
Abstract
Background:
Patients' knowledge, attitudes, and behavior play a large role in preventing and managing the risk factors making up metabolic syndrome (MetS). MetS is associated with increased morbidity and mortality per the World Health Organization criteria. The objective of the study was to examine the current health literacy levels, risk perceptions about MetS, and associated management challenges in diverse Indian settings.
Subjects and Methods:
This cross-sectional study was performed during the period of April–May 2012 by enrolling 125 individuals at risk of MetS from urban, rural, and slum settings in India. A convenience sample was recruited from primary care clinics. In-depth interviews were conducted using ground theory and framework analysis. Individuals 30 years old and above with confirmed diagnosis of obesity, type 2 diabetes mellitus, hypertension, or hypercholesterolemia and willing to participate in the in-depth interviews were included in the study. Individuals involved in other research studies were excluded.
Results:
Difficulty in understanding healthcare information was commonly reported, especially in rural and slum settings. Only 10% of the individuals perceived lifestyle behaviors as a risk factor of acquiring MetS. Significant disparities were seen among urban, rural, and slum individuals about using diet and exercise as means to manage their MetS. Individuals in slum and rural settings were rarely advised about diet and exercise approaches to manage MetS. Access to appropriate information and direction from the healthcare professionals is lacking.
Conclusions:
Different perceptions about MetS and its varied management approaches exist across the three settings. An urgent need exists to develop interactive health education programs that can enhance self-management approaches to meet the growing burden of MetS by providing access to right information applicable to individuals living in diverse Indian settings.
Introduction
Extracted from Alberti et al.6
Extracted from World Health Organization.8
Extracted from Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults.7
Values given are for systolic/diastolic blood pressure.
ATPIII, National Cholesterol Education Program's Adult Treatment Panel III; BMI, body mass index; HDL, high-density lipoprotein; IDF, International Diabetes Federation; MetS, metabolic syndrome; WHO, World Health Organization.
Studies have shown that the prevalence of MetS continues to increase globally, regardless of the definition used. 9 –15 MetS is commonly associated with an increased risk of type 2 diabetes mellitus (T2DM) and cardiovascular disease. 16,17 Central obesity plays a very important role in diagnosing MetS as it induces multiple abnormalities that eventually contribute to the pathogenesis of T2DM and cardiovascular disease. 16,18 MetS prevalence is rapidly increasing in India. In one of the largest diabetes studies conducted in India, the Chennai Urban Rural Epidemiology Study, MetS prevalence was 23.2% (World Health Organization criteria), 18.3% (ATPIII criteria), and 25.8% (International Diabetes Federation criteria). 9 Recent data have shown approximately one in three urban individuals have MetS. 19 However, much lower prevalence has been estimated in rural settings. One study has shown the rural prevalence of MetS to be 9.3% (ATPIII criteria) 20 ; another study found an estimated prevalence between 4.4% and 11.0% (ATPIII criteria). 21
Individuals with MetS require continuous ongoing support to self-manage their disease state, but several barriers exist to help modify risky lifestyle behaviors. Changes in diet and exercise can prevent MetS transformation into T2DM and cardiovascular disease in high-risk individuals. 22,23 The ATPIII prioritizes treatment with therapeutic lifestyle change for individuals with lifestyle-related risk factors. 24 Improving adherence to treatment plans is another important goal of education programs, and prior studies have shown that treatment adherence is correlated with improved outcomes in individuals with both T2DM and hypertension. 25 To achieve such changes in behavior, it is essential to first understand the current knowledge, attitude, and practices related to MetS and what barriers are encountered by individuals.
Good patient–provider relationship and patient education are crucial to reducing these barriers. 26,27 Health literacy is broadly defined as the degree to which individuals have the capacity to understand basic health information and services needed to make appropriate health decisions. 28 Inadequate literacy level leads to unsuccessful education programs, as they usually rely on high-level written material. 29 Successfully communicating recommendations requires context-specific information, multimedia-enabled and in a format appropriate to meet the needs of the individuals. Advances in information and communication technology are leading to better delivery of patient-centered care compared with conventional modes of patient information. Emerging fields such as telehealth, mobile health, and electronic health can lead to an improvement in patients' knowledge, attitude, and practices and increase the probability of individuals engaging in healthy behaviors. 30,31 Interactive health information programs can be tailored and targeted to the specific needs of the community or the individual and delivered through electronic health kiosks. 32 The health kiosks interface can be designed for adequate use by individuals regardless of setting, socioeconomic level, or education level. 33,34
Currently, information is limited or nonexistent in the literature on patients' health-related behavior in the context of knowledge and attitudes about MetS for individuals living in diverse Indian settings. The objective of the study is to compare and contrast the knowledge, attitude, and practices of individuals living in diverse Indian settings for the prevention and management of MetS.
