
Abstract
Background:
A reliable method to detect biochemical nocturnal hypoglycemia is highly needed, especially in patients with recurrent severe hypoglycemia. We evaluated reliability of nocturnal continuous glucose monitoring (CGM) in patients with type 1 diabetes at high risk of severe hypoglycemia.
Patients and Methods:
Seventy-two type 1 diabetes patients with recurrent severe hypoglycemia (two or more events within the last year) participated for 4 nights in blinded CGM recordings (Guardian® REAL-Time CGMS and Sof-Sensor®; Medtronic MiniMed, Northridge, CA). Blood was drawn hourly from 23:00 to 07:00 h for plasma glucose (PG) measurements (gold standard).
Results:
Valid data were obtained in 217 nights. The sensitivity of CGM was 65% (95% confidence interval, 53–77%) below 4 mmol/L, 40% (24–56%) below 3 mmol/L, and 17% (0–47%) below 2.2 mmol/L. PG and CGM readings correlated in the total measurement range (Spearman's ρ=0.82; P<0.001). In the normo- and hyperglycemic ranges CGM underestimated PG by 1.1 mmol/L (0.9–1.2 mmol/L) (P<0.001); in contrast, in the hypoglycemic range (PG<4 mmol/L) CGM overestimated PG levels by 1.0 mmol/L (P<0.001). The mean absolute relative differences in the hypo- (≤3.9 mmol/L), normo- (4–9.9 mmol/L), and hyperglycemic (≥10 mmol/L) ranges were 45% (37–53%), 23% (22–25%), and 20% (19–21%), respectively. Continuous glucose error grid analysis indicated a clinical accuracy of 56%, 99%, and 93% in the hypo-, normo-, and hyperglycemic ranges, respectively.
Conclusions:
The accuracy in the hypoglycemic range of nocturnal CGM data using Sof-Sensor is suboptimal in type 1 diabetes patients at high risk of severe hypoglycemia. To ensure clinical useful sensitivity in detection of nocturnal hypoglycemic episodes, an alarm threshold should not be lower than 4 mmol/L.
Introduction
Preliminary results of this study have been presented elsewhere in abstract form. 5
Subjects and Methods
Study design
The present study is part of an investigator-initiated, prospective, randomized, open, blinded endpoint (PROBE) multicenter, 2-year crossover trial (HypoAna) designed to investigate the effect of basal-bolus therapy with subcutaneous injection of insulin analogs (insulin detemir/insulin aspart) versus human NPH insulin/soluble insulin on the frequency of severe hypoglycemia in high-risk patients (i.e., patients with type 1 diabetes and at least two episodes of severe hypoglycemia during the year before the study). 6
The CGM study comprised two overnight stays in each HypoAna treatment arm (at 6, 12, 18, and 24 months) at the inpatient facilities at Steno Diabetes Center. A blinded subcutaneous CGM system was used (Guardian® REAL-Time CGMS using Sof-sensor® MMT-7020C; Medtronic MiniMed, Northridge, CA). Written informed consent to participate was obtained from all patients. The study was approved by The Regional Committee on Biomedical Research Ethics (protocol number H-KA-20070008).
Subjects
All adult (>18 years of age) patients diagnosed with type 1 diabetes mellitus and followed up at six Danish outpatient clinics in 2007–2009 were screened to identify candidates for participation in the HypoAna trial. In total, 3,861 subjects completed a given or mailed questionnaire about hypoglycemia as previously reported. 7 The inclusion criteria for the HypoAna trial were type 1 diabetes for more than 5 years, age >18 years, basal-bolus treatment with human insulin or insulin analogs, a negative pregnancy test, and at least two episodes of severe hypoglycemia (defined by need for assistance from another person to treat the episode) in the previous year. 6 The most important exclusion criteria were adrenal insufficiency, growth hormone deficiency, untreated myxedema, and recent history of major cardiovascular events. In total, 159 subjects fulfilling these criteria were recruited to the HypoAna study. 6 A subgroup of 110 of these patients who were followed at Steno Diabetes Center or Hillerød Hospital was invited to participate in the study of CGM performance during nighttime. Seventy-six patients agreed to participate, and 72 patients completed the study. Four patients had to be excluded (three did not return, and one was excluded because of technical failures of the CGM device during the first visit and because of the patient's failing to return at the subsequent three scheduled visits). Data on patients' history of diabetes were extracted from medical records. Previous experience of hypoglycemia was assessed in the questionnaire, and the patient's state of hypoglycemia awareness was classified according to a validated method based on the patient's self-reported ability to recognize symptoms during a hypoglycemic episode. 8 Subjects who reported always being able to recognize symptoms of hypoglycemia were classified as aware, those usually recognizing symptoms were classified as having impaired awareness, and patients occasionally or never recognizing symptoms were classified as being unaware of hypoglycemia.
