate glycemic markers should be considered. A proposed algorithm for the use of alternate markers is presented in Figure 1.
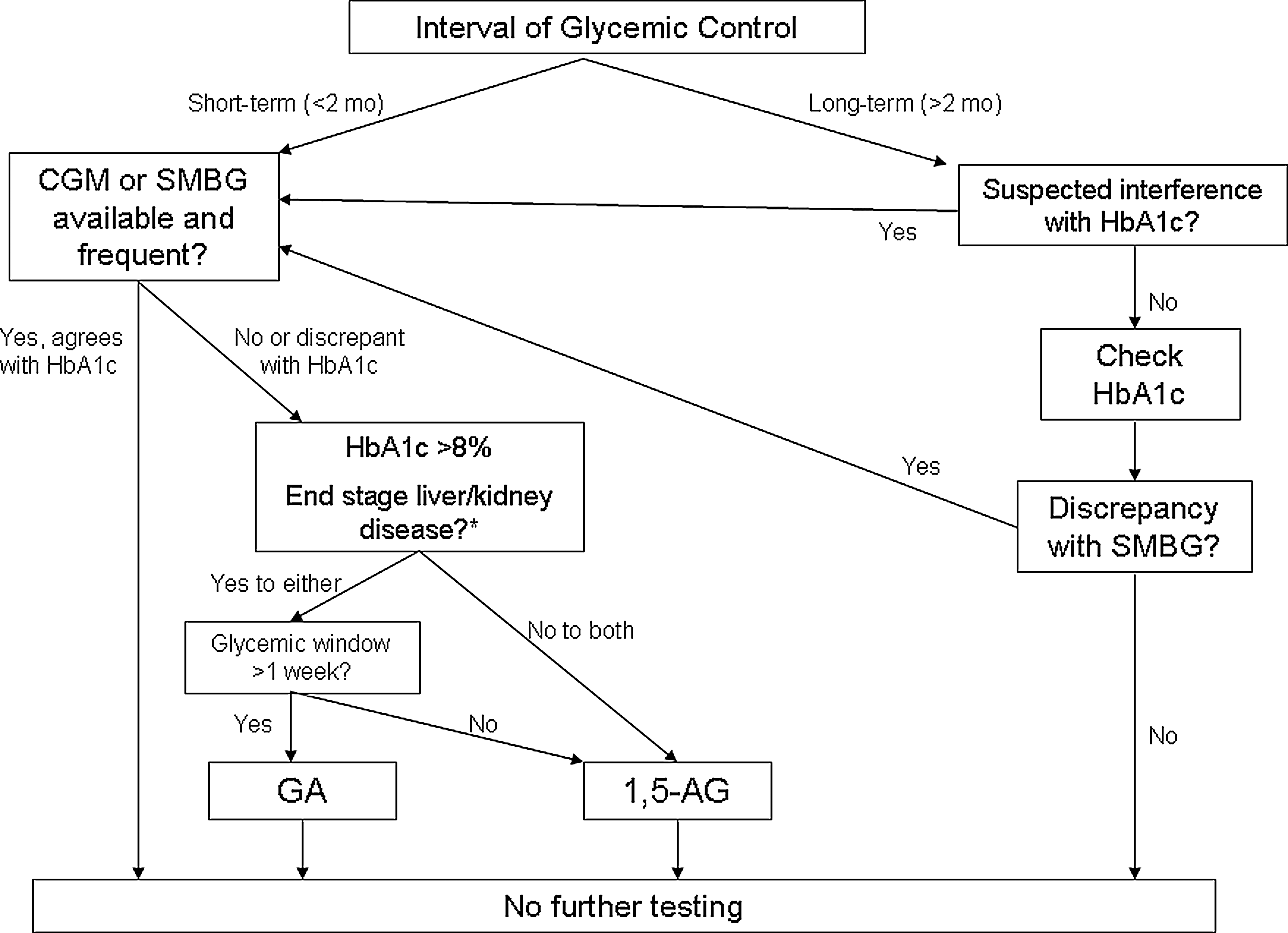
Decision tree for performing testing of alternate glycemic markers. Note that other parameters may also require caution, such as medications and conditions (for example, pregnancy) that affect urinary glucose excretion. 1,5-AG, 1,5-anhydroglucitol; CGM, continuous glucose monitoring; GA, glycoalbumin; HbA1c, glycosylated hemoglobin; mo, months; SMBG, self-monitored blood glucose.
How does one choose an alternate glycemic marker in an individual patient? First, important features of the GA assay make it the logical choice over FA, as discussed above. Otherwise, it depends upon (1) the time period over which glucose is to be estimated, (2) overall glycemic control, and (3) relevant comorbidities (Fig. 1). Recent data using CGM as a tool suggest that GA is a better marker of mean glucose, glucose excursion, and SD than 1,5-AG or HbA1c in patients with diabetes with variable but stable chronic control. 31 A smaller CGM study among unselected patients found similar correlation among HbA1c, FA, GA, and 1,5-AG and mean glucose and glucose excursions, but patients were not selected for stability of glycemic control or change in therapy. 32 Fair comparisons necessitate the use of long-term CGM or patients with stable glycemic control over the life of all markers (12 weeks for HbA1c). 1,5-AG is preferred when rapid changes in glycemic control are followed or when a postprandial glucose marker is desired (at least where the HbA1c level is <8%). 1,5-AG would be more useful to establish changes over very short intervals of 1 week or less. GA would be preferred in patients with advanced renal or liver failure and during pregnancy.
In summary, emerging data are further defining a niche for each marker of glycemic control. The available evidence suggests that GA should be preferred for patients with poor overall control and that 1,5-AG would be more useful in patients with good–fair control, particularly if targeted therapy is desirable. Prospective studies with diverse populations and longer-term follow-up are needed to establish utility for guiding treatment decisions and definitive associations with complications.