Subjects and Methods
A cross-sectional study was performed during a period of April–May 2012 by enrolling individuals at risk of MetS from diverse Indian settings such as urban, rural, and slum. A convenience sample was recruited from primary care clinics. In-depth interviews were conducted, and both qualitative and quantitative data were gathered. Individuals 30 years of age and above, with confirmed diagnosis of obesity, T2DM, hypertension, or hypercholesterolemia and willing to participate in the in-depth interviews, were included in the study. A checklist with obesity, blood sugar, blood pressure, and cholesterol information was filled out for each potential participant, and confirmation of MetS was achieved if an individual presented three or more criteria. Body mass index, blood pressure, and blood sugar level measurements were taken using a digital weight scale, a blood pressure device, and a point-of-care glucometer testing, respectively. Fulfillment of the criteria was verified by confirmed physician diagnosis, prescription records, and medications list and by testing at recruitment; otherwise, if the individual did not have any of the previous requirements, the tests were conducted at the recruitment site. Individuals involved in other research studies were excluded. Quantitative assessments included information about (1) sociodemographics and (2) health literacy assessments. Sociodemographic information included variables such as age, gender, location of residence, educational level, current employment status, income, smoking, and alcohol consumption. Health literacy assessment was performed using a previously tested questionnaire. 35 Questions were selected based on five domains: navigating the healthcare system, completing medical forms, following medication instructions, interacting with providers, and reading appointment slips. 36
The questionnaire included 11 open-ended questions about MetS and its related components, more specifically, T2DM, hypertension, hypercholesterolemia, and obesity (Supplementary Table S1; Supplementary Data are available online at
Overall, 125 individuals from urban and rural areas of Bhubaneswar and Baleshwar, India, were enrolled and also from Saliasahi Basti, an urban slum in Bhubaneswar, Orissa. Forty-five people were from an urban area and 40 people each from rural and slum area participated in the study (Fig. 1). Informed consent was obtained from the participants, and audio recording of in-depth interviews was done. Transcription of the audio recording of the in-depth interviews was performed, and common themes were identified. Qualitative analysis was conducted through ground theory and framework analysis, which provided a clear series of steps to manage the data. This framework uses a thematic approach, allowing themes to develop both from the research questions and from the narratives of research participants. 37 The analytical process involves several distinct although highly interconnected stages, including familiarization, identifying a thematic framework, indexing, charting, mapping, and interpretation. 37 The emerging variables were dichotomized (yes/no) according to the individual responses and compared using χ2 analysis to assess differences across the three settings. Descriptive analysis was performed using univariate statistics to report mean and SD values for the continuous variables and frequency distributions for the categorical variables. The χ2 analysis was performed to compare frequency distribution of the various categorical variables among individuals living in diverse settings. Significance of the results were reported as P values for two-sided tests (α=0.05), and analysis was performed using SAS version 9.1 software (SAS Institute, Cary, NC). The study experiments comply with the current laws of India, and the study was approved by the Asian Institute of Public Health, Bhubaneswar Institutional Review Board (protocol number 621).