Study setting
Patients arrived at the outpatient clinic at Steno Diabetes Center at 18:00 h for dinner and were observed continuously for clinical bedside signs of hypoglycemia during the night. In case of confirmed hypoglycemia the event was treated according to standard clinical instructions. The CGM device was mounted after dinner. The device consists of (1) a subcutaneous glucose oxidase sensor that converts interstitial glucose to an electrical current, (2) a radiofrequency transmitter connected to the sensor that wirelessly transmits the electrical information to a monitor every 5 min, and (3) a monitor that stores and displays the glucose data. 9 A glucokinase-based amperometric minimally invasive glucose sensor estimates plasma glucose (PG) based on the interstitial glucose concentration in the subcutaneous tissue. At bedtime and at 2:00 h the CGM device was calibrated with fingerstick meter blood glucose measurements performed according to the recommendations from the manufacturer and supervised by a diabetes specialist nurse. Hypoglycemic glucose values were not used for calibration. In the case of hypoglycemia at the planned time of calibration, hypoglycemia was treated according to clinical recommendations, and calibration was postponed until normalization of the glucose level. The CGM device was from the manufacturer dedicated to the study by blinding the display, and the alarm functions were switched off. Venous blood samples were drawn every hour from 23:00 to 07:00 h from an intravenous line inserted into an antecubital vein. As the reference method (gold standard) we determined PG on a Roche Hitachi 912 chemistry analyzer (Roche Diagnostics GmbH, Mannheim, Germany) the following day in an accredited laboratory. Plasma was stored at −20°C until analysis.
End points
Hypoglycemic episodes were classified according to three glucose thresholds: <4 mmol/L (threshold indicated by the American Diabetes Association and the European Medicines Agency), <3 mmol/L (the commonly used threshold), and <2.2 mmol/L (detection limit of the CGMS). According to the CGM hypoglycemia definition used by the United Kingdom Hypoglycaemia Study Group, 10 a valid episode of nocturnal hypoglycemia lasted at least 20 min, and recovery was considered to have occurred once the CGM glucose level remained above the defined threshold for a further 20 min.