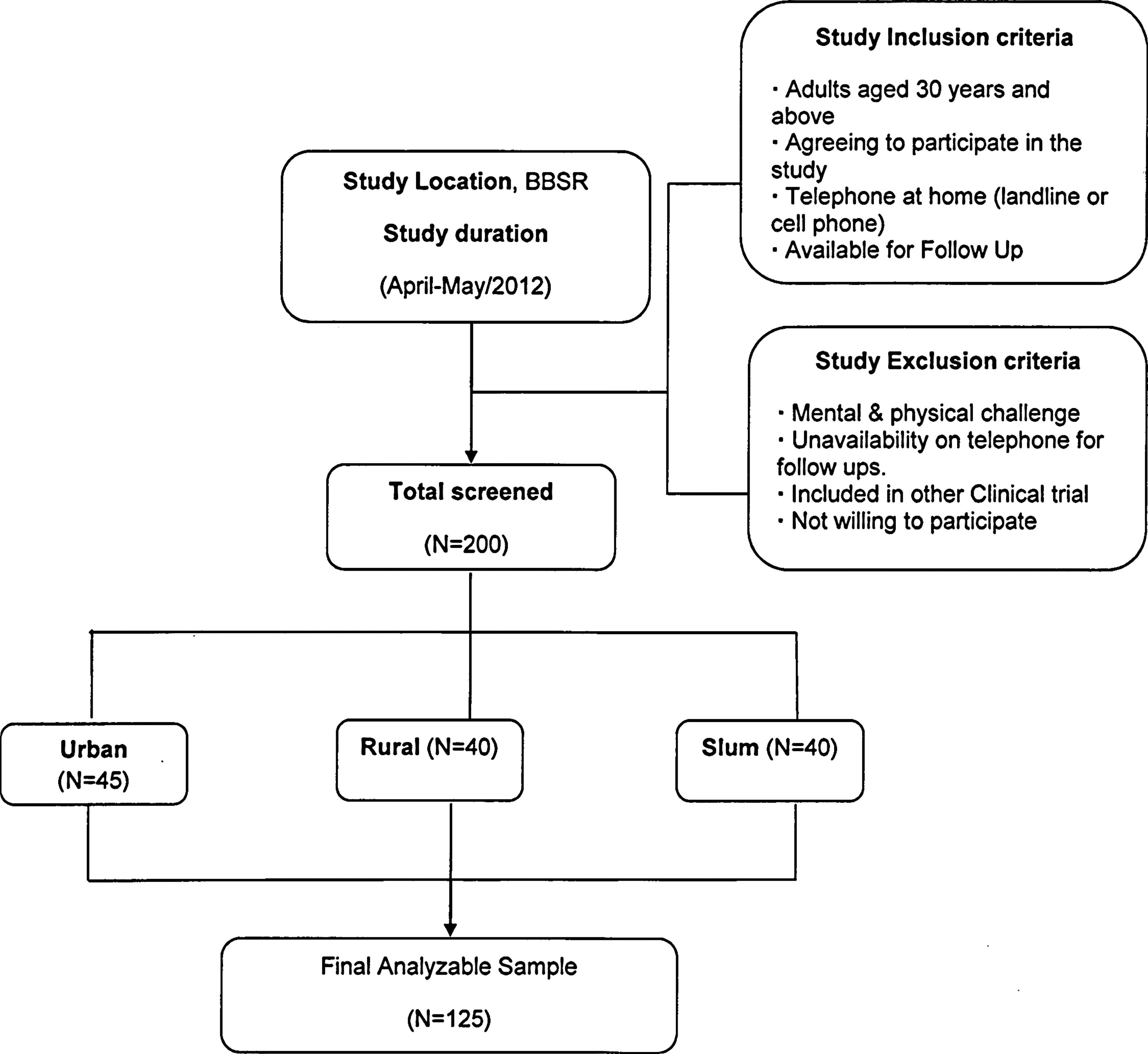
Study enrollment. BBSR, Bhubaneswar–Baleshwar–Saliasahi Basti.
Results
The total number of individuals enrolled after screening was 125, well distributed among the three different settings. Most individuals belonged to the age groups of 51–60 years and above 60 years. The majority of individuals were male (66%; n=82). Among individuals that reported being unable to work due to MetS (n=24), a higher proportion was found in rural (27.5%; n=11) and slum (25%; n=10) settings compared with urban (7%; n=3). The majority of the individuals reported having less than high school for educational level in the rural setting (65%; n=26), where 5% (n=2) declared not having a formal education; respective values for the slum setting were 66% (n=26) and 28% (n=11). More details on the sample characteristics can be found in Table 2.
Significant values at α=0.05.
MetS, metabolic syndrome.
Health literacy assessment
The majority of the individuals had difficulty in understanding information from healthcare providers and written healthcare information (54%; n=68). Over half of the individuals from rural (53%; n=21) and slum (48%; n=19) settings had difficulty in understanding written information (Fig. 2). Individuals from the rural setting (42%; n=17) had greatest difficulty in understanding information from the healthcare provider compared with individuals living in slum (25%; n=10) and urban (2%; n=1) settings, and this difference was significantly different (P<0.001). Similarly, individuals from the rural setting (38%; n=15) had the greatest difficulty in understanding directions on medication containers compared with those individuals living in the slum (33%; n=13) and urban (2%; n=1) settings, and these differences were significant (P<0.001).

Frequency distribution of individuals' health literacy assessment.
Individuals from the rural settings (28%; n=11) were also unsure about how to take their medications correctly compared with those individuals living in slum (8%; n=3) and urban (2%; n=1) settings, and this difference was significant (P=0.001). More than half of the individuals from the rural settings (58%; n=23) needed help from someone to read information compared with 23% (n=9) living in the slum setting and none in the urban setting (P<0.001).
Screening of individuals with MetS components
Hypertension was predominantly the most common disease condition found among individuals with MetS across urban, rural, and slum settings. Combined hypertension and abnormal blood sugar levels were highest among individuals living in slum settings. Sixteen percent (n=20) of the individuals were identified to have MetS during their screening at the point-of-care testing. A higher proportion of individuals living in the slum setting (30%; n=12) was diagnosed with MetS for the first time at recruitment compared with 12.5% (n=5) who lived in the rural setting and 9% (n=3) who lived in the urban setting (P=0.01).
Qualitative assessments
Perceptions on how MetS is acquired
There were few individuals who perceived that they had acquired MetS due to a certain lifestyle (10%; n=13) (Table 3). Individuals living in the slum setting more often reported lifestyle (20%; n=8) as an important factor resulting in MetS relative to urban (11%; n=5) and rural (n=0) individuals (P=0.006). Less physical activity and a sugar-rich diet were the most commonly reported lifestyle factors overall. In the rural setting, no individuals perceived lifestyle to contribute to acquiring MetS, and knowledge of MetS or T2DM was usually achieved after seeking medical attention because of certain symptoms. Responses such as “I was getting head reeling, then I went to the doctor and checked” or “I was doing my daily work,…feeling weakness, head reeling, thirsty,…I did not ask anybody…I visited the nearest doctor and tested FBS [fasting blood sugar], which came 580” were common among rural individuals. Although in small number (8%; n=3), individuals living in the slum setting were the only ones who identified alcohol consumption as a possible contributor to acquiring MetS. Smoking was reported as a risk factor by only one individual from the urban setting.
Significant values at α=0.05.
MetS, metabolic syndrome.
Approximately 39% (n=49) of the individuals were able to describe the most common symptoms associated with MetS. As already suggested above, individuals living in a rural setting had a very symptomatic concept of MetS. The majority of rural individuals were able to report symptoms relevant to MetS (73%; n=29). This was significantly different from those individuals who were living in slum (30%; n=12) and urban (18%; n=8) settings (P<0.001). The most common symptoms were dizziness, polyuria, and generally not feeling well. Pain, body aches, headaches, and fever were also reported.
MetS perceived risk
The majority of the individuals perceived MetS as a risk (67%; n=84). Individuals living in the slum setting were more prone to perceiving MetS as a risk (70%; n=28) compared with the rural (68%; n=27) or urban (64%; n=29) setting, but the difference was not significant (P=0.861). Urban individuals often reported receiving advice on managing and treating MetS, and they are more often diagnosed by a health professional (62%; n=28) compared with rural (55%; n=22) or slum (20%; n=8) individuals (P<0.001), which may lead to the reduction in risk perception. For example, one urban individual reported “[the neurologist] advised me to take medicine to reduce sugar level in my body…I think this is a common disease, so I can maintain a common life without any fear,” whereas another individual reported, “I go to hospital monthly to receive care.”
MetS management approaches
The majority of the individuals were currently managing MetS (81%; n=101). More individuals living in the urban setting (93%; n=42) were currently managing MetS compared with rural (85%; n=34) and slum (63%; n=25) individuals (P=0.001). A higher percentage of individuals living in urban settings was managing the condition with diet (84%; n=38) compared with rural (60%; n=24) and slum (35%; n=14) individuals (P<0.001). Similarly, physical activity was more common among urban individuals (62%; n=15) than rural (38%; n=13) and slum (35%; n=16) individuals (P=0.02), and the same applied to medication management, with 80% (n=36) of urban individuals perceiving its benefits compared with 48% (n=19) living in rural and 30% (n=12) living in slum settings (P<0.001).
MetS management benefits
Overall, the majority of individuals (81%; n=101) considered the different types of management to be beneficial in the prevention of MetS. Perception of MetS management benefits was not significantly different (P=0.947) among the diverse settings, however. Exploring the perceptions about different management approaches, it was found that diet management was considered beneficial by a higher percentage of individuals living in the slum setting (43%; n=17) compared with rural (28%; n=11) and urban (18%; n=8) settings (P=0.042). More rural individuals (68%; n=27) saw medication intake as beneficial compared with individuals living in the urban (56%; n=25) or slum (30%; n=12) setting (P=0.003). No significant differences were observed for physical activity (P=0.741). The results seem to indicate that individuals living in slum areas rely more on diet and physical exercise to manage MetS, whereas urban and rural individuals tend to see benefits in managing their condition with medication. Individuals living in slums may lack economic access to adequate medication. It is also interesting to note that the highest proportion of individuals who perceive benefits of medication was living in a rural area, which may be related to the symptomatic perception these individuals have of MetS.