Statistics
Different methods for detection of agreement between PG and CGM measurements were used: 1. Sensitivity and specificity were calculated to evaluate the ability of detecting hypoglycemic nights by CGM: sensitivity=true positive/(true positive +false negative) and specificity=true negative/(true negative +false positive) according to the three thresholds for hypoglycemia. 2. Spearman's correlation coefficient ρ between PG and CGM glucose values was determined by linear regression analysis. 3. Bland–Altman analysis was done with PG as the reference. 4. The mean difference (MD) (MD=PG – CGM glucose value), mean absolute difference (MAD) (MAD=|MD|), and mean absolute relative difference (MARD) (MARD=MAD/PG) were calculated for all paired measurements and for glucose ranges of hypoglycemia (<4 mmol/L), normoglycemia (4–9.9 mmol/L), and hyperglycemia (≥10 mmol/L). 5. Continuous glucose error grid analysis (CG-EGA) (software from The Epsilon Group, Charlottesville, VA) was used to assess the clinical accuracy of the CGM sensors. The interdependency of successive data was taken into account by combining point accuracy (P-EGA) with rate accuracy (R-EGA). P-EGA reflects the difference between two paired samples at one point in time, and R-EGA is defined as the difference in glucose level between two consecutive measurements divided by the time interval between these measurements, which indicates the ability of CGM to follow the direction and tempo of the PG changes. In the CG-EGA matrix the CGM readings and corresponding PG values are divided into five zones (A–E) according to accuracy regarding PG changes. Zone A represents rates of change in CGM readings similar to PG rates, points in Zones B–D represent rates of change with increasing inaccuracy, and points in Zone E represent readings with a rate opposite to the PG rate. CGM readings are considered clinically accurate when falling into Zones A and B of both the P-EGA and R-EGA. Clinically benign errors are defined as those that are unlikely to result in clinically negative therapeutic consequences (i.e., points with acceptable P-EGA) (Zones A or B) but significant errors in R-EGA (Zones C–E). Clinically significant rate errors are those in Zones C–E on R-EGA, which could lead to serious decision errors in management. Points in these zones could prompt decisions that could result in PG levels outside the target range. Zone C (upper and lower) represents errors that would result in overcorrecting acceptable PG levels, Zone D (upper and lower) represents failure to detect hypoglycaemia, and Zone E (upper and lower) represents erroneous readings (i.e., inverse treatment should be administered
11,12
). 6. A Kaplan–Meier estimation of the cumulative probability of hypoglycemia-free nighttime according to PG was made.
Data from the CGM device were obtained from the files generated by the Medtronic MiniMed software. The distribution of data was tested with the Kolmogorov–Smirnov test, and data were compared using paired t tests or standard nonparametric tests as appropriate (Wilcoxon signed ranks test). Continuous variables were expressed as mean±1 SD or median (range) if the variables were not normally distributed. One-way analysis of variance and multiple comparison tests applying Bonferroni's correction were conducted in order to test differences in MARD and MAD and calculated on logarithmic values; MD could not be analyzed in this way because of the occurrence of negative values. The level of statistical significance is P<0.05 (two-sided). Calculations were performed using statistical software (SPSS version 20.0.0 for the Macintosh; SPSS Inc., Chicago, IL).
Results
In total, 217 nights with valid data was obtained in the completing 72 patients. Patient characteristics are shown in Table 1. Eighteen nights were missing because of CGM failure to log data, and 53 nights were missing because of patients failing to return for the scheduled visits. All participants were sleeping with the device during venous blood sampling. No device-related adverse events were reported.
BMI, body mass index; HbA1c, glycosylated hemoglobin.
Occurrence of nocturnal hypoglycemia
Prevalences of episodes of nocturnal hypoglycemia according to simultaneously measured PG and CGM values and the three thresholds are shown in Table 2. An analysis including all CGM glucose values measured 15 min before and after hypoglycemic events detected by PG did not change the CGM hypoglycemia prevalence results (data not shown). Fifty-three percent of the patients experienced at least one hypoglycemic night with PG <4 mmol/L, 25% were hypoglycemic with PG <3 mmol/L, and 8% of patients experienced at least one hypoglycemic night with PG <2.2 mmol/L. Twenty-eight percent of the nights were hypoglycemic (PG <4 mmol/L). The largest risk of experiencing a hypoglycemic episode existed at bedtime. Thus, patients went to bed at 23:00 h being hypoglycemic in 18 (8%) of the nights, whereas the occurrence of hypoglycemia was almost evenly distributed throughout the rest of the night. The duration of nocturnal hypoglycemia (PG <4 mmol/L) was skewed, with a median duration of hypoglycemia at 2 h and a mean duration of 2.7 h.
Plasma glucose (PG) was considered the gold standard.
CGMS, continuous glucose monitoring system.
Performance of CGM
In total, 1,786 PG values were correlated with simultaneous CGM measurements (slope=0.76, intercept=1.2 mmol/L; P<0.001). At 167 hourly time points of simultaneous measurement either a PG or a CGM value was missing (26 PG samples and 141 CGM readings). The Spearman's rank correlation coefficient was 0.82 (P<0.001) over the total range of measured values but only 0.32 (P<0.001) in the hypoglycemic range (<4 mmol/L). The Bland–Altman analysis showed that CGM underestimates PG at 67% of the readings in the total measurement range (1.0–27.1 mmol/L), corresponding to a mean difference of 1.1±0.1 mmol/L (95% confidence interval, 0.9–1.2) (P<0.001) (Fig. 1). In contrast, at PG <4 mmol/L CGM overestimates PG levels by 1.0±0.3 mmol/l (P<0.001). MAD was lower at hypoglycemia than at normoglycemia (P<0.03) and hyperglycemia (P<0.001) (Table 3). MARD was 45% in the hypoglycemic range, which was higher than in the normo- or hyperglycemic ranges (both P<0.001) (Table 3). CG-EGA showed an overall clinical accuracy of 56.4% (Zones A and B) in the hypoglycemic range (PG <4 mmol/L), 98.6% in the normoglycemic range (PG 4–10 mmol/L), and 92.8% in the hyperglycemic range (PG>10 mmol/L) (Fig. 2). The sensitivity of CGM according to the three thresholds was 65%, 40%, and 17% with a specificity of 80%, 94%, and 97%, respectively (Table 2).
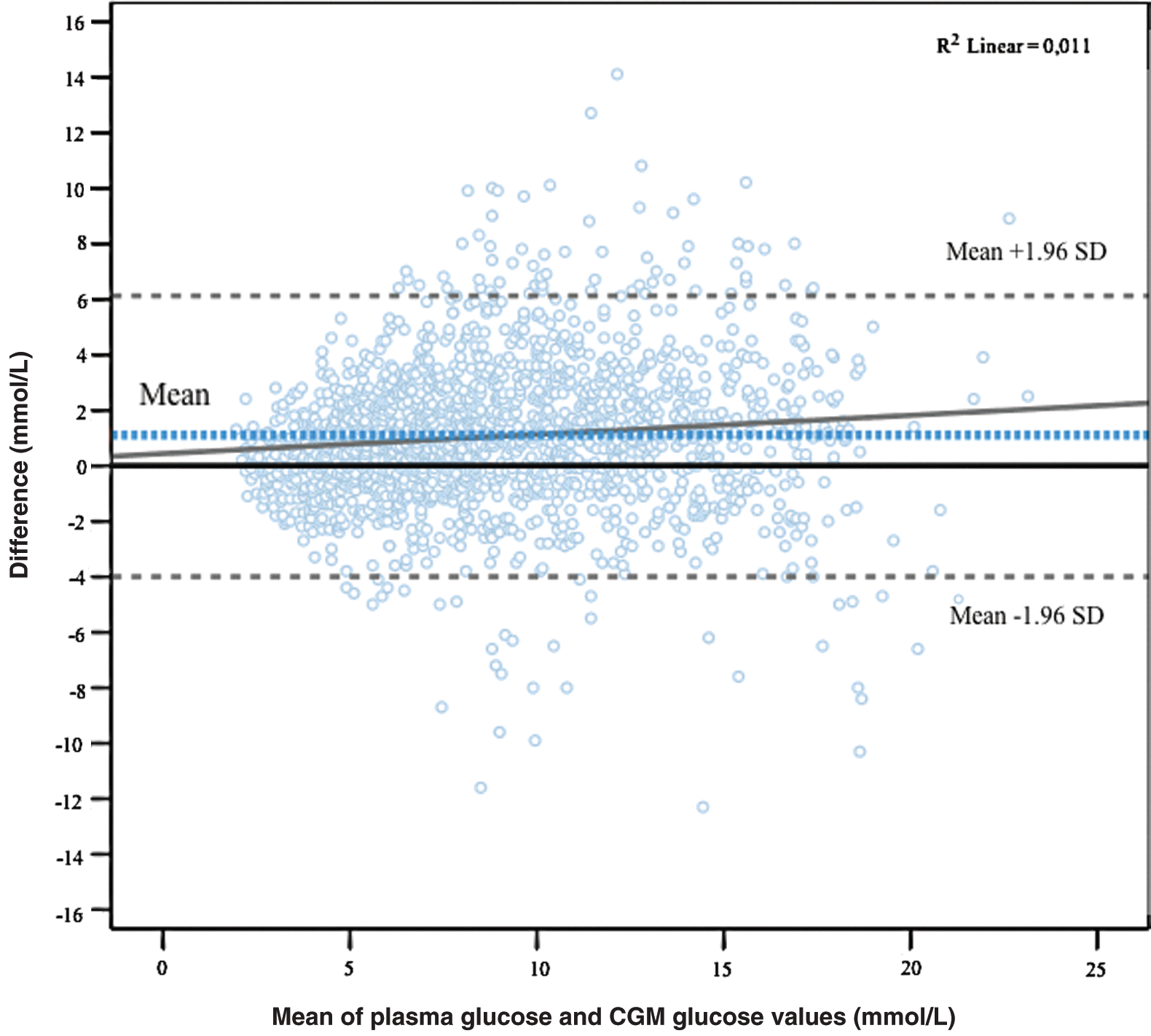
Bland–Altman plot enabling detection of a tendency for the variation of continuous glucose monitoring (CGM) glucose to change with the level of plasma glucose. Differences between plasma glucose and CGM glucose are plotted against the mean of both methods. Limits of agreement are indicated, and the horizontal dashed line “Mean” illustrates the mean difference. (Color graphics available online at

Continuous glucose error grid analysis combining rate and point accuracy stratified by glucose range. PG, plasma glucose.
CI, confidence interval; MAD, mean absolute difference (mmol/L); MARD, mean absolute relative difference (%); MD, mean difference (mmol/L).
Discussion
We assessed the clinical reliability of nocturnal CGM using the REAL-time CGMS with the Sof-Sensor in patients with type 1 diabetes at high risk of severe hypoglycemia and found that in contrast to at normo- or hyperglycemia, the accuracy of CGM was suboptimal in the hypoglycemic range. Only the highest tested threshold of 4 mmol/L resulted in clinically useful sensitivity in detection of nocturnal hypoglycemia.
The frequency of nocturnal hypoglycemia in our cohort, whether defined as <4, <3, or <2.2 mmol/L, corresponds well with reported results. 13 –15 In these studies blood glucose levels were also measured hourly during the night in patients with type 1 diabetes, but their previous experience with severe hypoglycemia and their state of hypoglycemia awareness are not stated. 13,14