Adherence with MetS treatment
The majority of the individuals were taking prescribed medication as advised (68%; n=85). In the urban setting, almost all individuals (98%; n=44) were taking the prescribed medication compared with 63% (n=25) of individuals in rural and 40% (n=16) in slum settings (P<0.001). Rural and slum individuals reported challenges to follow the treatment as prescribed by their doctor. One individual from the rural setting declared that “I am very poor, so I am not able to prepare separate food for myself.” Other rural individuals have noted “insufficient time” or “living with joint family” as barriers to following an adequate diet. Costs of treatment were a challenge also for individuals living in the slum setting, as one individual reported, “I am unable to buy medicine due to financial problems…if the treatment is available free of cost, I will take the medicine as prescribed by the doctor.” Difficulty in understanding the doctor's advice was stated as an issue by rural individuals, and some may rely on relatives to interpret the information. One individual from the rural setting stated that “… my grandson clearly understands the doctor and tells me how to take the medicine.” Individuals living in rural and slum settings received advice on diet and physical activity management less often than those living in the urban setting (P<0.001).
Sources of health information
The majority of urban individuals reported television as their current source of health information (64%; n=29) compared with rural (23%; n=9) and slum (20%; n=8) residents (P<0.001). A higher proportion of urban individuals (36%; n=16) also reported newspapers as a source compared with 10% (n=4) of individuals living in rural and 5% (n=2) in slum settings (P<0.001). The majority of individuals from rural (68%; n=27) and slum (65%; n=26) settings referred to a health professional as their source of health information compared with 29% (n=13) of urban individuals (P<0.001). Family members and friends were mentioned across the three settings without significant differences (P=1.00). Family members may be, however, essential for the successful communication of health information, as one rural individual stated that “… my son describes the health information to me.”
MetS modules information
Seventy-eight percent (n=98) of the individuals expressed an interest in obtaining more MetS-related health information. Almost all individuals from urban settings (93%; n=42) appreciated having MetS-related health information that can help them manage their condition, compared with 85% in rural (n=34) and 55% in slum (n=22) settings (P<0.001). A higher proportion of individuals living in the urban setting (36%; n=16) would like more information on physical exercise compared with rural (13%; n=5) and slum (18%; n=7) residents (P=0.03). More information on medication was required by a higher proportion of rural individuals (25%; n=10) compared with urban (13%; n=6) and slum (5%; n=2) residents (P=0.04). There was no significant difference on information about diet across the three settings.
Preferred mode of health information delivery
No significant differences were found in preference for health information sources across the three settings. It is important to note, however, that individuals in slum and rural settings more often reported the health professional as a preferred source of information compared with those in the urban setting. In addition, urban individuals seem to demonstrate a preference for written information compared with rural and slum residents. Some individuals from rural and slum settings reported that it would be helpful to have the information communicated in the local language.
MetS impact on overall quality of life
The majority of the individuals (71%; n=89) agreed that MetS had an overall impact on their quality of life. A higher proportion of urban individuals (84%; n=38) declared that MetS had an impact in their life compared with slum (76%; n=28) and rural (58%; n=23) residents (P=0.02). Depression reports were higher among individuals living in rural settings (28%; n=11) relative to individuals from slum (10%; n=4) and urban (n=0) settings (P<0.001). Similarly, reports regarding work disabilities were also higher for rural individuals (18%; n=7) compared with slum (13%; n=5) and urban (2%, n=1) residents (P=0.046).
Discussion
The findings of the present study described important and relevant issues associated with knowledge, attitude, and practices to prevent and manage MetS. The results show limited awareness about the various risk factors related to MetS. This disparity was predominant among individuals living in rural and slum settings in India. Lifestyle-related behaviors were mainly reported in the slum setting as possible MetS risk factors, compared with no individuals living in rural settings. Overall, fewer than half of the individuals were able to describe the most common symptoms associated with MetS. Furthermore, the results seem to demonstrate that rural individuals perceived having more symptoms of MetS compared with those living in the slum and urban settings. Knowledge about MetS is still low among the general population in India, and proxy responses in relation to T2DM or high blood sugar are usually given. Improved prevention will depend on increased education related to risk factors associated with MetS. This seems necessary across all settings, but especially among rural residents, who seem to not seek help or information until becoming symptomatic.