Although the overall regression analysis showed good agreement between PG and CGM, the clinical accuracy of CGM in the hypoglycemic range was less good. CGM overestimated PG by 1 mmol/L in the hypoglycemic range <4 mmol/L. In accordance with this finding, a recent study reported that CGM overestimates glucose levels by 0.8±0.2 mmol/L in the hypoglycemic range <5 mmol/L. 16 This difference may have major clinical implications as CGM has become an increasingly common method for evaluation of overnight insulin requirements and an important tool for discovering otherwise undetected nighttime hypoglycemia. In accordance with previous studies, 17 we found that MARD in the hypoglycemic range was higher than in the total glycemic range. Zijlstra et al. 18 recently also reported that CGM was least accurate in the hypoglycemic range. In their study, including 2,317 paired data in 18 type 1 diabetes patients, CGM failed to detect more than half of the true hypoglycemic events (CGM <3.9 mmol/L). Both MARD and results of the Clarke error grid analysis were also comparable to our results. 18
The clinical accuracy of CGM has been investigated in various clinical settings using various sensors, making comparisons difficult. 4,9,17 –22 Because no consensus exists concerning reporting of the reliability of CGM, we choose to report several parameters of CGM performance. It should be emphasized that outcomes of testing CGM are highly dependent on the setting. 23 Results may vary between subjects with small oscillations in blood glucose levels to type 1 diabetes patients with much more fluctuating blood glucose levels. 19 Our patients probably represent the subset with the greatest glycemic instability. Accuracy also depends on the number of days on CGM. Thus, Day 1 of sensor wear, which was the day of interest in this study, has higher MARD than other days. 20,21 Moreover, the number of blood glucose calibrations and the equipment used (i.e., a home blood glucose meter versus a laboratory analyzer) influences accuracy. 23 Finally, but most importantly, accuracy metrics are highly dependent on variation of the blood glucose level, primarily the relative proportion of low glucose concentrations, and consistently demonstrate less reliability in the hypoglycemic range. 17,18,21,22
The major strength of our study is that we challenged the CGM device maximally by using it only single nights, with two calibrations on a home blood glucose meter, in type 1 diabetes subjects with fluctuating blood glucose levels even at night. This may have underestimated the reliability of the CGM. Nonetheless, our results are comparable to those of the study by Zijlstra et al., 18 even though they excluded type 1 diabetes patients with recurrent severe hypoglycemia (more than one episode within 12 months) and performed their study in-house for 9×2 days with calibration using a laboratory glucose analyzer every 4 h. Furthermore, our study is the first to be conducted on type 1 diabetes patients at particularly high risk of severe hypoglycemia who might be those benefitting the most from sleeping with real-time CGM. There are limitations in our study. First, because of technical difficulties complete CGM glucose readings were lacking in 8% of the nights (calibration errors, lack of signal between monitor caused by either an improper connection between the transmitter and the sensor, “lost sensor” alert or “weak signal” alert). Previous studies have reported rates of sensor failure or malfunction up to 18%. 24 Second, noncompliance during the last visits may indicate that the study setting was too inconvenient or time-consuming for some of the patients. Finally, we only had PG samples drawn hourly to minimize disturbance of the patient's sleep, which we compared with the corresponding single CGM glucose value. CGM might have detected hypoglycemia a few minutes before or after this single point of comparison. However, an analysis including all CGM glucose values 15 min before and after hypoglycemic events missed by CGM did not change the hypoglycemia prevalence results.
In conclusion, the reliability of CGM in patients with type 1 diabetes at high risk of severe hypoglycemia is comparable to that previously reported in patients without this problem. This implies rather low accuracy and overestimation of glucose levels in the hypoglycemic range. Absolute values of CGM recordings of nighttime hypoglycemia should therefore be interpreted with caution in clinical practice. CGM detected the majority of the nocturnal hypoglycemic episodes <4 mmol/L as indicated by our data. The point accuracy in the hypoglycemic range was suboptimal, resulting in the need for a relatively high threshold of 4 mmol/L or above to obtain a clinically useful event sensitivity in detection of nocturnal hypoglycemia, at the expense of specificity. Improved predictive algorithms in the newer generations of CGM may compensate for some of the lacking point accuracy and thereby improve event accuracy. CGM may still be useful as a research tool to document nocturnal hypoglycemia in a much more detailed manner than PG. However, firm definitions of hypoglycemia in terms of threshold and duration are important. Continued efforts to refine the CGM technology with more sophisticated predictive algorithms and improved sensor performance as reported for the Veo calibration algorithm 25 and the Enlite glucose sensor 21,22 are needed. Studies specifically addressing the reliability of the new sensor generations in the most likely candidates for chronic sensor use, namely those prone to severe hypoglycemia, are warranted using standardized study designs and metrics to allow comparisons of different CGM systems.
Footnotes
Acknowledgments
C.B. received research grant support from The Research Foundation of Hillerød Hospital. The staff at the outpatient diabetes clinic, Endocrinology Section, Hillerød Hospital, and at Steno Diabetes Center, Gentofte, are acknowledged for their cooperation during the patient recruitment phase and for careful handling of patients and data. Medtronic Denmark A/S provided Guardian REAL-Time continuous glucose monitors for the study.
Author Disclosure Statement
U.P.-B. has received lecture honoraria from Medtronic Denmark A/S but has not received reimbursements, fees, funding, or salary from any organization relating to the content or the preparation of this manuscript. C.B., P.L.K., L.T., and B.T. declare that they have no competing financial or other interests related to the preparation or the content of the manuscript.