MetS risk was perceived by the majority of the individuals, and this was significantly more often among individuals living in the slum setting, followed by rural and urban settings. Urban individuals may have a lower risk perception of MetS because of easier and better access to health care, with more knowledge about treatment derived from professional advice, or also because of better knowledge and practice of management approaches. These results may indicate that more information on different ways of managing and treating MetS is needed, in order to reduce the risk perception of individuals across the three settings. In addition, the higher proportion of rural individuals presenting depression related to their condition may illustrate further a lack of knowledge about managing and treating MetS.
Medication intake and physical activity were seen as beneficial mainly by individuals living in urban and rural settings, whereas individuals living in the slum mostly perceived diet to be beneficial. A smaller proportion of individuals from rural and slum settings was actually managing their MetS with diet and physical activity, however. This may be an indication that health education programs and campaigns targeting individuals in slum and rural areas should focus on prevention and management approaches through lifestyle. Money, time, and living with family were among the challenges reported by individuals to manage their health condition. Some individuals from the rural setting also reported reliance on family members to help them in understanding the doctor's instructions. These findings may point to the importance of family-centered health education programs in order to facilitate compliance with MetS treatment and also prevention. Previous studies have demonstrated the importance of family-centered interventions in improving diabetes knowledge and control. 38 Further research should be performed comparing the efficacy of MetS health programs directed to families with that of programs that focus on the individual across the three settings.
Individuals living in urban settings more often expressed a need for more information related to diet and physical activity in relation to MetS prevention and management compared with individuals from the slum and rural settings. More information about medication was mostly required by rural individuals. These findings corroborate to the previous discussion about improving health education regarding diverse management approaches.
The larger proportion of rural individuals preferring multimedia sources of information may be related to most of them having difficulty in understanding information from the healthcare provider. Health programs that use audiovisual resources may be beneficial to rural populations as they could be contextually tailored, in the local language, and composed by images and text related to the diverse modules of MetS information. Similar programs should be developed targeting individuals living in slum areas, who also reported at a high level difficulty in understanding written health information. Novel intervention initiatives involving the use of informatics applications using one-on-one teaching, audiotapes, videotapes, and computer multimedia should be used more often. 33,34,39 More research in this area is extremely needed, as there is currently a paucity of studies related to knowledge of MetS in the Indian population. Research regarding other chronic diseases, however, has demonstrated that patient awareness of risk factors and management approaches is usually very unsatisfactory. 40,41 Culturally appropriate health education has been shown to improve knowledge and management of diabetes with the use of visual aids. 42 Nonetheless, illiterate individuals did not perform well. Solutions to educate a large part of the Indian population in characteristics such as diabetes self-management are still being sought. 43
This was a pilot study to understand the current knowledge, attitudes, and practices regarding MetS across the various settings. Understanding the challenges and needs of these populations is paramount to the development of effective health education programs that can lead to a measurable impact in the local communities. The cross-sectional nature of the study does not allow for inferences about temporality and causality in the relationships observed. Other limitations include the self-reported data, and the convenience sample limits the representativeness of the findings. Because of this non-probability sampling method, the differences among the three settings must be interpreted with caution. The main goal of the in-depth interviews, however, was to search for recurring themes and to provide understanding of the diverse contexts of health knowledge and behavior related to MetS. The study findings identified multiple key features, including varied levels of understanding about MetS risk factors and perceptions, its symptoms, preventive strategies, management approaches, and current and preferred sources of information.
Conclusions
These findings help to understand the role of personalized health information in managing, treating, and preventing MetS. Individuals across the diverse settings tend to have different perceptions about the disease and of the role that varied management approaches such as medication intake, diet, and physical activity can play to help the individual manage MetS. Ongoing research will explore and compare these differences and how to enhance the delivery of tailored health education programs. 44 These programs should be geared to meet the needs of the diverse Indian population. An urgent need exists to develop user-centered programs that take into account individual sociodemographics, disease state, and other characteristics. They could provide interactive, tailored, and contextually relevant dietary and physical activity guidelines to manage MetS, besides illustrating and identifying the risks, symptoms, and other MetS-related information in a manner that effectively communicates the messages to each particular individual.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.